Applications of Particle accelerators in Europe Royal Academy
 RADIATION TREATMENT")












")





. OAR 1 OTV = remainder of body")











 vs. Intensity Modulated X-rays (IMXT) 7 (field) IMPT")



- Slides: 41
Applications of Particle accelerators in Europe (Royal Academy of Engineering, London, 2015) RADIATION TREATMENT Bleddyn Jones MD Gray Laboratory, CRUK/MRC Oxford Centre Department of Oncology University of Oxford & CERN, Geneva
Radiation Treatment • 30 -40% die of cancer; up to a half of these patients are given radiotherapy • around 10 -15% population given radiation for cancer therapy. • Radiation given either to cure (overall cure 40%. . . in some instances it is 90 -95%), or palliate cancer (symptomatic relief). • Radiation is only around 12% of cancer budget in NHS, but it is frequently now given as part of multimodality approach … surgery+chemotherapy+radiation
The technology has improved, but how is it applied? What are the pitfalls? Choose your operator well.
Legal Requirements • Dose delivery to around 1% accuracy with good reliability; not as high as aero-engines; • radioprotection of workers and patients when machine is in off and on mode. • No absolute legal requirement to test effects of new treatments in tissues…. . but some countries monitor outcomes • Pharmaceutical Industry has strictly enforced requirements exist for animal testing etc……with costs borne by Industry.
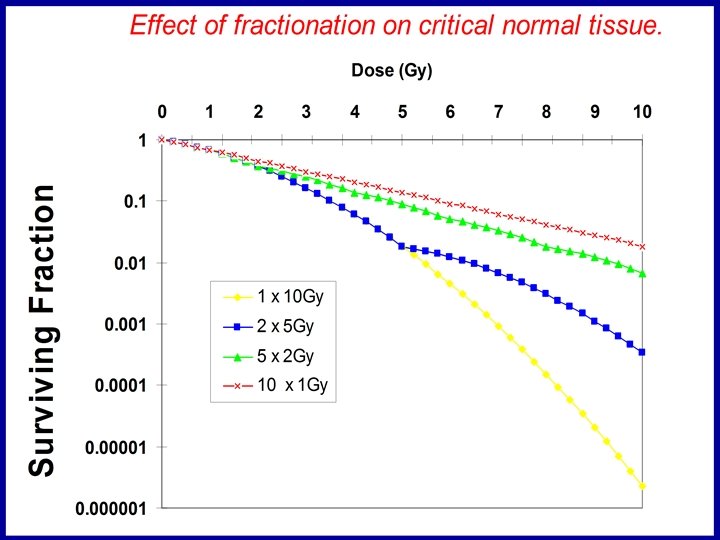
Radiation Biology • Study of radiation effects on living systems, from DNA, membranes, to cells, tissues and organisms, and their modification in time. • Non Linear effects : models for application • Different qualities of radiation behave differently – ionisation density independent of dose, dose rate etc.
Skin of patient treated with low voltage x-rays to large doses 23 years previously; she also developed cancer of the hypopharynx; NOTE FULL DOSE TO SKIN
Before and after radiotherapy; superficial tumours were treated this way with low voltage 50 -150 ke. V X-rays or later with 4 -10 Me. V electrons; since the full dose is given to skin chronic scarring and new vessel formation is seen years after “succesfull” treatment
Development of Cancer Radiotherapy • 1895 : Konrad Rontgen’s Xrays • 1898 - Marie Curie’s Radium • Radium and x-ray machines used to treat cancer very quickly • Most current radiotherapy uses High energy X-ray beams from linear accelerators or ‘linacs’ • These X-ray beams pass through entire thickness of body Modern Linac
Standard radiotherapy technology
Parallel opposed fields: note ‘hot areas’ in red: increase in proportion to tissue separation (thickness) and reduce with increased beam energy
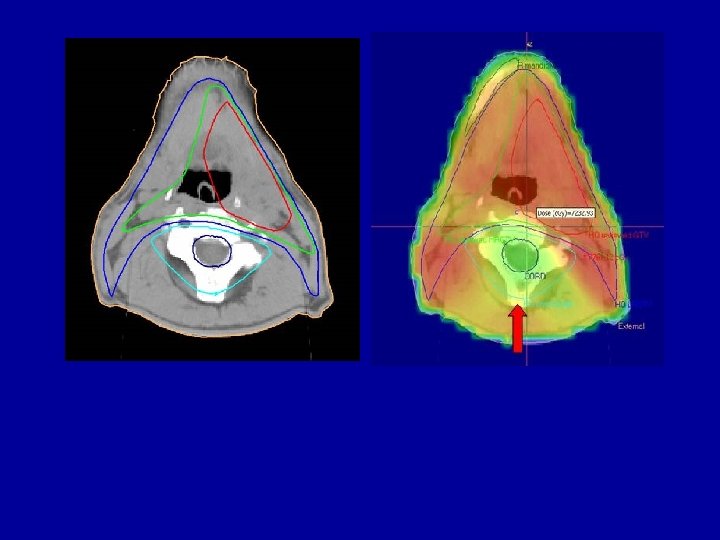
Conformal RT dose distributions
Radiotherapy - IMRT RT 3 D-CFRT Parotide glands IMRT Optimised beams to deliver the prescribed dose with maximum sparing S. Manolopoulos of the healthy tissue
IMRT modes S. Manolopoulos
Stereotactic Multiple Arc RT (SMART)
Equipment – MV era Linacs • • • • Metropolitan- Vickers in UK, then Phillips, Varian in USA, Siemens in Germany Compton scattering Pair production increase >10 Me. V and secondary Neutrons in rooms 20 Electron build up equilibrium at depth of 1 -3 cm, proportional to energy Depth dose increase and reduced dependency on skin as limiting tissue Tangential effects Longer SSD…even better Depth dose. Reduced penumbra compared with short SSD radiations and lower energies Take away target – use electron beam therapy for superficial cancers. . skin, breast, superficial lymph nodes often as boosts…. energy dependency roughly range=MV/3 in cm. MV energies resulted in increase indications for cancer treatments, particularly cancers in deeper anatomical locations e. g. pelvis. Safety issues: feedback on output; flattening of beam, dose homogeneity; regular QA checks, servicing replacement of parts; downtime>5% unacceptable… 1% preferred; to achieve 0. 01% would incur additional costs Each machine is unique, has to be characterised, outputs documented and fed individually into planning software systems. Run up each day: checks, before clinical use…starts often 6 -30 onwards for clinical start at 9 -00 AM. Output ~1 -2 Gy/min [Gy = 1 J Kg-1
Equipment – MV era Linacs • • • IMRT, portal imaging etc Couches (360 rotation and elevation) Gantries (360 rotation) Pit beneath couch…. can increase treatment distance to cover larger targets. Robotics Collimators Arcing PC controls Cost Working life: staffing ratios Servicing maintenance
Isocentricity: use constant distance from treatment source to isocentre –a defined {x, y, z} point within tumour target Set up P 1 % Depth dose inversely proportional to source skin distance for divergent beams, so before computers used in depth calculation a constant source skin distance was preferred X cm P 2 Distance of P 1, P 2 and P 3 to isocentre is constant = x cm Set up accuracy better than previous system of constant source to skin distance; also faster. P 3
Variants of Linac • Standard • Electron mode : remove target – electron range approx Me. V÷ 3 in cms. Scatter is problem and dose calculation more uncertain; volume narrows with depth. • Conformal- 3 D: shaped collimators • IMRT: non uniform fluence across fields • Tomotherapy: rotating linac • Radio. Surgery: multiple rotating arcs pointed at same isocentre • Cyber. Knife: robotic controlled linac arm
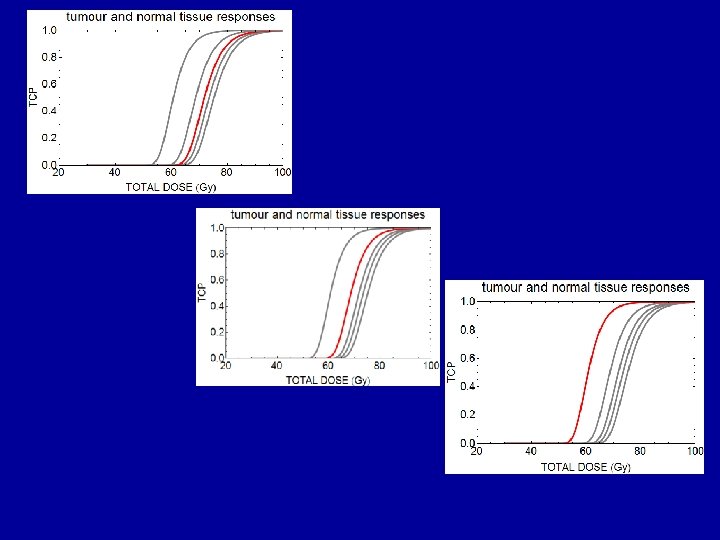
X-ray radiotherapy Basics Usage • Effect is related to the physical radiation dose, and the increased sensitivity (inability to repair damage) of tumour cells • X-ray radiotherapy delivers many lethal events per cell Probability • Approx 40% of cancer patients receive radiotherapy • This consumes approx 5 % of the cancer budget • Of the patients who are cured, approx – 50% is by surgery – 40% by radiotherapy – 10% by drugs TCP • NTCP 50 60 70 80 Dose / Gy BUT Most cured patients need ALL of these treatments
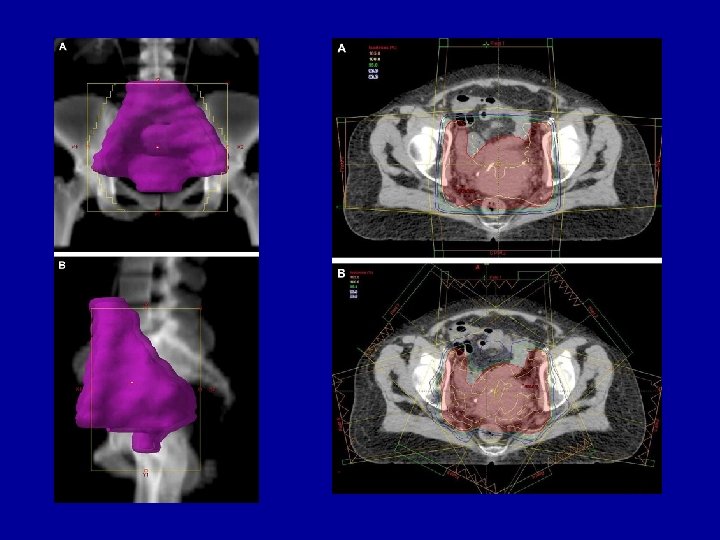
Conventional Target Volumes around a cancer (red). OAR 1 OTV = remainder of body GTV Gross tumour volume GTV CTV PTV OAR 2 CTV Clinical target volume contains normal tissue PTV Planning target volume contains normal tissue OAR = Organs at Risk – within CTV, PTV and OTV
Normal tissue volumes which have to be treated
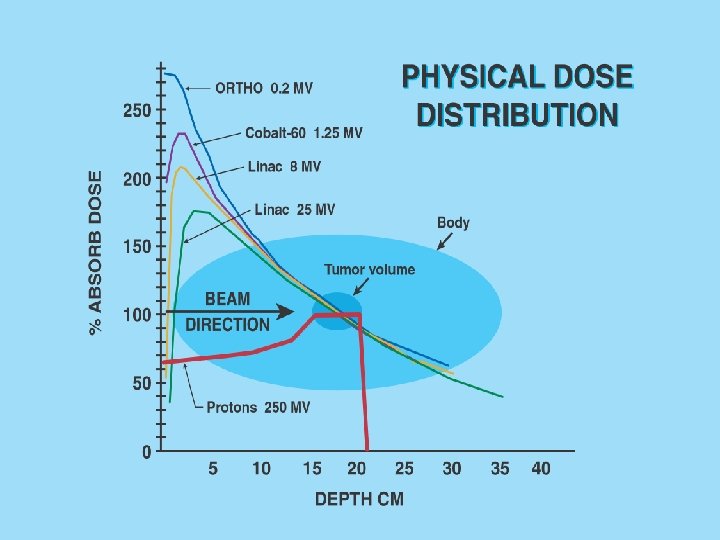
Comparative aspects of different therapeutic beams in medicine x-rays neutrons protons Attenuation with depth Pseudoexponential Bragg Peak Bragg * Peak ** Bragg Peak*** Integral biological dose highest lower lowest Average RBE 1 3 1. 1 1. 4 3 Oxygen modification factor 2. 5 -3 1. 5 -1. 8 2. 4 2. 3 1. 7 -1. 8 * refer to relative peak dimensions helium ion carbon ion
Three Disappointments in Radiation Therapy • -ve Pi mesons – ‘event size’ too large – fragmentation + primitive imaging of tissues/tumours • Fast Neutrons……RBE inversely related to dose, bio-effect relative to photons increases with depth • Brachytherapy…. when dose rate increases were unmatched by a reduction in dose (UK early 1980`s). ALL due to a lack of appreciation of how radiation interacts with biological systems in 3 -D space.
Brachytherapy • Short Range Therapy : use of radioisotopes in or near to a cancer. • Inverse square law allows very high cancer dose & lower normal tissue doses in 4 geometry (i. e. 3 -D) • Linear or circular/oval (ovoid) Ra sources applied into or adjacent to cancers. • Became acceptable alternative to radical surgery; gave highest cancer local control rates –c. 95% in 1920`s Cervix cancer Ra treatment
Afterloading machine…hollow. metal or carbon fibre tubes placed in patient; radiation loaded from this machine by compressed air and single source has calculated dwell times to deliver prescribed dose to target volume
Cervix cancer – modern CT planning views of applicators for HDR brachytherapy
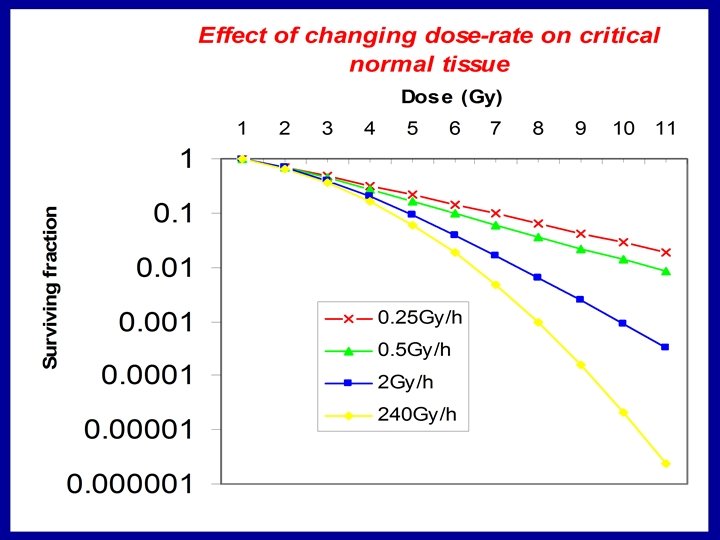
The 137 -Caesium Dose Rate was 1. 5 -2 Gy hr-1 compared with from Radium (0. 5 Gy. hr-1. ) JH Hendry had done experiments showing that a dose reduction of around 30% was necessary This was not followed High incidence of serious normal tissue damage followed Dose reduction later followed with reduction in morbidity.
Very High Dose Rate LINAC effects on tissues? Theoretical In Vivo Expts Depends on tissue/cells as to where flattening of effect occurs. Also, some earlier work in 1960 -70 s showed local oxygen depletion at very high dose rates M=marrow, G=gut, E=skin, L=lung…….
Radiation Biology is quantifiable and can be used to predict outcomes • Expected Lethal events per cell= • Surviving Fraction= • Tumour cure probability= • Repopulation term
Proton therapy in UK • 1989 first hospital based proton therapy at Clatterbridge, Liverpool, [converted fast neutron facility]. • >1700 patients with ocular melanoma; local control >98%. • First example of 3 D computer treatment planning in UK based on U/S reconstruction; use eye gaze direction to vary angle of eye relative to beam.
Japan: Tsukuba University New Proton Medical Research Centre, 2001
Spinal Sarcoma Intensity Modulated Protons (IMPT) vs. Intensity Modulated X-rays (IMXT) 7 (field) IMPT IMXT
Dose confirmation at required depth
Jouer avec le premier synchro-cyclotron + 3600 gantry de Meccano?
External Beam Therapy at the Present Time • Photons 1. Best dose conformity • Protons and ions 1. Best integral dose 2. Dose placement and RBE uncertainties 2. Dose rates 3. Optimum fractionation increasing remains to be 3. Optimum determined fractionation remains to be determined.