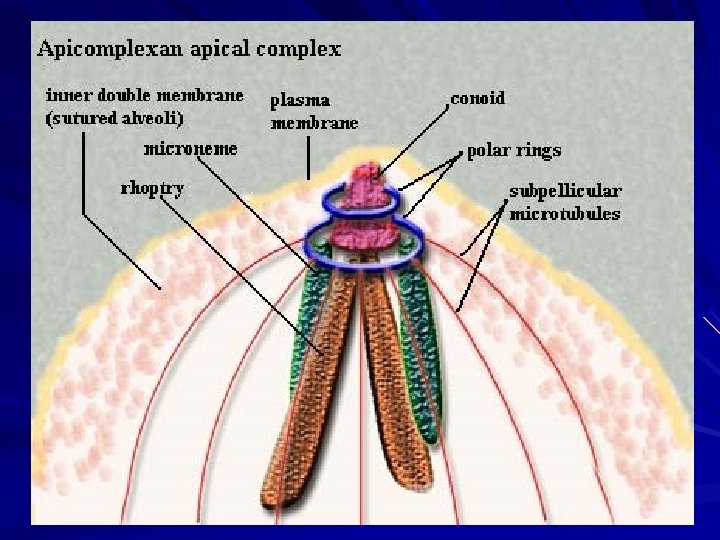
Apicomplexa structure Phylum Apicomplexa Class Sporozoea Subcl Coccidia

Apicomplexa structure

Phylum: Apicomplexa Class : Sporozoea Subcl. : Coccidia Order : Eucoccidiida Subor. : Eimeriina (Tissue & Intestinal Coccidia) Family : Eimeriidae Cryptosporiidae Sarcocystidae Genus : Isospora Cyclospora Species: Cryptosporidium Sarcocystis Toxoplasma belli cayetanensis parvum hominis natalensis hominis suihominis gondii

Intestinal Coccidia 1 -Isospora belli Causal Agent: Infects the epithelial cells of the small intestine, and is the least common of the three intestinal coccidia that infect humans. Geographic Distribution: Worldwide, especially in tropical and subtropical areas. Infection occurs in immunodepressed individuals, and outbreaks have been reported in institutionalized groups.

Morphology Oocyst form: Average size 30μm in length by 12 μm in width Mature oocyst Immature oocyst Stained oocyst

Life Cycle of Isospora belli

Symptoms -Infections often are asymptomaticand self-limited. -Symptomatic Infection include; - acute, non bloody diarrhea - malabsorption syndrome - Severe diarrhea - Eosinophilia may be present (differently from other protozoan infections ). .

Pathogenesis - Villous atrophy commonly associated with malabsorption Syndrome. -It will be remembered that this condition is also seen at times in giardiasis

Pathology of Isosporiasis

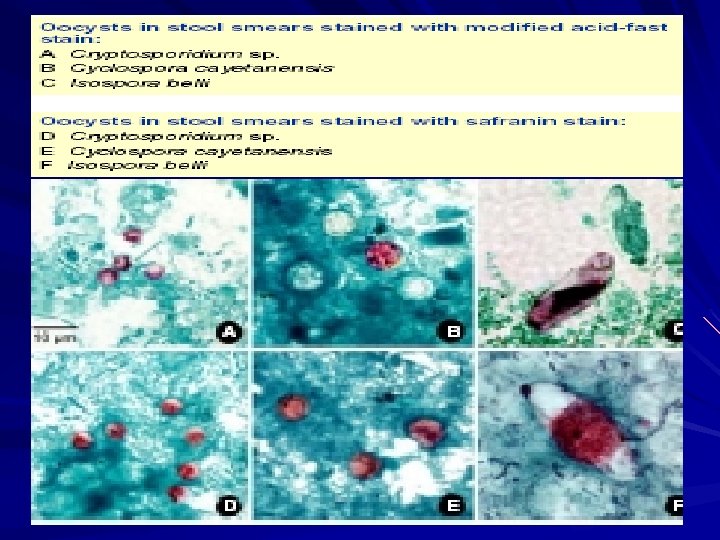
Laboratory Diagnosis Stool examinations and microscopic Repeated stool examinations and concentration procedures are recommended. Examination of duodenal specimens by biopsy or string test (Enterotest®) may be needed. - They can also be stained by modified acid-fast procedure or auramine-rhodamine stains. -The modified acid-fast procedure is especially useful.

1. Wet mount Under UV fluorescence microscopy, the oocyst wall has blue autofluoresces as illustrated in Figures C and F.

2. Modified acid-fast stain A blue-green background, or contrasting counterstain. Oocyst will stain light pink to deep purple, while others may be unstained. This staining method is the easiest and most practical, and provides a permanent record.
 is the drug of")
Treatment Trimethoprim-sulfamethoxazole combination( trimethoprim 160 mg, sulfamethoxazole 800 mg ) is the drug of choice, ”in immunosuppressed person every 6 hours for 10 days, followed by the same dose twice daily for 3 weeks. Combined pyrimethamine and sulfadiazine has also been shown to be an effective treatment. Albendazole, 400 mg twice daily for 20 days, and ornidazole, 2 g in a single dose on days 1, 15, and 20 have been effective.

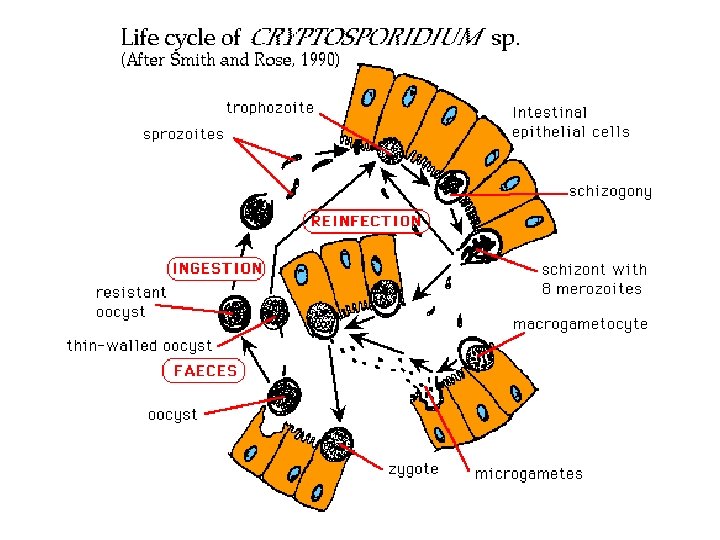
2 - Cryptosporidium spp. Many species of Cryptosporidium exist that infect humans and a wide range of animals (including mammals, birds, reptiles and fish). Cryptosporidium spp. : Human spp. : C. parvum and Cryptosporidium hominis (formerly known as C. parvum anthroponotic genotype or genotype 1). Infections by C. felis, C. meleagridis, C. canis, and C. muris have also been reported.

Cryptosporidium parvum It is a opportunist parasite of human both; Immunocompromised and immunocompetent individuals. One of the major characteristic is the lack of host specifity that sets Cryp. apart from the other coccidia. C. parvum isolates: - one containing human isolates - other containing mostly domesticated isolates

Morphology, Biology Oocysts of parasite

Life cycle

Life cycle in host

Geographic Distribution: Since the first reports of human cases in 1976, Cryptosporidium has been found worldwide. Outbreaks of cryptosporidiosis have been reported in several countries. The most remarkable being a waterborne outbreak in 1993, that affected more than 400, 000 people.

Clinical Features results in a wide range of manifestations, from asymptomatic infections to severe, life-threatening illness. Incubation period is from 2 to 10 days. Watery diarrhea, accompanied by dehydration, and malabsorption syndrome. In immunocompetent persons, symptoms are usually short lived (1 to 2 weeks). In immunocompromised it can be chronic and more severe patients, especially those with CD 4 counts <200/µl. infections in other organs including: other digestive tract organs, the lungs, and possibly conjunctiva.
. Children")
Epidemiology Crypto. as zoonosis may be acquired from domestic animals( calves and ships). Children are more commonly infected than adults. Non-breast-fed infants have more infection than breast-fed infants. For reduce the risk of waterborne Cryp. boil drinking water for 1 minute or filter drinking water with 1µm pore diameter.
 has also")
Laboratory Diagnosis Acid-fast staining methods The duodenal string test ( Enterotest ) has also been used to recover oocysts. Identify organisms in intestinal biopsy material.

Immunofluorescence microscopy For greatest sensitivity and specificity, it is the method of choice (followed closely by enzyme immunoassays). Molecular methods are mainly a research tool (PCR).

1. Wet mount In bright-field microscopy oocysts appear as small round structures (4 to 6 µm) similar to yeasts. They do not autofluoresce. This method is useful for Cyclospora, especially when low numbers of oocysts can be obscured by other fecal elements
 often have distinct oocyst walls")
2. Modified acid-fast stain Oocysts (4 to 6 µm) often have distinct oocyst walls and stain from light pink to bright red.

Treatment Infection in healthy, immunocompetent persons is self-limited. Nitazoxanide has been approved for treatment of diarrhea caused in immunocompetent patients. *The effectiveness of nitazoxanide in immunosuppressed persons is unclear. *For persons with AIDS, anti-retroviral therapy, which improves immune status, will also reduce oocyst excretion and decrease diarrhea associated with cryptosporidiosis. * In AIDS patients oral paromomycin appears to be an active and welltolerated suppressive treatment.

Cyclospora cayetanensis * This species was recognized in 1994 from Peruvian isolates of human. It appears that all human cases are caused by this species. The organism, variously referred to as; a large Cryptosporidium , a coccidian-like body , a cyanobacteriumlike body, and a blue-green alga. It is a coccidian parasite that infects a range of vertebrates including reptiles, insectivores , and rodents.

Geographic Distribution Cyclosporiasis is most common in tropical and subtropical areas. Since 1990, at least 11 foodborne outbreaks of cyclosporiasis, affecting approximately 3600 persons, have been documented in the United States and Canada.

Cyclospora oocysts

Coccidian life cycles are quite varied: 1 -completing their development in a single host such as Cryptosporidium. 2 -require a period of maturation outside the host such as Isospora. 3 -others require a second host

Life cycle of Cyclospora

Clinical Features Cyclosporiasis is clinically indistinguishable from Cryp. And Isosporiasis *symptomatic include watery diarrhea, . anorexia, weight loss, abdominal pain, nausea and vomiting, myalgias, low-grade fever, and fatigue. * Untreated infections typically last for 10 -12 weeks and may follow a relapsing course ( AIDS patients). Infections, especially in disease-endemic settings can be asymptomatic.

Pathology Inflammatory changes , villous atrophy, and crypt hyperplasia of jejunal tissue have been reported from patient with diarrhea and Cyclospora oocysts in stool specimens

Laboratory Diagnosis Microscopic examination The sediment can be examined microscopically with different techniques: wet mounts (by conventional light microscopy, which can be enhanced by UV fluorescence microscopy or differential interference contrast. stained smears (using modified acid-fast stain or a modified safranin stain)

1. Wet mount Under UV fluorescence microscopy, the oocyst wall autofluoresces.

2. Modified acid-fast stain The oocysts are variably stained. some may appear collapsed or distorted on one side. They may contain granules

3. Safranin stain Oocysts stain uniformly, red to reddish-orange. This uniform staining decreases the risk of misdiagnosis.

Sarcocystis spp. History: These parasites were first described in mice by Miescher in 1843. Host: - Defintive hosts – - Intermediate hosts Human sarcosporidia : 1 - human as accidental intermediate host - S. lindemanii 2 - human as accidental definitive host : - S. hominis( S. bovihominis) - S. suihominis S. lindemanni
 Differentiale diagnosis Sarc. from")
Morphology of Sarcocystis 1 - Tissue cyst ( Miescher’s tubules) Differentiale diagnosis Sarc. from Toxo. cyst in many cases; -Size -The limiting membrane - Septa divided the cyst into compartments.
: ( 4 to 9µm 8× 12 to 16µm )")
2 - Cystizoite ( bradyzoite): ( 4 to 9µm 8× 12 to 16µm ) 3 - Oocyst

Sarcocystis cyst
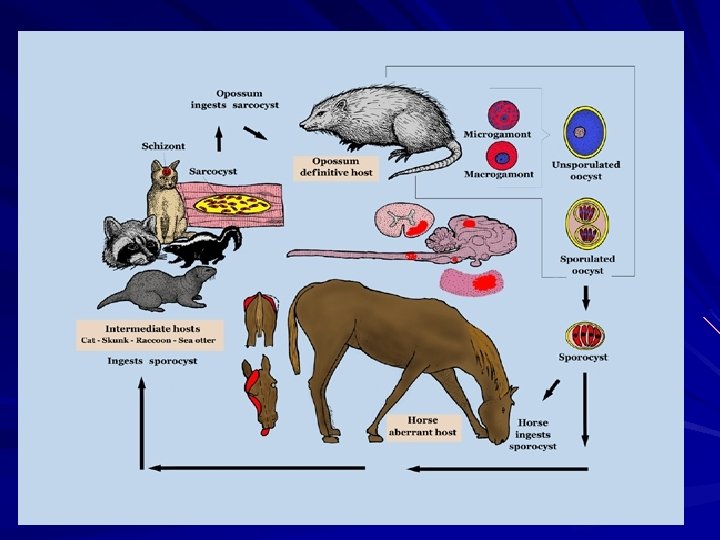

Life cycle of Sarcocystis

Pathogenesis and Symptoms -Muscular sarcocystosis: -Most human cases are asymptomatic. -Symptomatic form: - Myositis, dyspnea, and wheezing associated with eosinophilia. - Intestinal sarcocystosis: - Symptoms including; nasusea , stomach pains, diarrhea within 3 to 6 hours after ingested meat. Instance of ingest pork infected symptoms persisted for 2 to 3 weeks.

Pathology of Sarcocystis Merozoite of sarcocystis in blood smesr

Laboratory diagnosis 1 - Intestinal infections: * Exam stools for detecting of sporulated sporocysts, using zinc sulfate flotation. 2 - Muscle biopsy : Microscopic examination of a muscle biopsy CT scan or MRI can sometimes visualize sarcocysts in the muscles. Complete Blood Count (CBC) , to reveal eosinophilia, may also be helpful. 3 - Serologic tests include : IFA test Immunoblotting test (may be useful for muscle infections) Serologic tests may not be widely available.

Oocyst forms

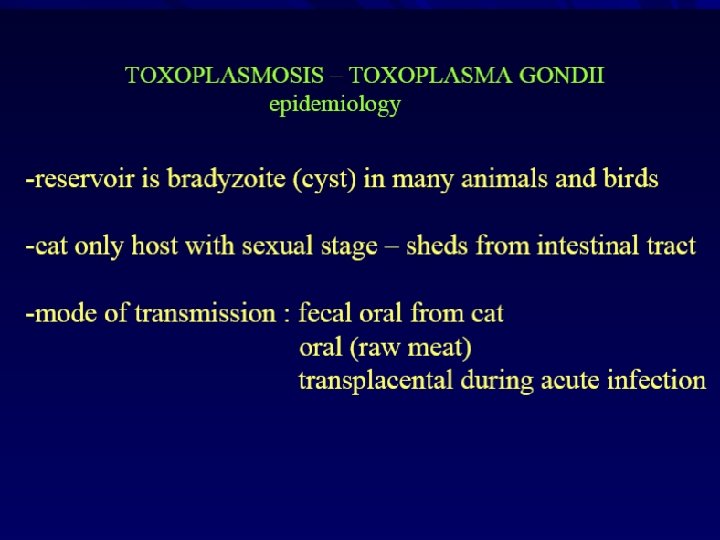
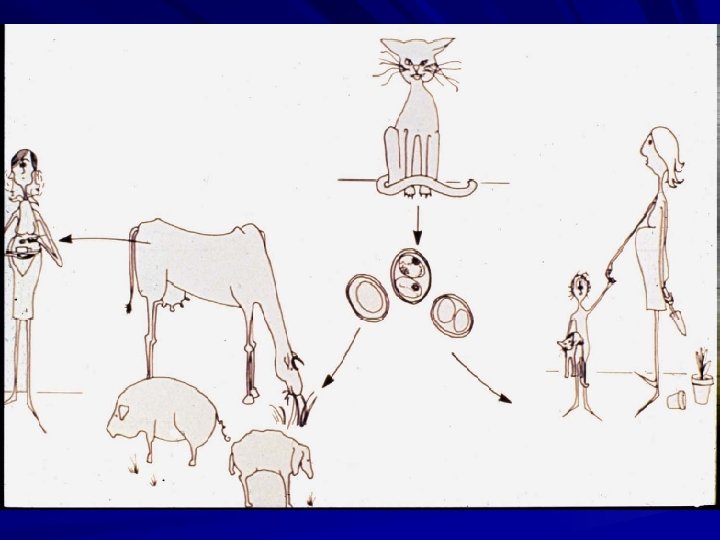
Toxoplasma gondii Causal Agent: It is an obligate intracellular protozoan parasite. It’s defintive host is the house cat and certain other Felidae. History: It was originally described in a North African rodent called ” Ctenodactylus gondi”.

Geographic Distribution - Toxoplasmosis is one of the most common of humans infections throughout the world. - Infection is more common in warm climates than in cold climates and mountainous regions. - High prevalence of infection in France and Central America (has been related to the frequency of stray cats in a climate favoring survival of oocysts. - The overall seroprevalence in the United States between 1988 and 1994 was found to be 22. 5%, with seroprevalence among women of childbearing age (15 to 44 years) of 15%.

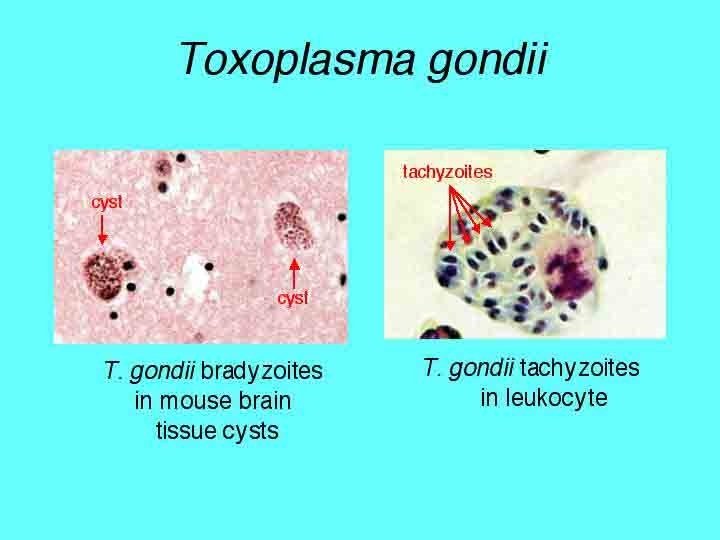
Different form of Toxoplasma *In definitive host: 1 - Immature oocyst: ( 9 - 10 µm in width by 11 - 14 µm in length) *In intermediate host: 2 - Tachyzoite ( toxoplasma trophozoite ) 3 - Tissue cyst: (contain slower-developing bradyzoite)

Life cycle of Toxoplasma

Life cycle
: Toxoplasma gondii Stained tachyzoites, microscopic preparation")
In vitro culture (MCR-5): Toxoplasma gondii Stained tachyzoites, microscopic preparation

Pathogenesis 1 - Attchment to nuclated cells of the intermediate host by secretory lectin. 2 - Secretion of peneterating-enhancingfactor(P. E. F). 3 - Endodyogeny proliferation of parasite in nuclated cells and disruption of them.
:")
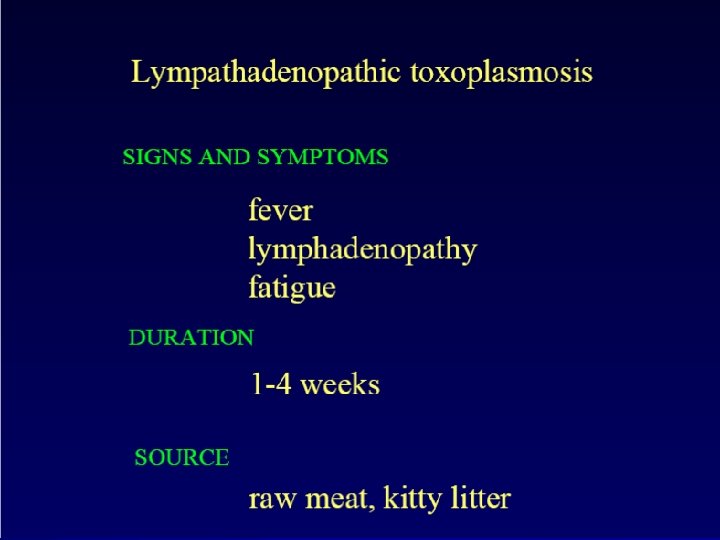
Clinical Features 1 -Acpuired Toxoplasmosis: - Asymptomatic infection: - Symptomatic infection: *lymphadenopathy( mild form): * Sever form Symptoms: Pneumonitis, hepatitis, encephalomyelitis, myocarditis, retinochoroiditis, maculopapular rashs, … In immunodeficient patients : central nervous system (CNS) disease , retinochoroiditis, or pneumonitis. Toxoplasmosis in patients being treated with immunosuppressive drugs may be due to either newly acquired or reactivated latent infection

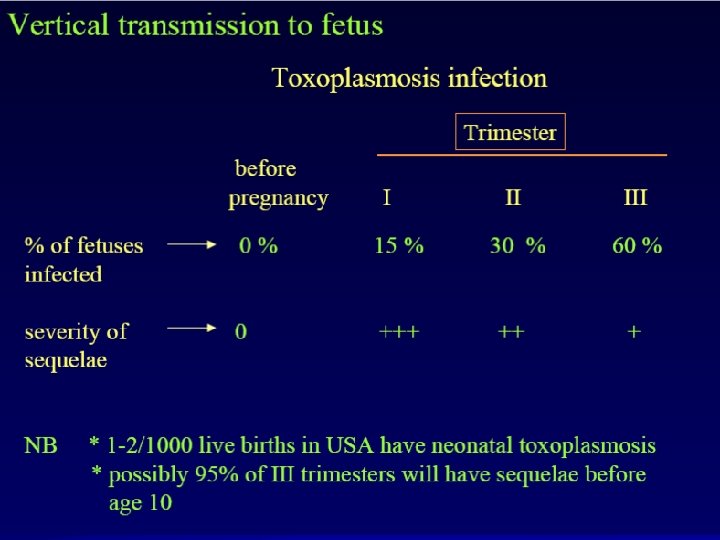
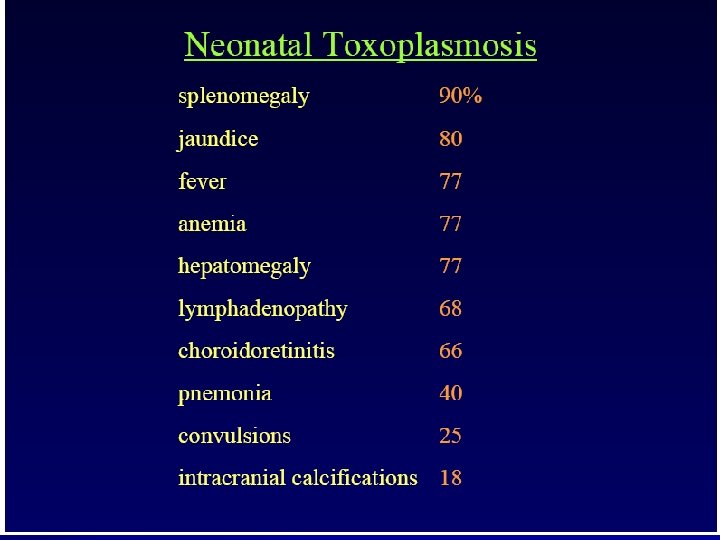
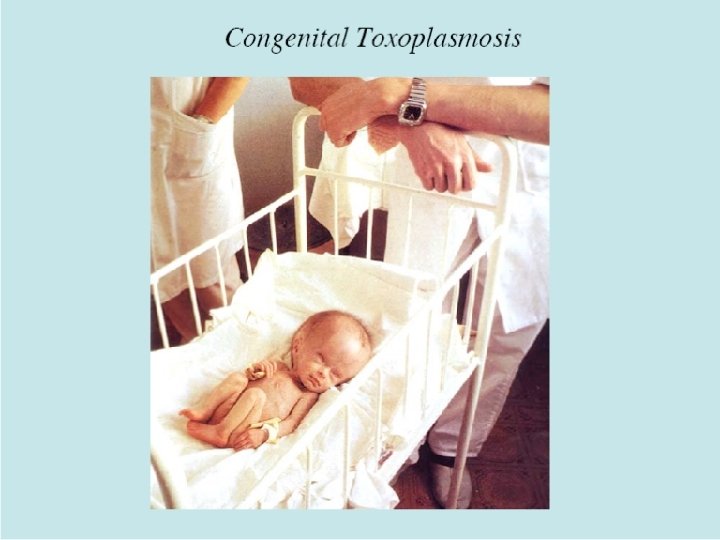
2 - Congenital toxoplasmosis The incidence and severity of congenital toxoplasmosis vary with the trimester - in the first trimaster: abortion, microcephaly, hydrocephalus, …. -in the second trimaster: Symptoms: hepatomegaly, splenomegaly, encephalitis, pnemonia, purpura, … -in the last trimaster: subclinical infection at birth subsequently retinochoroiditis (unless the infection is treated).

Histopathology of Toxoplasmosis

Pathology of Toxoplasmosis

Hydrocephaly & Microcephaly

Retinochoroiditis, is frequently a result of congenital infection. Patients are often asymptomatic until the second or third decade of life, when lesions develop in the eye.

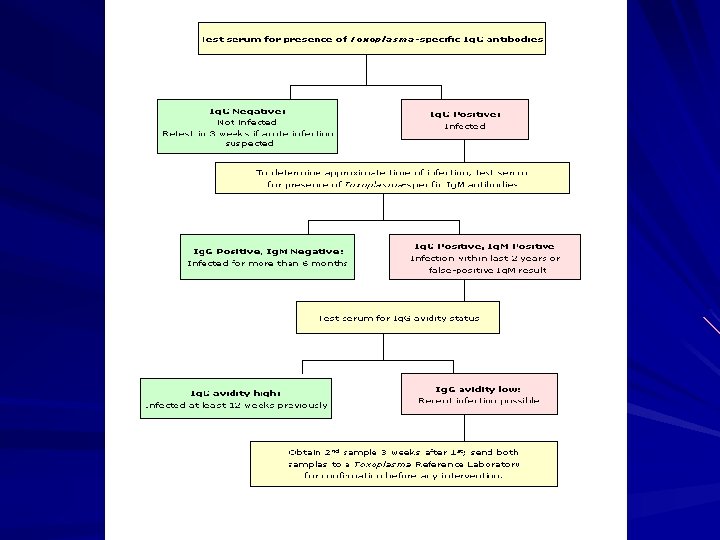
Diagnosis of Toxoplasma infection The diagnosis of toxoplasmosis may be documented by: Observation of parasites in patient specimens, such as: bronchoalveolar lavage material, or lymph node biopsy. Isolation of parasites from blood or other body fluids Detection of parasite genetic material by PCR, especially in detecting congenital infections in utero. Serologic testing is the routine method of diagnosis,

Microscopy Findings A Toxoplasma gondii tachyzoites

Microscopy finding in tissue smear B: Toxoplasma gondii cyst in brain tissue
 2 -2 I. F. A")
2 - Serological procedures: 2 -1 Sabin-Feldman( Dye test) 2 -2 I. F. A test 2 -3 I. H. A test 2 -4 D. A. T 2 -5 C. F. T 2 -6 ELISA test 3 -Detection of parasite genetic material by PCR, especially in detecting congenital infections in utero.

IFA TEST AA B C A: Formalin-fixed Toxoplasma gondii tachyzoites, B: Negative IFA for antibodies to T. gondii. C: Negative IFA for antibodies to T. gondii, polar stain reaction.

Treatment may be recommended for pregnant women or persons who have weakened immune systems. Before 16 th weeks' gestation – 4 weeks Spiramycine After 16 th weeks' gestation (Seroconversion, or persistend Ig. M in the 2 nd or 3 rd Trimenon) alternating to birth 4 weeks combination of: Pyrimethamin [Daraprim©], Sulfadiazin, Folinic Acid 4 weeks Spiramycine [Rovamycine©]
 Both cellular & humoral immunity; especially humoral Play main")
Immunity Concomitant immunity( premuntion ) Both cellular & humoral immunity; especially humoral Play main role. Cellular immunity IL-12 increase Th 1 INF-γ Activate macrophage CD 8+ Lysis of infected cell

- Slides: 84