Approach to Hemorrhagic and Ischemic Strokes ACEP South



























- Slides: 35
Approach to Hemorrhagic and Ischemic Strokes ACEP South Dakota March 4, 2017 Marko Duic & Gaurav Puri
Objectives Classifying types of CVA Acute management Long-term management/treatment options
Types of CVA Ischemic CVA Hemorrhagic spontaneous traumatic
Ischemic CVA Causes: Embolic Thrombosis Dissection Vascular obstruction
Signs and Symptoms Transient or progressive symptoms: Visual symptoms Speech deficits Unilateral weakness Coordinations issues Vertigo Decreased LOC Other:
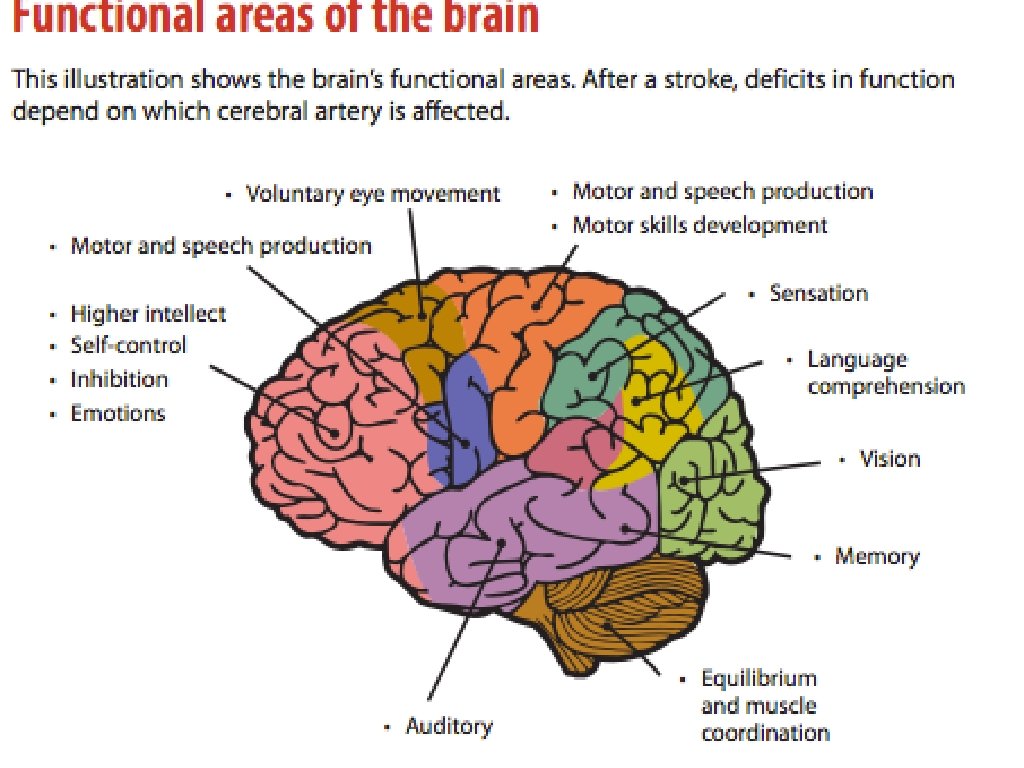
Deficits Are all strokes created? Location matters Why?
So you’re having a stroke…. . now what? Acute management: diagnosis first ABCs thrombolysis/stroke protocol antiplatelet antihypertensive other:
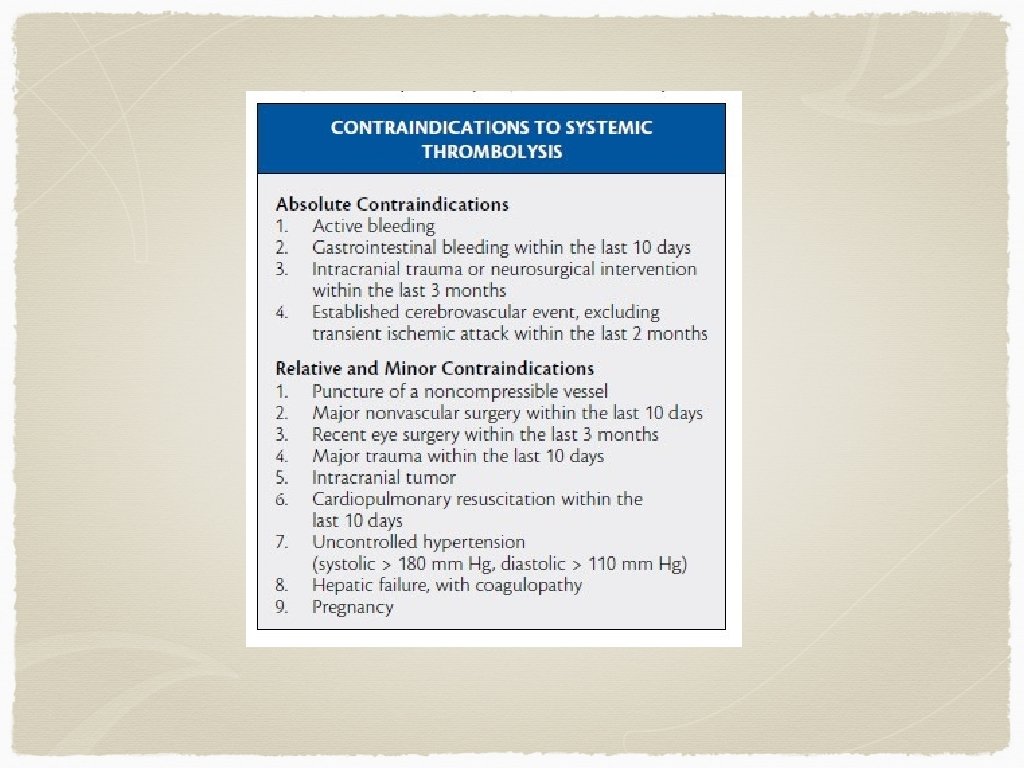
Diagnosis Clinical diagnosis initially If someone presents within the window for thrombolysis (3 -4. 5 hours), and does not have contraindications for thrombolysis, they should be transferred to a stroke centre for consideration of thrombolysis Controversial - why? Any other options?
Thrombolysis To date, roughly 12 trials examining thrombolysis with over 60000 patients 2 of 12 showed a benefit for thrombolysis unfortunately, both use nonstandard data analysis and reporting Several studies showed harm
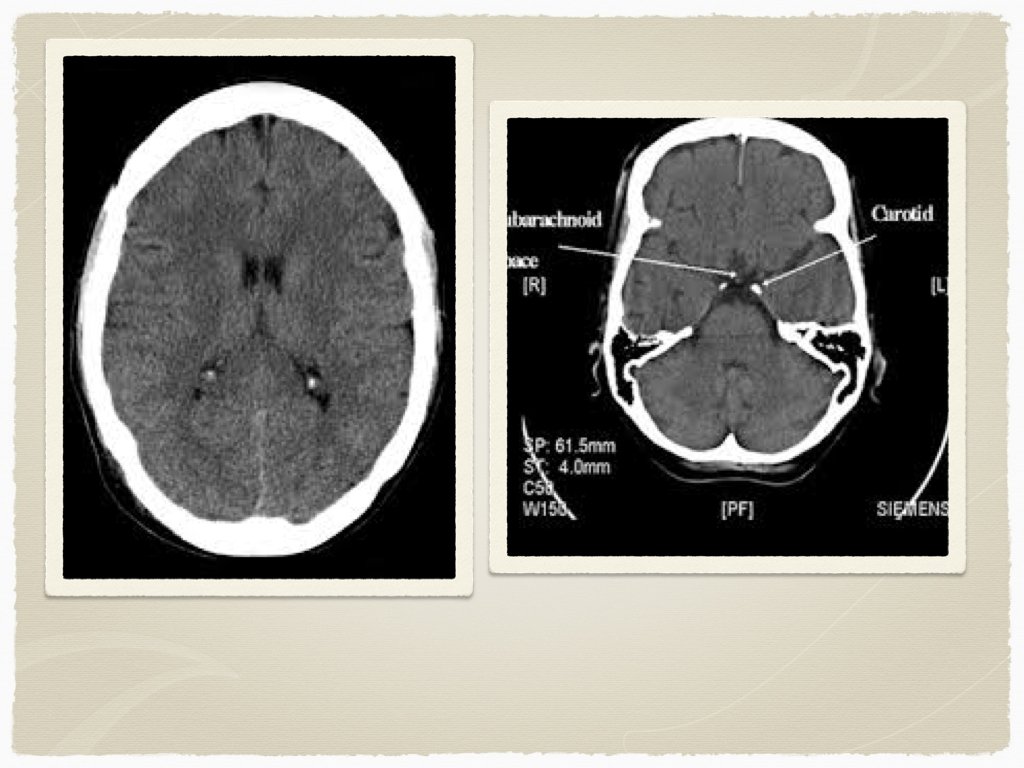
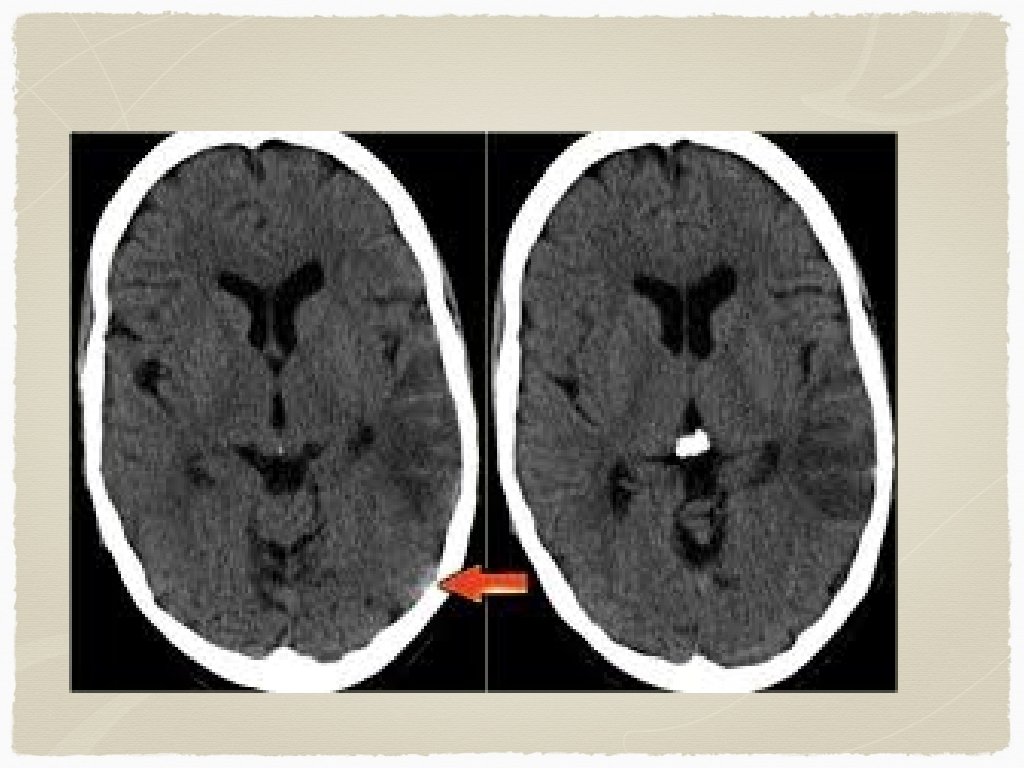
Outside of the window for TPA - Diagnosis CT head: findings? early vs late findings?
Treatment? Medical therapy Antiplatelet: ASA, Plavix
Antihypertensives For candidates of thrombolysis, target BP is less than 185 systolic and 110 diastolic For non TPA patients, blood pressure reduction is targeted at 10 -15% reduction Initial agents usually: Labetolol 10 -20 mg IV initially, can repeat, consider infusion Nitroglycerine Enalapril 1. 25 mg Nicarapine 5 mg/hr (can titrate to effect)
What’s the point of BP control? Need to match changes in ICP and CPP to ensure perfusion to affected area/collateral circulation Aggressive BP management can be harmful
Other treatment/diagnostics Bed position Cholesterol/blood glucose control Echo, holter, doppler, MRI
Questions?
Hemorrhagic CVA Bleeding secondary to: trauma aneurysm mass hypertension other
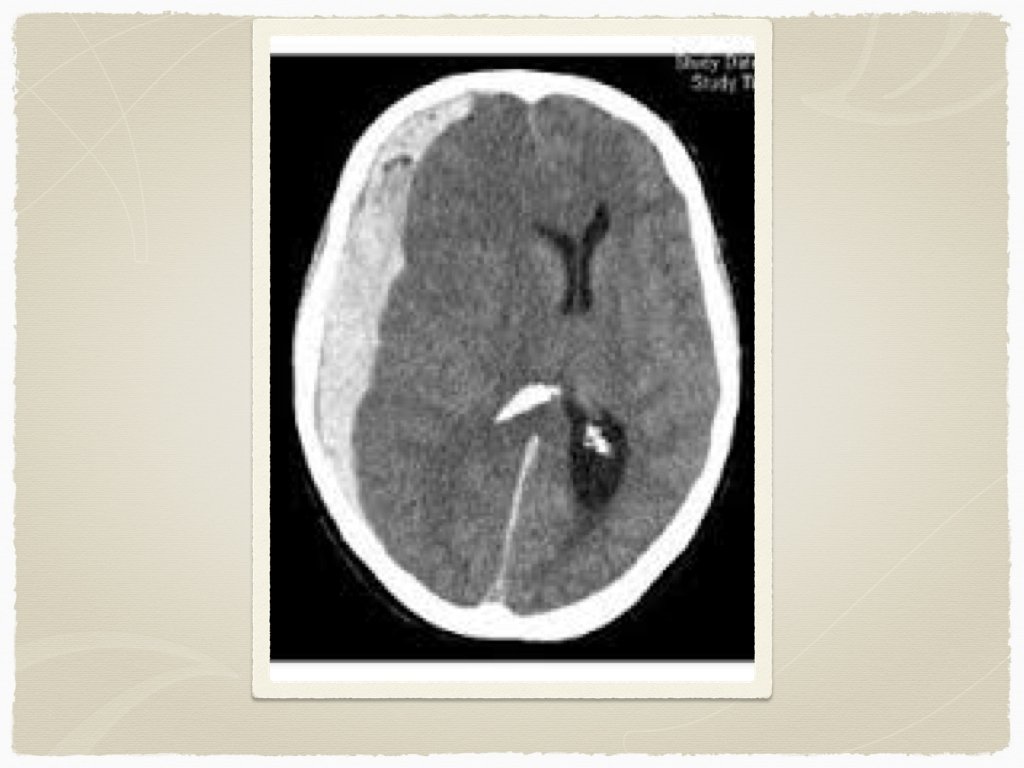
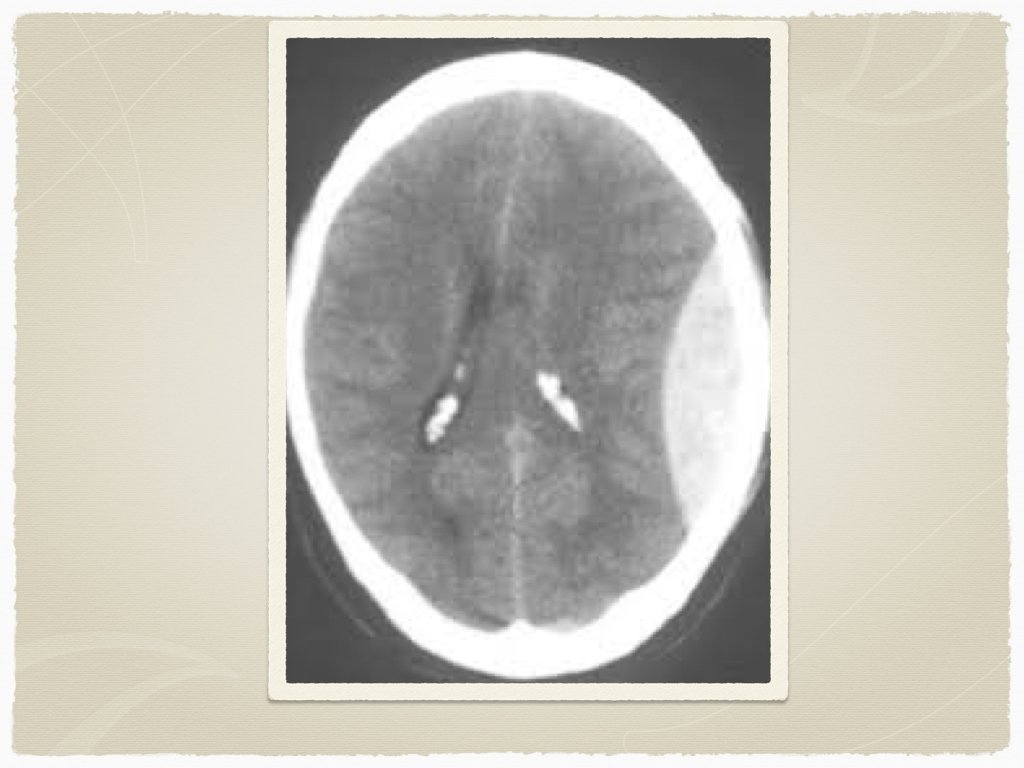
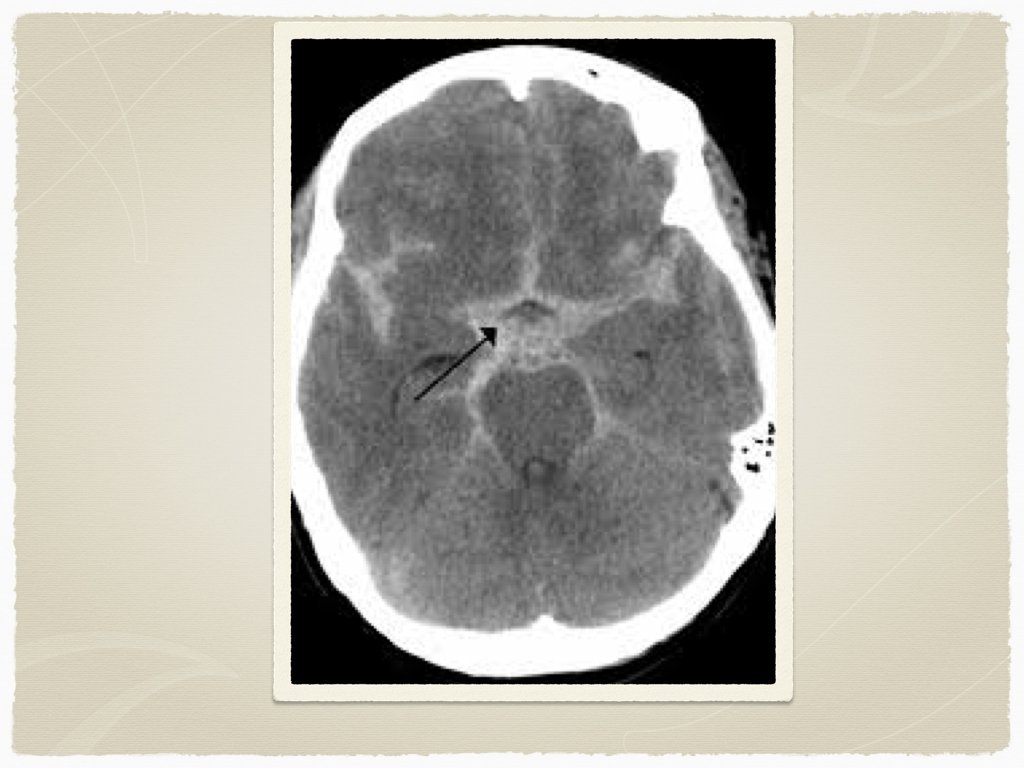
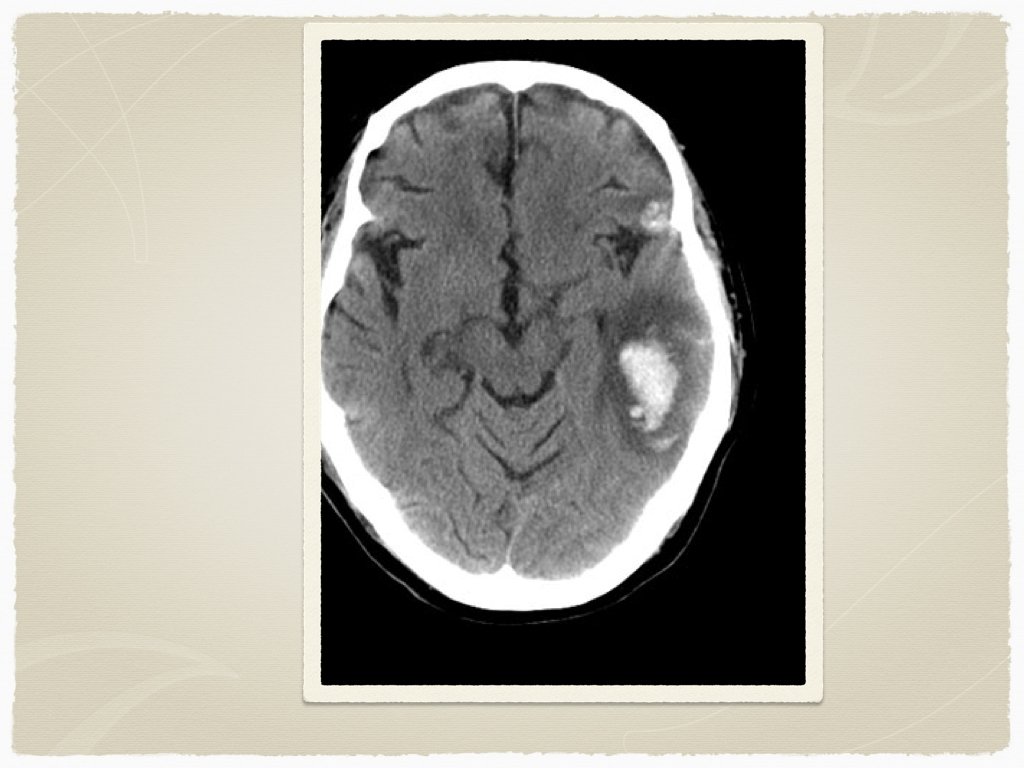
Types Subdural Epidural Subarachnoid Intraparenchymal Are all bleeds the same?
Signs and Symptoms Decreased LOC Obvious Trauma Pupil abnormalities Unilateral weakness Headache Elevated BP Low heart rate other:
Diagnostics CT is the initial test of choice In sentinel bleed for aneurysmal SAH, can be negative LP to follow if suspicion Lab work: INR Troponin ECG
Initial Management ABCs first If surgical bleed, consultation with neurosurgery for transfer Reversal of coagulation issues Tranexamic acid? Blood pressure management Anticonvulsants ICP management
Coagulation issues Oral anticoagulants Warfarin - Octaplex/beriplex, Vitamin K FFP Pradaxa - Praxbind Platelet dysfunction Hepatic failure - Vitamin K, FFP Renal failure - Platelets Heparin - protamine sulfate
Traumatic ICH Tranexamic acid - 1 g IV CRASH 2 trial - Early administration of TXA safely reduced the risk of death in bleeding trauma patients Administration beyond 3 hours of trauma is unlikely to provide benefit
Blood Pressure Management No clear guidelines/studies describe optimal BP levels in hemorrhagic CVA Significantly elevated BP may lead to rebreeding/hematoma expansion INTERAC 1 & 2 trials showed that early intensive BP control (less than SBP < 140) led to less hematoma expansion This was more important in patients on antithrombotic therapy Agent of choice was either labetolol, enalapril or nicardipine (can also use hydralazine in refractory cases) ATACH-II trial ongoing currently to assess outcomes with BP control less than 140 with nicardipine
Seizures in ICH Acutely, benzodiazepines can be used to stop an active seizure Dilantin load can be used to prevent further seizures Patients with ICH and seizure will likely require intubation and sedation Conflicting evidence for prophylactic anticonvulsants in ICH/SAH - more to come on this
Key concepts ICP - intracranial pressure CPP - cerebral perfusion pressure MAP - mean arterial pressure
ICP is usually elevated in ICH Elevation of the bed to 30 degrees improves venous outflow and decreases ICP No evidence for use of mannitol No evidence for use of corticosteroids - may result in complications
Questions?