APPROACH TO ABDOMINAL TRAUMA DR MOHAMMADZADEH TRAUMA Trauma

APPROACH TO ABDOMINAL TRAUMA DR. MOHAMMADZADEH

TRAUMA • Trauma is the most common cause of death for ages of 1 & 44 years

MECHANISMS OF INJURY • BLUNT TRAUMA • PENETRATING TRAUMA

BLUNT TRAUMA • Low - energy transfer: – struck with a club – falling from a bicycle – falls from short height • High-energy transfer: – auto-pedstrain accident – motor vehicle accident – motor-cycle accident – falls from heights greater than 20 feet

PENETRATING TRAUMA • Stab wound • Gunshot wounds – high-velocity injury(bullet speed > 2000 ft/s( – low-velocity injury • Shotgun wounds – close-range (< 7 meters( – long-range ( > 7 meters(
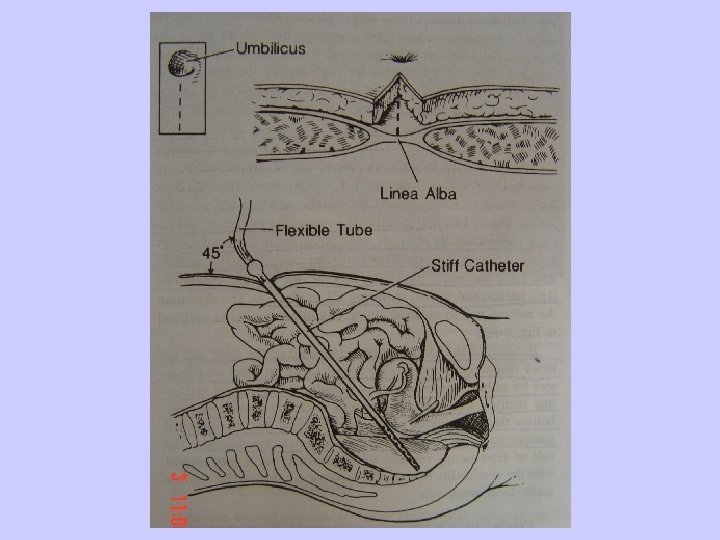

DIAGNOSTIC PERITONEAL LAVAGE DPL • The most sensitive test for determining of intraabdominal injury • POSITIVE TEST • • • Aspiration of more than 10 ml of free blood RBC greater than 100, 000/ml Detection of bile, vegetable or fecal materia ALK. PH>3 IU/L & Amylase> 20 IU/L Effluent draining from a chest tube, NGT, Fo

INDICATION OF DPL • • • Equivocal physical exam Unexplained shock or hypotention Altered sensorium(e. g closed-head injury( General anesthesia for extra abdominal proc Cord injury

ADVANTAGES OF ULTRASOUND • Noninvasive • Dose not require radiation • Useful in the resucitation room or emergency department • Can be repeated • Used during initial evaluation • Low cost

DISADVANTAGES OF ULTRASOUND • • • Examiner dependent Obesity Gas interposition Lower sensitivity for the fluid <500 ml False-negative retroperitoneal and hollow viscus injuries

ADVANTAGES OF CT-SCAN • Adequate assesment of the retroperitoneum • Nonoperative measurment of solid organ injuries • Assesment of renal perfusion • Noninvasive • High specifity

DISADVENTAGES OF CTSCAN • • • Specialized personnel Hardware Duration: helical versus conventional Hollow viscus injuries Cost

INDICATION OF CT-SCAN • • Blunt trauma Hemodynamic stability Normal or unreliable physical examination Mechanism : duodenal and pancreatic trauma

CONTRAINDICATION OF CT-SCAN • • Clear indication for exploratory laparotomy Hemodynamic instability Agitation Allergy to cotrast media

DECISION MAKING FOR BLUNT ABDOMINAL TRAUMA Overt peritonitis Hemoperitoneum LAPARATOMY

HIGH-ENERGY TRANSFER DPL POSITIVE LAPAROTOMY NEGATIVE OBSERVE

LOW-ENERGY TRANSFER stable v/s Unstable v/s CT-SCAN DPL Major solid organ Hollow viscus LAPAROTOMY Minor solid organ OBSERVE
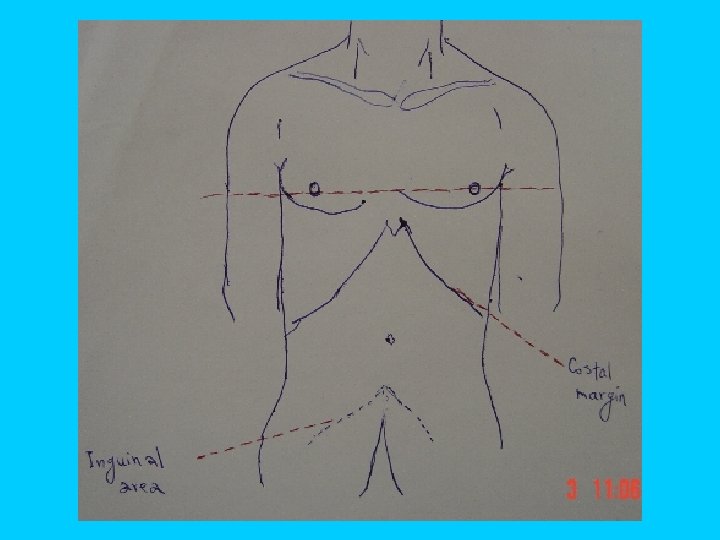

STAB WOUND TO LOWER CHEST AREA Exploration of wound for diaphragmatic injury - DPL - Thoracoscopy

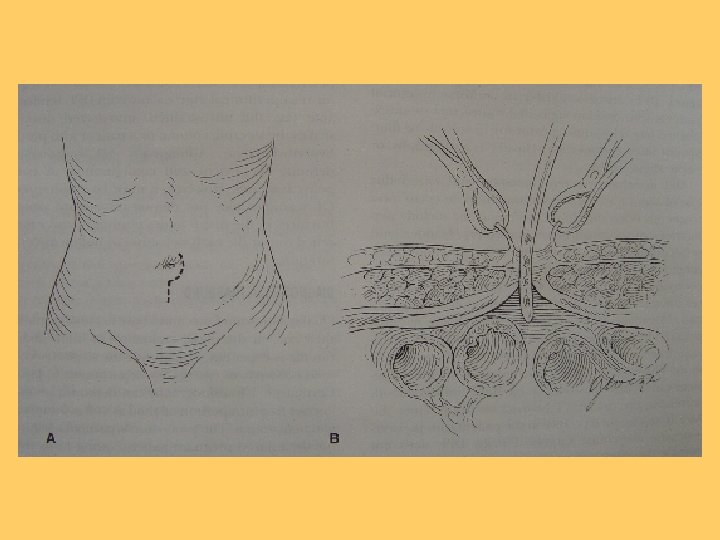
STAB WOUND TO ANTERIOR ABDOMEN Fascia intact D/C HOME Local wound exploration Negative Fascia violated Observation DPL Positive Laparotomy

STAB WOUND TO BACK AND FLANK Frequent examination DPL Triple contrast CT -scan

GUNSHOT WOUNDS Peritoneal violation Laparotomy Positive Gunshot wounds Equivocal DPL Negative Superficial Observe

SHOTGUN WOUND Close-range Similar to gunshot Shotgun wound Long-range Abdominal X-ray AP and lateral
- Slides: 24