Approach to neck lump thyroid lumps and cancers












 Calcitonin (if suspect")



 – Young, irradiation, FAP, Gardner’s syndrome, Cowden")
 and Hürthle cell cancer – Middle age –")



 PTH")


- Slides: 26
Approach to neck lump, thyroid lumps and cancers, and parathyroid disorders MRCS teaching 01 September 2015
Current Surgical Therapy: Evaluation of the isolated neck mass by Philip, Smith et al
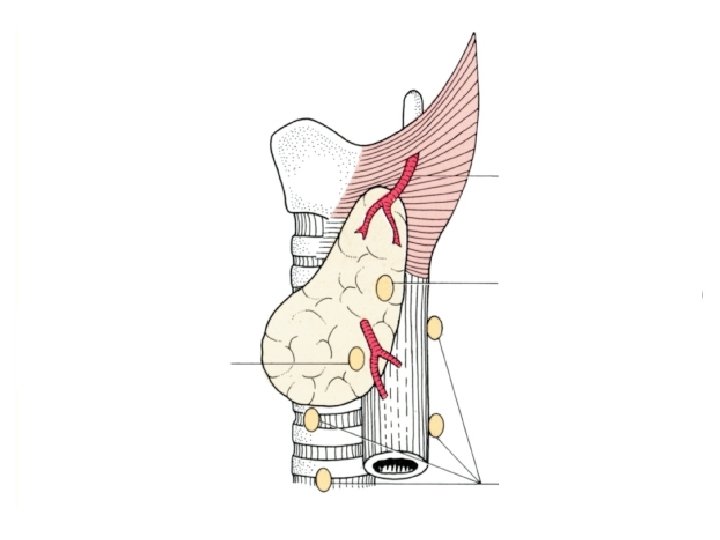
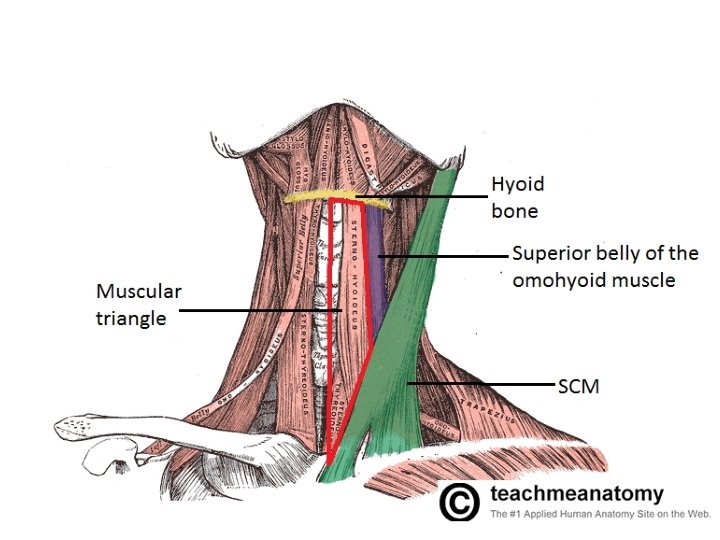
Clinical Anatomy: Applied Anatomy for Students and Junior Doctors by Ellis and Mahadevan
Clinical Anatomy: Applied Anatomy for Students and Junior Doctors by Ellis and Mahadevan
Current Surgical Therapy: Evaluation of the isolated neck mass by Philip, Smith et al
Differential diagnosis • Congenital, inflammatory, neoplastic • 2 -9% of head and neck cancers present as cervical masses without a known primary • Up to 80% of neck masses that occur outside thyroid are neoplastic in adults over age of 40 years Current Surgical Therapy: Evaluation of the isolated neck mass by Philip, Smith et al
History Age Personal or family history of malignancy Smoking/tobacco use or heavy alcohol Sun and radiation exposure Persistent mass, dysphagia, hoarseness, neurologic deficit, epistaxis, radiating pain • Constitutional symptoms • Rapidly developing tender masses are often infectious/inflammatory • Prior treatment/surgery • • • Current Surgical Therapy: Evaluation of the isolated neck mass by Philip, Smith et al
Surgery At A Glance, Fifth Edition, by Pierce and Niel
Current Surgical Therapy: Evaluation of the isolated neck mass by Philip, Smith et al
Imaging • Chest X-ray/CT thorax • Ultrasound scan – Hyper or hypoechogenicity, cystic degeneration, punctuate calcifications, unclear borders with surrounding structures perinodal oedema • CT scan – Invasion or distortion of normal anatomy – If thought to be nodal metastasis, can identify primary source in 20% • MRI – Presence of invasion into surrounding structures especially vascular or neural structures • PET – Not first-line – Metastatic squamous cell carcinoma of unknown primary – Further workup for known diagnosis Current Surgical Therapy: Evaluation of the isolated neck mass by Philip, Smith et al
Tissue diagnosis • • FNA Core biopsy Excision biopsy Panendoscopy and biopsy – Laryngoscopy, bronchoscopy and esophagoscopy – Biopsy – Tonsillectomy (tonsils are found to be the primary source in 20 -40% of these patients) Current Surgical Therapy: Evaluation of the isolated neck mass by Philip, Smith et al
Thyroid
Work-up • • Thyroid function test Serum Tg (not initial evaluation) Calcitonin (if suspect MTC) Ultrasound – Ill-defined borders, microcalcifications, internal vascularity, absence of colloid halo sign, hypoechogenicity, suspicious lymph nodes • • FNA Radionuclide thyroid scan (if TSH subnormal) CT/MR neck/PET Nasopharyngolaryngoscopy Current Surgical Therapy: Management of Thyroid Nodules Cooper, David S, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association (ATA) guidelines taskforce on thyroid nodules and differentiated thyroid cancer. Thyroid 19. 11 (2009): 1167 -1214.
National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology: Thyroid Carcinoma Version 2. 2013
Current Surgical Therapy: Management of Thyroid Nodules
Thyroid carcinoma • • • Papillary thyroid cancer Follicular cancer Hürthle cell cancer Anaplastic cancer Medullary thyroid cancer Lymphoma
Thyroid carcinoma • Papillary thyroid cancer (80%) – Young, irradiation, FAP, Gardner’s syndrome, Cowden disease, Wegener’s syndrome – Lymph node spread – Total thyroidectomy + neck dissection if any of: • age <15 or >45, radiation history, known distant metastasi, bilateral nodularity, tumour >4 cm, cervical LN metastasis, aggressive variant – Completion total thyroidectomy if • Tumour >4 cm, positive margins, gross extrathyroidal extension, macroscopic multifocal disease, confirmed nodal metastasis, vascular invasion – RAI – Surveillance with TSH, Tg, antithyroglobulin Ab and US National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology: Thyroid Carcinoma Version 2. 2013 Cooper, David S, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association (ATA) guidelines taskforce on thyroid nodules and differentiated thyroid cancer. Thyroid 19. 11 (2009): 1167 -1214.
Thyroid carcinoma • Follicular cancer (10%) and Hürthle cell cancer – Middle age – Blood spread – Total thyroidectomy if invasive cancer, metastatic cancer or patient preference • Central neck dissection if lymph node positive • Lateral neck dissection if clinically involved – Completion thyroidectomy if invasive cancer – RAI – Surveillance with TSH, Tg, antithyroglobulin Ab and US National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology: Thyroid Carcinoma Version 2. 2013
Thyroid carcinoma • Medullary thyroid cancer – MEN 2 – Serum calcium, calcitonin, CEA, pheochromocytoma screen, RET proto-oncogene – Total thyroidectomy + central neck dissection ± lateral neck dissection – Adjuvant EBRT • Anaplastic cancer – 10 year <1%, poor prognosis – FBC, calcium, TSH, CT/PET – Local disease: total thyroidectomy and selective resection of local/regional structures and lymph nodes – EBRT, chemotherapy, best supportive care National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology: Thyroid Carcinoma Version 2. 2013
Parathyroid
Primary hyperparathyroidism • • Most common cause for hypercalcaemia Excessive PTH production Incidence 1%, 2% after age 55 Women 2 -3 times more likely Single adenoma in 80 -85% Parathyroid carcinoma in 1% Present in nearly all patients with MEN 1 and 25% in MEN 2 A Current Surgical Therapy: Primary Hyperparathyroidism
Work-up • • • High or high-normal calcium Elevated or high normal (nonsuppressed) PTH Decreased serum phosphate Increased or high-normal chloride 24 -hour urinary calcium and creatinine – To rule out familial hypercalcemia hypocalciuria • Sestamibi scan • US neck Current Surgical Therapy: Primary Hyperparathyroidism
Indications for surgery • Symptomatic • Younger than 50 years old • Serum calcium levels over 1 mg/d. L above upper limit of normal (2. 8 mmol/L) • Creatinine clearance less than 60 m. L/min • Bone mineral density T score ≤ 2. 5 Current Surgical Therapy: Primary Hyperparathyroidism
Treatment • Minimally invasive parathyroidectomy with intraoperative parathyroid hormone monitoring – 50% drop in the intact parathyroid hormone level – Complication rate 1% • Bilateral neck exploration – Procedure of choice for MEN – Trachea-oesophageal groove, thymus, within thyroid, carotid sheath – Complication rate (including RLN injury) 4% Current Surgical Therapy: Primary Hyperparathyroidism