Approach to Motor Weakness Dr Rashmi Kumar Professor














 (late)")


 •")





- Slides: 24
Approach to Motor Weakness Dr Rashmi Kumar Professor, Pediatrics KGMU
Pathways Types of weakness Upper motor neuron Lower motor neuron Localization of lesion Patterns of weakness monoplegia hemiplegia paraplegia quadriplegia diplegia Cerebral palsy
MOTOR WEAKNESS: • Types & pattern • Anatomical localization • Etiology
History • Onset • Course • H/o fever • H/o seizures • Developmental milestones
Examination • Young child - ‘observation’ • Older child - ‘play’ § § § § Gait & Posture Muscle mass Tone Power Coordination Abnormal movements Reflexes –superficial & deep
Examination: Posture – – Frog leg Scissoring Decerebrate/decorticate/ophisthotonus Others Gait – – Foot drop Circumduction Limp Waddling
Examination: Muscle mass: • Compare 2 sides • Measure in relation to fixed points • in lower motor neuron • Slightly in upper motor neuron Muscle Tone • in LMN, cerebellar lesions • in UMN • physiological in newborn • frog leg position/scissoring Muscle power • maximum strength maybe impossible to test in uncooperative children • normal strength in pure cerebellar/basal ganglia lesions
Infant/toddler: ‘observation’ • definite hand preference before 2 yrs suspicious • hemiplegic arm flexed at elbow, movement, fisting with thumb adduction • asymmetric developmental reflexes • lift with hands under arms • traction
Older child: Quick assessment • hold arms over head • walk on heels & toes • get up from floor • run • hop on 1 foot • press arms against wall • squeeze finger • circumduction of thumb • formal testing
Types of motor weakness: • above anterior horn cell – UMN • below – LMN (final common pathway) UMN LMN M mass Slightly dt disuse · severely M tone spastic flaccid M power Distribution Individual Mm never affected Individual Mm maybe affected DTRs lost Babinski absent Superficial reflexes Lost (maybe regained later) lost
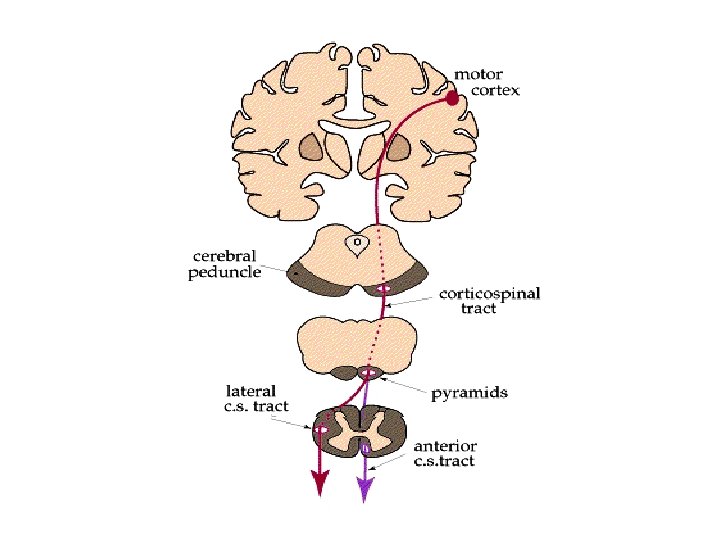
Localisation of lesion: UMN MOTOR CORTEX: • u/l weakness of opposite distal hand, leg or lower face • proximal muscles mb transiently weak • seizures mb+ • gaze palsies (area 8 inv) • aphasia (Brocas area –left side) • cranial nerves, trunk muscles not affected dt b/l innervation Internal Capsule: • • dense hemiplegia dystonia Midbrain • • ‘crossed’ paralysis ipsilateral IIIrd nerve + contralateral hemiplegia Pons • • • ‘crossed’ paralysis ipsilateral Vith/VIIth nerve palsy + contralateral hemiplegia Involvement of reticular activating system – altered consciousness
Localisation of lesion : UMN Medulla • ‘crossed’ paralysis • ipsilateral XII th nerve palsy + contralateral hemiplegia • Involvement of reticular activating system – altered consciousness Spinal cord • LMN signs at level of lesion • UMN signs below Acute destructive lesions of UMN hypotonia All cranial nerves have b/l representation except part of VII & XII
The Final Common Pathway
Localisation of lesion: LMN Spinal Cord lesion: • • • LMN signs at level of lesion + UMN signs below Acute lesions spinal shock recovery in few weeks Bladder & bowel involvement Anterior horn cell/ventral root/plexus lesions: • • Weakness in specific myotomes Slow degeneration of anterior horn cells fasciculations Peripheral Nerves: • • Single nerve lesion mononeuritis –weakness in distribution Polyneuritis: – – Distal weakness Early loss of reflexes – may not correlate with degree of weakness Neuromuscular junction: • Prediliction for ocular/pharyngeal or proximal muscles • Reflexes lost late in affected muscles Muscle: • Proximal weakness • Deep reflexes maybe but elicitable • Myotonia in some
LEVEL SC PN NMJ M Weakness ++ +/- + DTRs - (early) (late) Distribution upper level distal ocular+ proximal or patchy pharyngeal fasciculations + - (in chronic degenerative disorder) tone NCV n n EMG fibrillations , , fatigue pattern BSAPP amplitude of MUP
Patterns of Weakness: • MONOPLEGIA – weakness of a limb • Lesion often cortical, vascular in etiology • Sometimes, peripheral n lesion • • HEMIPLEGIA – weakness of upper & lower limbs on same side • Usually UMN • Lesion at cortex, internal capsule • Sometimes, brain stem/SC lesions Signs: • hand preference before 2 yrs of age • circumduction gait • asymmetrical reflexes • hemiplegic hand kept flexed at elbow, fisted with adducted thum Causes: • Hemiplegic cerebral palsy Migraine • Todds palsy Abscess • Tumour Granuloma • Trauma Vascular - Stroke : Sudden onset -- > gradual recovery
Stroke in Childhood Ischemic-sudden Hemorrhagic- severe headache, s/o ICT, meningeal signs Infections – PM, TBM, NCC, tuberculoma, VE, abscess o Vascular – AV malformation, aneurysm Hypertension Bleeding diatheses Vit K deficiency Cardiac – CHD, RHD, SABE o Collagen vascular disorders – SLE, PAN, APS o Hematologic – Sickle cell disease, leukemia, dehydration, iron deficiency, hypercoagulable states, o Metabolic Idiopathic - 'acute infantile hemiplegia' mb dt trauma to internal carotid
PARAPLEGIA: Weakness of both lower limbs • Lesion in SC or PN (polyneuritis) • UMN type – lesion in SC. If acute may spinal shock • LMN type - - lesion in lower SC eg. myelomeningocele - spinal shock stage - polyneuritis eg GBS, post diptheretic palsy - NM junction - Muscle
SPINAL CORD LESIONS: • I Compressive • Acute – trauma, epidural abscess • Chronic –tumour, vertebral disease, syringomyelia, arachnoiditis • • II Non compressive • Acute – TM, hematomyelia, infarction, infections, post infectious • Chronic – degenerative • -spinocerebellar degenerations • -spinal muscular atrophy • -motor neuron disease • -subacute combined degeneration Chronic lesions may present acutely dt secondary vascular changes
QUADRIPLEGIA- weakness of all 4 limbs · Deep coma · Lesions of brain stem Upper SC UMN signs · Polyneuritis All causes of paraplegia Craniovertebral malformations DIPLEGIA- weakness of both arms or both legs • Cerebral diplegia – a form of CP seen in premature babies
Cerebral Palsy: • MOTOR defect due to non progressive cerebral disorder acquired in early life • 2/1000 • Maybe associated with MR, seizures, hyperactivity etc. • • ETIOLOGY: • Prenatal- radiation, drugs, infections, malformations • Natal – LBW, trauma, asphyxia, ischemia • Post natal – kernicterus, neonatal illness, hypoglycemia, CNS infections • No cause found in ¼
Cerebral Palsy: • • • • • DIAGNOSIS: Delayed motor development Abnormal persistence of developmental reflexes Feeding problems TYPES: Spastic quadriplegia - most common - severe disability, MR - pseudobulbar palsy feeding problems - extrapyramidal signs - multicystic encephalomalacia Hemiplegia - related to perinatal events – PIH, ischemia stroke - porencephaly Diplegia - prematurity periventricular leukomalacia ·Dyskinetic – kernicterus, circulatory failure, asphyxia · Ataxic – often due to unrecognized cerebellar malformation
MANAGEMENT Multidisciplinary approach with involvement of neurologist, physiotherapist, speech therapist, occupational therapist Drugs to reduce tone , appliances