APNL Presents All About Trauma The Many Facets

APNL Presents: All About Trauma The Many Facets of Trauma

Themes for This Evening: • Introduction to Trauma by Marina E. Hewitt, R. Psych. • Early Childhood Experiences by Dr. Heather Sheppard, R. Psych. Presented by Dr. Megan Grant, R. Psych. • Post-Trauma Responses by Dr. Megan Grant, R. Psych. • The body remembers: Physiology of Trauma by Dr. Beatriz R. Rodriguez Rubio, R. Psych. • Trauma Symptoms and Diagnoses by Curt Hillier, M. Sc. , Registered Psychologist • Paths to Recovery by Dr. Megan Grant, R. Psych. • Pharmacological Management of PTSD by Dr. Cynthia Slade, MD, FRCPC

Introduction to Trauma Marina E. Hewlett, R. Psych.

What is Trauma? . • Trauma is caused by negative events that are stored in the brain and body and may affect how we feel, think, and behave. It affects how we see the world.

Facets of Trauma affects how we interact with the world.

Facets of Trauma is not about what is wrong with someone but about what has happened.

Facets of Trauma • Trauma can result in living the present through the past.

Facets of Trauma • Negative experiences and unmet developmental needs which undermine sense of: • self-worth; • safety; • ability to assume responsibility for self or others; • ability to control choices.

Facets of Trauma • Trauma comes in many forms and reactions are individualized.

Facets of Trauma • Stored memory – thoughts, – pictures, – sounds, – smells, – tastes, – emotions; and – body sensations.

FACETS OF TRAUMA Trauma and the brain’s pathways to healing • The Brain is : • oriented towards health • has a physiological information processing system that normally helps us to process our experiences adaptively.

Facets of Trauma Recovery • The Callery Tree , now known as the “Survivor Tree”, was discovered in the rubbles of Ground Zero following the terror attacks on September 11, 2001. The severely damaged tree was nursed back to health and now stands at the 9/11 Memorial as a living reminder of our shared strength in the face of trauma.

Early Childhood Experiences Dr. Heather Sheppard, R. Psych. Presented by Dr. Megan Grant, R. Psych.

Childhood matters • Childhood trauma can include – Abuse – Neglect – Parental mental illness/substance use – Parental incarceration – Parental separation – Family violence – Environmental disaster – War

Childhood Trauma is Common • 67% of us experience at least one of these traumas • 1 in 8 experience 4 or more. • Our developing brain is extremely vulnerable to toxic stress.

What are the impacts?

Our Body Remembers • Childhood trauma increases the rates of 7 of the 10 leading causes of death in our country (e. g. , heart disease, asthma, cancer) – With or without an increase in negative behaviours (e. g. , smoking) – Changes our DNA – Changes brain structure and function – Changes our immune system • Alters the impact of adult trauma

Our Thinking is changed • Our story – Safety, intimacy, trust, control – Self and other • Memory is changed – Trauma memory are tied together – neurocognitive,

Our emotions are changed • Reactions become more automatic • We get ‘stuck’ in an emotion – Fear – Anger – Numbness • Fearful of emotions – Dissociation – Emotions can become triggers

Our coping is changed • You survived. • Many of the tools and solutions we used to cope and survive become ‘stuck’, – They stay, even when we are safe – The solution may become the “problem”.

Are we doomed? • No but…. Often painful and frustrating to acknowledge role of childhood trauma in adult experiences • Power in understanding …. . – Why some things may be hard – Personal vulnerabilities • Informs treatment – Physical and mental health

Post-Trauma Responses Dr. Megan Grant, R. Psych.

Post-trauma Responses • Not everyone who experiences a traumatic event will develop lasting symptoms • Whether trauma symptoms develop/persist can be influenced by multiple factors related to the – individual experiencing the trauma – traumatic event – social context

Individual Factors • Greater likelihood of developing trauma impacts/symptoms has been associated with – – – – – Female gender Younger and older age (vs. middle age) Poverty / low SES Previous or coexisting psychological disorder Less functional coping styles Family dysfunction / family history of psychopathology Previous trauma exposure Dissociation / “shutting down” at time of trauma Greater distress at time of or immediately after traumatic event

Event Factors • Greater likelihood of developing trauma impacts/symptoms has been associated with events that Involve intentional acts of violence Present a life threat Cause physical injury Involve harming others (e. g. , combat), or witnessing death Loss of friend/loved one due to trauma Life-threatening illness (especially painful medical procedures/events) – Sexual victimization – Longer duration/greater frequency of traumas – Unpredictability and uncontrollability – – –

Social Factors • Social factors tend to be some of the most important in determining a person’s response to trauma • More positive outcomes tend to be associated with – Support from family, friends, and safe others – Accepting/non-blaming responses to talking about the trauma – Caring and nurturing responses from others – Availability of helpers/agencies • Public attitudes / prejudice toward some groups contribute to trauma response

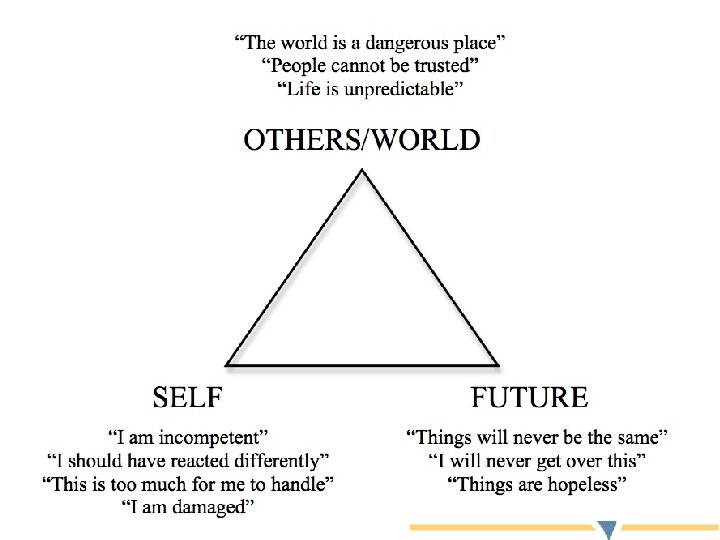
Impacts of Trauma • For those who experience symptoms, the impacts can be widespread • Many find that their beliefs are changed by their trauma – Beliefs about themselves – Beliefs about others/the world – Beliefs about the future

Impacts of Trauma • People who are impacted by trauma may find themselves having difficulties with – Relationships – Work, school, daily tasks – Leisure / personal interests – Substance use • Even though trauma can dramatically impact one’s life, post-traumatic growth is possible

The body remembers: Physiology of Trauma Beatriz R. Rodriguez Rubio, Ph. D. , R. Psych (Dr. Betty)

Trauma and the body • How does trauma get “stuck” in the body? – Part of PTSD is non-verbal it shows up when, at times, seemingly “for no reason” we feel extra jumpy or anxious or angry or numb. – This has to do with how our brain works:

Brain Basics • Frontal Lobe- involved in planning thinking, complex decision making, personality expression, and moderating social behaviour. In charge of language and logic. Thinks things through and can be slow • Limbic System: Doesn’t have language it is more concerned with basic survival motivations, kicks in quick, it is not too concerned with logic or reason. Two important parts within the limbic system: • Amygdala – Involved with emotions such as anger, fear, pleasure • Hippocampus – Involved in learning and memory
")
Response to Trauma (Fight, Flight, or Freeze)
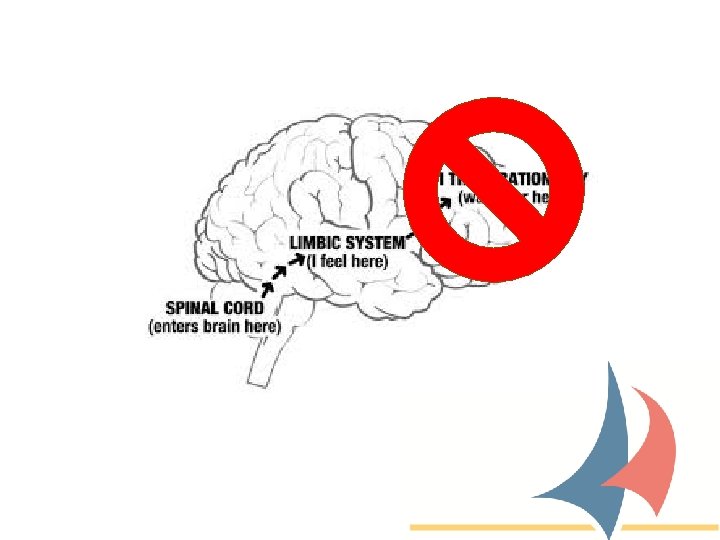

• Our brain has survival mechanisms that are trying to protect us, it doesn’t know that we are safe now. • One of the most important parts in healing is to restore a sense of safety. • And to be kind to ourselves, understanding that our limbic system is trying to protect us…. Don’t judge, attack, or “should” at yourself for normal reactions.

Trauma Symptoms and Diagnoses Curt Hillier, M. Sc. Registered Psychologist

Trauma Symptoms • Intrusion and re-experiencing trauma • Avoidance of trauma reminders • Negative changes in thinking and mood • Changes in arousal level

Intrusion and Re-experiencing Trauma • Intrusive distressing thoughts and memories of the trauma • Recurrent distressing dreams related to trauma • Flashbacks – feeling or acting like trauma is recurring • Intense psychological distress when triggered or cued to trauma • Marked physiological reactions when triggered or cued

Avoidance of Trauma Cues and Triggers • Avoidance of distressing memories, thoughts, or feelings about or closely associated with trauma • Avoidance of people, places, conversations, activities, objects, or situations that trigger distressing thoughts, memories, or feelings about trauma

Negative Changes in Thinking or Mood • Inability to remember an important aspect of the trauma • Exaggerated negative beliefs or expectations about oneself, others, or the world • Distorted thoughts about the cause or consequences of trauma that lead to blame of self or others • Negative emotional state (fear, horror, anger, guilt, shame) • Diminished interest or participation in significant activities • Feelings of detachment or estrangement from others • Inability to experience positive emotions

Changes in Arousal Level • • • Irritable behaviour and angry outbursts Reckless or self-destructive behaviour Hypervigilance – on guard, scanning for threat Exaggerated startle response – jumpy Problems with concentration Sleep disturbance

Diagnoses • Acute Stress Reaction • Acute Stress Disorder • Post Traumatic Stress Disorder

Further Resources • National Center for PTSD • PTSD Buddies

Paths to Recovery Dr. Megan Grant, R. Psych.

Paths to Recovery • The type of treatment received will depend on – Type of trauma and specific symptoms experienced – Individual needs – Availability and appropriateness of trauma-specific services • In general, treatment that addresses trauma will occur in phases – Phase 1: Education, Safety, Coping – Phase 2: Processing Memories – Phase 3: Engagement / Reconnection

Phase 1 • Client and therapist discuss consent, treatment and what is involved, education provided around rationale for treatment • Therapist assists client in developing an understanding of their symptoms • Coping skills and strategies are taught and practiced to promote safety between sessions and prepare for next phase of treatment

Phase 2 • The exact method used to process memories will vary depending on the orientation of therapist, the service being provided, and on client needs • This is often the most “intense” phase of treatment, but can also be one of the most meaningful for clients • Focus of this phase is to discuss memories in a way that will encourage – Normalizing client’s response to what happened to them – Developing new ways of understanding their trauma – Decreasing the intensity of emotion associated with the trauma memories – Decreasing avoidance of thoughts/memories related to the trauma

Phase 3 • This phase focuses on getting clients back to the life they want to be living • Treatment may focus on – Repairing relationships or forming new ones – Returning to work, hobbies, interests – Potentially developing a new sense of self – Ensuring clients have the knowledge/skills they need to maintain their health/well-being once treatment has ended – Supporting post-traumatic growth

Paths to Recovery • A client’s journey through these three phases is not always linear • The course that treatment is taking can be impacted by triggers, life events, new traumas, etc. • Finding a fit between client needs and a treatment approach that can be consistent yet flexible is key

Pharmacological Management of PTSD Dr. Cynthia Slade, MD, FRCPC March 13, 2018
 • “Comprehensive management of")
Canadian Psychiatric Association: Clinical Practice Guidelines for Managing PTSD (2006) • “Comprehensive management of PTSD should incorporate both psychoeducational and pharmacologic components. ”

Recommendations for Pharmacotherapy for PTSD First line Fluoxetine, paroxetine, sertraline, venlafaxine XR Second line Fluvoxamine, mirtazapine, moclobemide, phenelzine. Adjunctive: risperidone, olanzapine Third line Amitriptyline, imipramine, escitalopram Adjunctive: carbamazepine, gabapentin, lamotrigine, valproate, tiagabine, topiramate, quetiapine, clonidine, trazodone, buspirone, buproprion, prazosin, citalopram, fluphenazine, naltrexone. Not recommended Desipramine, cyproheptadine. Monotherapy: alprazolam, clonazepam, olanzapine.

• Response to an SSRI should be apparent within 2 -4 weeks. • Adequate trial length is up to 8 weeks at maximal, tolerated dose.

• Combination therapy with multiple agents early on is often seen to preserve and build upon gains made in treatment.
 • LTM is often needed. • Approximately 25% of patients with")
Long-Term Management (LTM) • LTM is often needed. • Approximately 25% of patients with PTSD who responded to treatment relapsed within 6 months of discontinuing medications. • It is suggested that those patients with chronic PTSD continue medications for at least one year. • Benefits have been shown to accrue with LTM. • Improvement in psychosocial functioning tends to lag behind symptomatic improvement, highlighting the need to continue medication well after symptoms remit. • Many patients will require LTM to prevent relapse.

Thank you! Questions? If you would like to seek treatment please go to: http: //www. apnl. ca/find-apsychologist/
- Slides: 56