Application of CBT for Addiction and Recovery Dr

Application of CBT for Addiction and Recovery Dr. Kenneth Robinson, Ed. D. , President/Founder, Correctional Counseling, Inc. & Co-Developer of Moral Reconation Therapy - MRT® Slides may not be reproduced without written permission

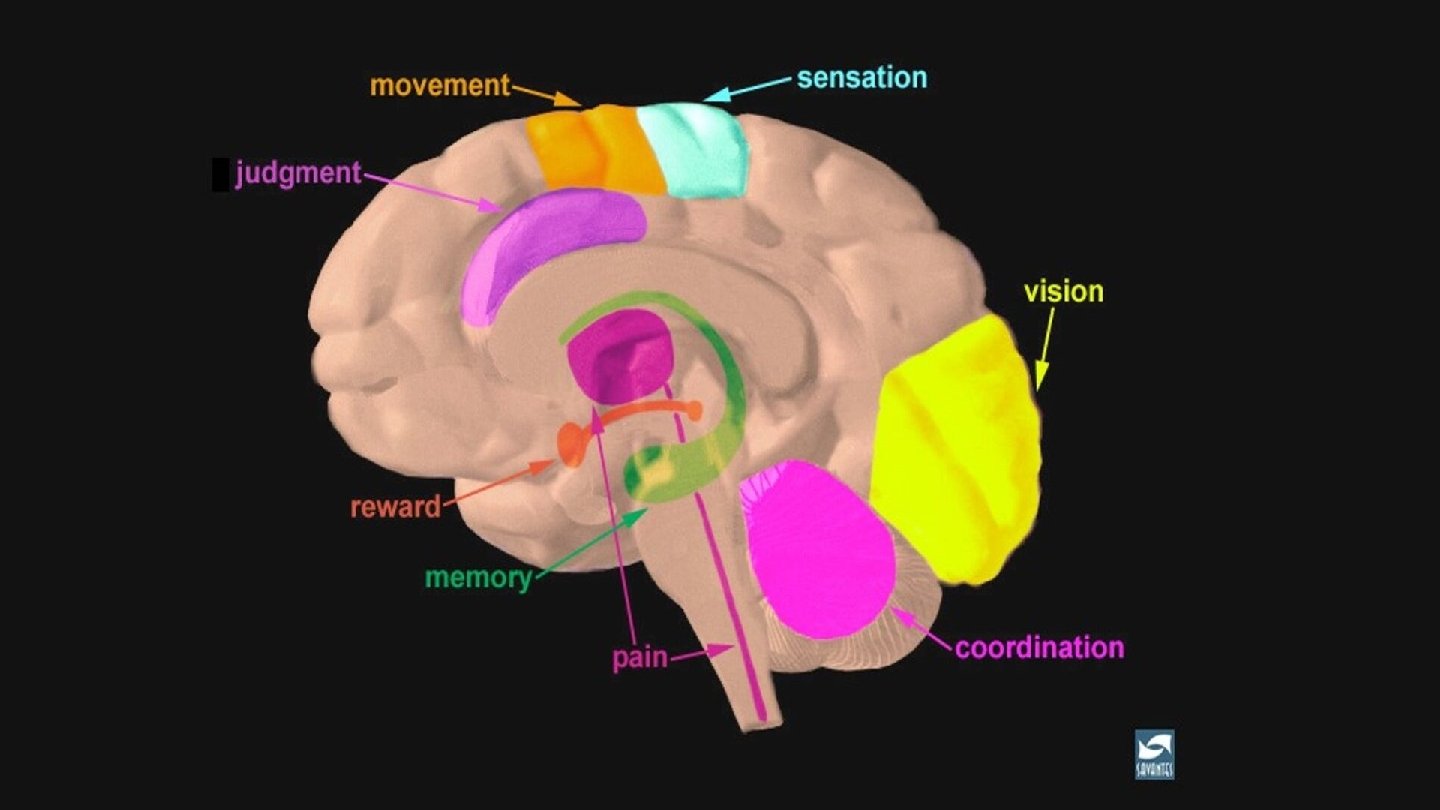
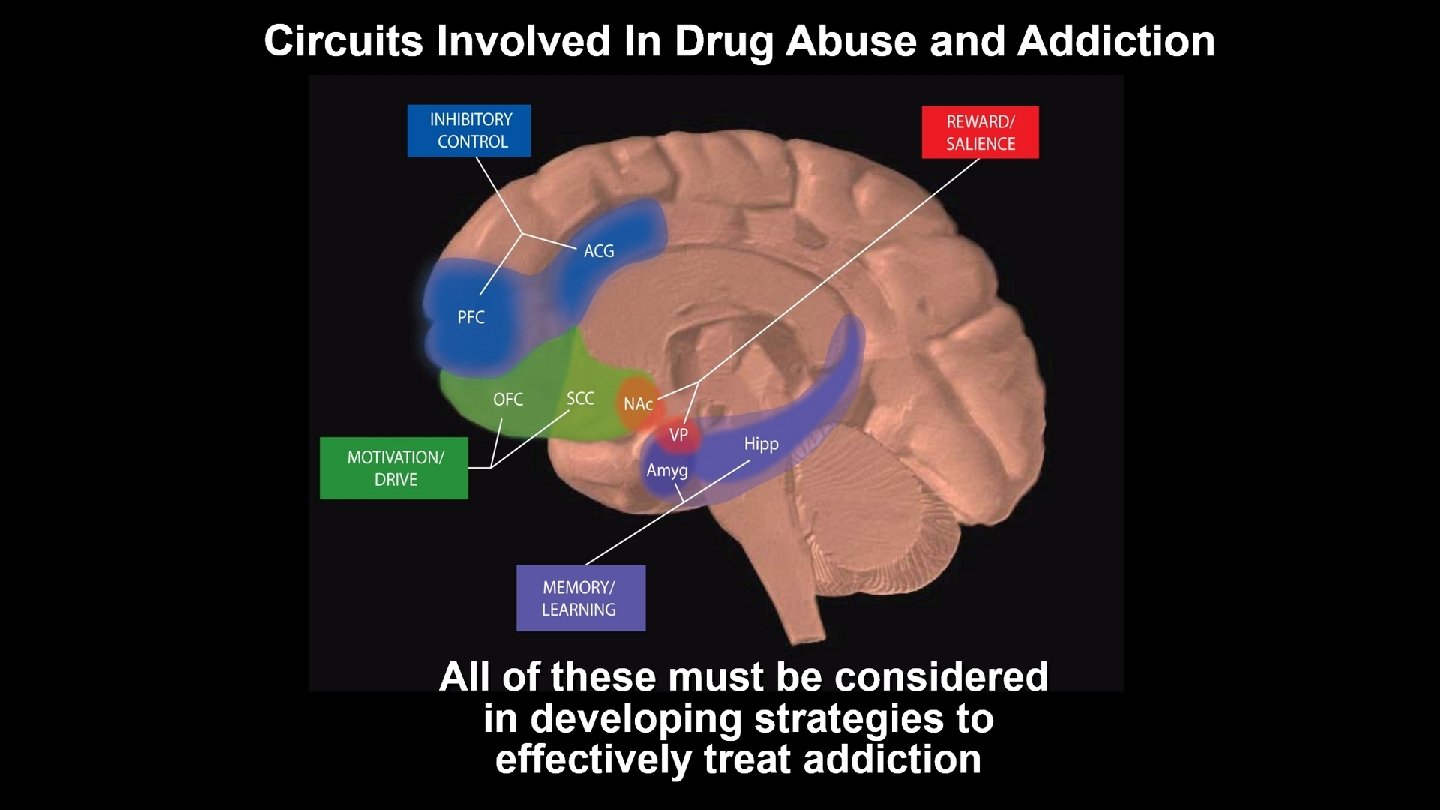
Biology/Genes Genetics Gender Mental Disorders Route of administration Effect of drug itself Environment DRUG Brain Mechanisms Addiction Early use Availability Cost Chaotic home & abuse Parents' use and attitudes Peer influences Community attitudes Poor school achievement

Addiction • A state in which an organism engages in a compulsive behavior �Behavior is reinforcing (rewarding or pleasurable) �Loss of control in limiting intake

ADDICTION AND BEHAVIORAL CHANGE: SUPPORTING PERMANENT RECOVERY • The impact of behaviors on addiction. Learn what research tells us about interventions that impact changing behaviors. • Factors critical to stabilize recovery from addiction. • Provide an opportunity to discuss the problem of sustained recovery for treatment court participants after graduation.

Things do not change, we do. HENRY DAVID THROEAU

DESIRED TREATMENT COURT OUTCOMES • Enhancing "real" abstinence • Creating permanent behavioral change • Sustaining post-program effects and reducing recidivism

ROOTS OF SUBSTANCE USE DISORDERS FOR TREATMENT COURT PARTICIPANTS • SUD History: Recent or Long Term • Criminogenic History: Degree and Frequency • Consequences of SUD on Participant • Consequences of SUD on others and community

WHY DO PEOPLE TAKE DRUGS? To feel go od To have novel: feelings, sensations, experiences AND to share them To feel better To lessen: anxiety, worries, fears, depression, hopelessness

IDENTIFYING THE PROBLEM Abuse of tobacco, alcohol, and illicit drugs is exacting more than $700 billion annually in costs related to crime, lost work productivity, and health care. Sources: https: //www. cdc. gov/features/costsofdrinking/index. html & https: //www. ncbi. nlm. nih. gov/pubmed/24455788
 • Behavioral self control")
STRONG EVIDENCE OF EFFECTIVENESS (CONSISTENT SUPPORT FROM NIDA CONTROLLED RESEARCH) • Behavioral self control training • Motivational enhancement therapies • Cognitive behavioral therapy • Self-help manual • Screening, Brief Intervention, Referral, and Treatment

DRUG PROBLEMS DO NOT OCCUR IN ISOLATION, BUT AS PART OF BEHAVIOR CLUSTERS • For adolescents, drug use occurs in conjunction with poor performance, precocious sexuality, anxiety, depression, and antisocial behavior. • For adults, drug use occurs with elevated rates of family discord, violence, health problems, unemployment, financial problems, homelessness, crime, injury, child abuse & neglect, disability, and mental health problems. • Interventions that target a broader range of life functioning are more successful in resolving drug problems.

DEFINING TREATMENT IN TREATMENT COURT • SUD Education Focus • Process Groups, Discussion Groups • CBT Evidence-Based Modalities • Trauma-Informed Treatment • Medically Assisted Treatment • Sustaining Treatment into Recovery

EFFECTIVE TREATMENT APPROACHES Many approaches have been tried in behavioral health interventions and attempts have been made to treat symptoms of these issues. To date, cognitive behavioral models have had superior results. SAMHSA lists Cognitive Behavioral Therapy as an evidence-based and promising practice.

Stages of Change Maintenance 50 Action Participant is successful in maintaining changed behaviors over time 40 Preparation 30 Contemplation Participant is actively engaged in changing behavior Participant is getting ready to make changes 20 Precontemplation 10 Not yet acknowledging that there is a problem behavior that needs to be changed 0 Item 1 Acknowledging that there is a problem but not yet ready or sure of wanting to make a change Item 2 Item 3 Source: https: //treatmentcourts. org/pluginfile. php/4810/mod_resource/content/1/Dr. %20 Mee%20 Leedoing%20 time%20 or%20 doing%20 change. pdf Item 4 Item 5 Deovers: Marketing 2020

MOTIVATIONAL INTERVIEWING Motivational interviewing is an evidencebased intervention designed to enhance client motivation for change.

COGNITIVE BEHAVIORAL THERAPY • Cognitive behavioral approaches are more structured and directive. • Cognitive behavioral approaches consistently appear to be the most effective treatment therapy for substance abusers. • Programs that include the cognitive component are more than twice as effective as programs that do not Source: (Gottfredson, 1997; Mackenzie, 1997; Mac. Kenzie et al; . , 1998; Andrews, et al. , 1995; Andrews & Bonta, 1990; Gendreau, et al. , 1993; Palmer, 1995)

Conation MRT - MORAL RECONATION ® THERAPY A term derived from the philosopher René Descartes to describe the point where body, mind, and spirit are aligned in decision making. "Reconation" then refers to altering the process of how decisions are made.

MRT FOCUS • Confrontation of beliefs, attitudes & behaviors • Assessment of current relationships • Reinforcement of positive behavior & habits • Positive identity formation • Enhancement of self-concept • Decrease in hedonism • Development of frustration tolerance • Development of higher stages of moral reasoning

• Open ended & Self-paced • Usable across systems • Encompasses a range of learning styles MRT UNIQUE PROGRAM ATTRIBUTES • Utilizes an Inside-Out process • Standardized curriculum provides facilitator structure and accountability • Program emphasizes feedback & student reflection • Enhances personal problem solving & selfdirection • Helps clients identify their individual strengths

• MRT is designed to be completed by the average client in 20 -30 sessions MRT CLIENT GROUP PROCESS • Completion is defined when the client successfully passes MRT's 12 th Step • However, Steps 13 thru 16 provide a loose structure for the search for sustaining change and identifying one’s life purpose. This allows for continued participation at their own pace of self discovery.

RECOVERY OUTCOMES AND TREATMENT COURT GRADUATION • Successful Treatment Court graduate: �Pre/Post Assessment results to confirm degree of change through treatment court participation �Readiness for graduation: criteria vs recovery �Determined on SUD treatment alone versus SUD Treatment and resolving critical needs

FROM TREATMENT TO RECOVERY The need for a shift from focusing on acute episodes of treatment to the management of recovery during longer periods of time, including continuing care, and linkage to mental health and wraparound services and other activities. Research indicates that the window of greatest vulnerability for relapse is the first 30 to 90 days following discharge from an index episode although an elevated risk of relapse can extend up to 2 years or more. Recovery is a developmental process, it doesn’t happen over night!

WHAT DO WE MEAN BY RECOVERY? • Substance Use Disorders are increasingly recognized as chronic relapsing conditions. • Aspects of recovery: health, mental health, coping responses, legal involvement, vocational involvement, housing, recovering peers, social and spiritual support. • “Sustained Abstinence”: 60% of people with lifetime substance use disorder eventually reach this state, or sobriety.

WHAT DO WE MEAN BY RECOVERY? • Duration of abstinence is associated with decreased crime and increased employment and income. • Abstinence is generally associated with being housed and having some friends.

ABSTINENCE VS SOBRIETY • Abstinence: a necessary first step in learning what to do to get and stay healthy in all areas of life • Sobriety: abstinence plus a return to full physical, psychological, social and spiritual health

CHARACTERISTICS OF RECOVERY • Resolving SUD issues; and maintaining sobriety • Understanding the roots of negative behaviors • Resolving problems internally; understanding external situations • Able to enter or return to positive living �Establishing support for recovery �Developing relationships; moving beyond past negative relationships �Resisting isolation; staying active �Returning to a normal life situation

COPING STYLES • Avoidance Coping Styles: cognitive avoidance, values correction and emotional discharge • Approach Coping Styles: logical analysis, seeking guidance, problem solving, seeking alternative rewards and positive reappraisal • Note: the duration of abstinence is associated with improvements in health, mental health and coping.

RISKS AND PROTECTIVE FACTORS • RISKS: Substance use among family, friends, and victimization. Activities involving drugs and/or alcohol. • Protective factors: Treatment and self-help participation, and peers in recovery. Sober living and positive activities. Support from “selfperceived strengths” (family, social peers and spiritual support).

POST-TREATMENT COURT SUCCESS FOR GRADUATES • Characteristics of graduates in Recovery: �Focus on future goals �Meeting needs for employment, housing, transportation �Creating positive relationships; discarding negative relationships �Participating in activities: for yourself and for others

POTENTIAL CHALLENGES TO INDIVIDUAL RECOVERY • Physical • Mental • Employment • Housing • Transportation • Expecting others will change because you are

ROOTS OF RECOVERY • Pre-program Assessment �Includes all elements of SUD history; potential mental health issues; criminogenic risk history �Applicable for Post-program assessment • Critical Needs and Strength-based Attributes �Identified and incorporated �Identified and not addressed • Individual Client Plans �Treatment plans �Socio-economic plans

CONTINUUM OF RECOVERY • Engagement: Internal and External • Treatment Effects • Transition to Self-Sustaining Recovery • Living in the Real World

Things do not change, we do. HENRY DAVID THROEAU

RECOVERY SUPPORT EFFORTS • Final stage of treatment should be relapse prevention • Sober Living: People; Places; and Things • Treatment court Alumni groups: success and challenges • Twelve step programs: safety with drawbacks • Private recovery groups • Organizations usually in urban areas, but could be formed anywhere, examples: �Center for Open Recovery, San Francisco, CA �Faces and Voices of Recovery, Washington, DC �Facing Addiction, Danbury, CT �Shatterproof, NY

WHAT IS BEING DONE IN YOUR COMMUNITY? • Do you prepare transition or sustainability plans for graduations? • Have you prepared a guide for graduates to reach out and support their continuing recovery? • Do you recommend specific self-guided material to continue client’s learning about recovery? • What are you doing, except waiting to see if they relapse!

NEED FOR MORE RESEARCH • Local treatment program managers need better information on activities that ensure recovery in their clients • Identifying and documenting research on Recovery to develop and/or confirm evidencebased practices • Gaining input from local program managers to identify best Recovery practices and practical, realistic approaches • Developing a system to disseminate “lessons learned” in promoting sustained Recovery

I was always looking outside myself for strength and confidence, but it comes from within. It was there all the time. ANNA FREUD

MRT and the Relationship to Recovery • Steps 1 -3 – Set the stage to see where the challenge is and where you are in the challenge – Steps 4 -6 – Begin to bring into view where you are in the relationship to others, what you view as important – And who you view as important as well as the importance of others in your life as well as the world/ – Steps 7 – 9 – Begin to assist in the development of the new you and the imporatnace of not giving up so quickly on yourself – Steps 10 – 12 – Ask you to take a hard look at yourself once again, look at relationships and then set new goals to achieve happiness. – Steps 13 – 16 – Bring the need to maintain the gain by doing things in the right way for the right reasons – By discovering your life purpose
 • Including age")
MEASUREMENT TO DETERMINE STAGE OF RECOVERY • Addiction Severity Index (ASI) • Including age of first use, date of last use, treatment history, and current service use. • Global Appraisal of Individual Needs (GAIN) • Scales related to SUD, mental distress and recovery environment • Perceived Family and Social Support Scales • Coping Response Inventory (CRI)

CONTACT US WE'D LOVE TO HEAR FROM YOU! ADDRESS PHONE 2028 Exeter Rd, Germantown, TN 38138 (901) 360. 1564 EMAIL FAX ccimrt@ccimrt. com (901) 757 -1995

Connect with us online! WEBSITE TWITTER FACEBOOK CCIMRT. COM twitter. com/CCI_MRT www. facebook. com/ twitter. com/Dr. Robinson. MRT Correctional. Counseling. Inc /
- Slides: 45