APHERESIS PRESENETED BY DR AKSHI GUPTA GUIDED BY

APHERESIS PRESENETED BY: DR AKSHI GUPTA GUIDED BY: DR ARCHANA BIDARI DR ROHINI SHEWALE

INTRODUCTION �Apheresis is a procedure carried out to harvest a particular component and returning the rest of the blood to the donor, by an automated machine. �This procedure should be carried out only in a blood bank licensed for this purpose.

PREREQUISITES �A medical officer trained in apheresis technique should be responsible for the procedure. �The staff working on the machine should be trained in apheresis procedure and should work directly under the supervision of the medical officer.

�The donor should be asked to sign a consent form in the language, which he understands after being explained the procedure and the risks involved. �Separate area of 10 square meters shall be provided.

APHERESIS ROOM S. S. Mohite, Jt. Comm, FDA, Maharashtra
 �CFC (continuous flow centrifugation)")
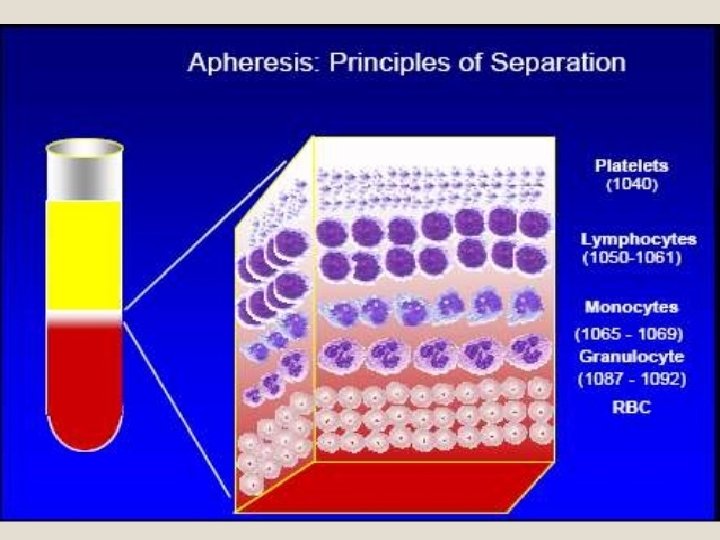
PRINCIPLE OF APHERESIS �IFC (intermittent flow centrifugation) �CFC (continuous flow centrifugation)

INTERMITTENT FLOW CENTRIFUGATION
 � Blood is collected from an individual")
� Performed in cycles (known as passes) � Blood is collected from an individual � Anticoagulant (CPD or ACD) is added to tubing � Separated components flow from bowl through outlet port into separate collection bags � Undesired components are diverted into reinfusion bag and returned � Reinfusion � Cycles completes one cycle are repeated until the desired quantity of product is obtaineed


CONTINUOUS FLOW CENTRIFUGATION �Withdraws, process and return the blood to individual simultaneously �Always done with 2 venepuncture sites �Advantage: low extracorporeal blood volume is used, so useful in elderly and children

INDICATIONS OF APHERESIS �Donor Apheresis: collect the components for transfusion �Therapeutic Apheresis: removing undesirable blood component

CYTAPHERESIS �Cytapheresis is the procedure for separation of individual cellular component of blood. �It can be achieved by the cell separator machine.

PLATELETPHERESIS �Plateletpheresis is the harvesting of platelets from whole blood using continuous or intermittent flow cell separator.

Selection of donors �Donors who undergo cytapheresis no more than once every 4 weeks should be treated as ordinary blood donors with regards to laboratory studies. �Age should be between 18 -50 years. �Weight be 60 Kg or more

Donors who undergo serial cytapheresis, more than once every 12 weeks, should be tested as under : Haemoglobin and/or haematocrit should be >12 g/dl and or Hct of 36%. � Total serum protein should not be below 6. 0 gm/dl. It should be tested before the 3 rd collection if done within 4 weeks. �

�Platelet count >150, 000 /ul. �Total and differential white cell count should be normal. �Persons who have ingested aspirin or similar anti-platelet drugs in the last 72 hours should not be taken. �Donors with personal and family history of bleeding tendency should not be suitable for plateletpheresis.

�In serial pheresis a minimum interval should be of 48 hours and not more than two procedures in a week should be allowed. �A participant of such a programme donates a unit of blood or if it has not been possible to reinfuse the red cells during a pheresis procedure should not be accepted for cytapheresis for 12 weeks.

�Donor should be screened prior to apheresis for markers of infectious diseases transmitted by the transfusion of blood and its components in the same manner as for the whole blood. �Each donor must be tested prior to each apheresis unless the donor in undergoing repeated procedures, in such cases testing for the markers of diseases need be repeated at 30 days interval.
 �Platelet concentrates should contain minimum 3 x 1011 platelets")
�Platelet concentrates (Single Donor Platelets) �Platelet concentrates should contain minimum 3 x 1011 platelets in 75% of the units tested amongst 1% of monthly production or 4 platelet concentrates per month, whichever is higher. �They can be stored for 3/5 days at 220 C +20 C with continuous agitation depending on the blood bag used. �The p. H must be 6 or higher at the end of permissible storage period (3 -5 days)in all the PC units.

SDP v/s RDP SDP RDP One donor – 8 units One donor- 1 unit Post tranfusion platelet rise- 6070, 000/cmm Post transfusion platelet rise 5000 -7000/cmm Platelet yield=30 x 1010 per bag Platelet yield=3. 5 x 1010 per bag Next donation possible after 48 hrs, max upto 24 times/ year Next donation possible after 3 months, max 4 times/ year S. S. Mohite, Jt. Comm, FDA, Maharashtra

LEUKAPHERESIS is the harvesting of granulocytes from whole blood using continuous or intermittent cell separator. �Before leukapheresis total white blood cells counts should be 4000 /ul with normal differential count.

�Granulocyte concentrates �Leucocyte concentrates should contain at least 1 x 1010 leucocytes. �They should be transfused as soon as possible, preferably within 6 hrs. �Transfusion should not be given through microaggregate filters.

PERIPHERAL BLOOD STEM CELLS �Are harvested using continuous or intermittent cell separator. �Attempt should be made for harvesting minimum of 2 x 106 CD 34 cells and / or minimum of 2 x 108 MNCS/Kg of the recipient.

PLASMAPHERESIS �It is a procedure to harvest plasma from the whole blood and returning the cellular components to the donor. �Plasma is harvested by automated machine.

THERAPEUTIC PLASMAPHERESIS AND CYTAPHERESIS � To be done only at the written request of the patient's physician either in the blood bank or preferably in the ward depending on patient's clinical condition. � Records of patient's identification, diagnosis, therapeutic procedures, haemapheresis method, volume of blood removed and returned, time taken, nature and volume of replacement fluids, adverse reaction if any and medication administered, should be maintained. � Informed consent of the patient should be taken in the language he/ she understands. � Provisions for emergency care should be available.

Common Conditions for Therapeutic Plasmapheresis and Pathological Substances Removed �Waldenstrom’s macroglobinaemia: Ig causing hyperviscocity �Myastheniagravis: Autoantibodies �Goodposture’s syndrome: Autoantibodies �Hypercholesterolemia: Lipoproteins �Post transfusion purpura due to anti-PIA 1: Platelet antibodies �Acute Guillain-Barre syndrome: Uncertain �Lupus erythematosus: Immune complex �Factor VIII inhibitor Auto-or allo-antibodies �TIP: Platelet-aggregating factors �Barbiturate poisoning: Protein-bound toxins

EQUIPMENTS
")
�It has a continuous flow centrifugation technology complete with an Automated Interface Management (AIM) system for patient safety, and procedural efficiency. SPECTRA OPTIA

�Portable machine �Can be used for multiple procedure types based on kits set: �Spectra Optia MNC Collection set, Plasma exchange set, Granulocytes Depletion set, Platelet Apheresis Set and BMP Accessory set. �Different procedures will need specific test.

�Can be used for collecting platelets, plasma and RBCs on only one automated collection platform. �Collect products based on the percentage of a donor’s total blood volume. TRIMA ACCEL

Dimensions: �Height: 68. 5 cm �Width: 56. 5 cm �Depth: 56. 5 cm �Weight: 27. 5 kg HEMONETICS

�Ambient operating temperature: 180 C to 270 C �Tested storage temperature: 00 C to 400 C �Input voltage: 230 VAC +/- 10% �Operating Current: 1. 9 A �Operating frequency range: 50 -60 Hz �Maximum leakage current: 500 μA

REFERENCES � Transfusion Medicine, Technical Manual. Directorate General of Health Services Ministry of Health & Family Welfare Government of India � Accreditation standards on Blood banks/ blood centers and Transfusion services, June 2016, NABH � Standards for Blood Banks & Blood Transfusion Services, 2007, National AIDS Control Organisation, Ministry of Health and Family Welfare

THANK YOU
- Slides: 35