Aortic Dissection Clinical Presentation Diagnosis and Medical Management




 – ant.")





 – Ca sign")



















- Slides: 33
Aortic Dissection Clinical Presentation, Diagnosis and Medical Management Adoracion N. Abad, M. D.
Aortic Dissection • not very common, but challenging, frequently fatal, emergency clinical condition • keys to improve outcome: – high index of suspicion – prompt diagnosis and treatment
Predisposing Factors • HPN – 62 -78% • aortic disease – aortic dilatation/aneurysm – annulo-aortic dysplasia – chromosomal aberration • Turner’s syndrome • Noonan’s syndrome – – aortic arch hypoplasia coarctation of aorta bicuspid AV heredetary CTD • Marfan’s syndrome • Ehler’s Danlos syndrome
Predisposing Factors Cont… • traumatic injury – – arterial cannulation during surgery catheter based diagnostic or therapeutic intervention chest trauma high intensity weight lifting or other strenuous R training • cocaine • β blocker withdrawal • women <40, 50% occurs during pregnancy – HPN in 25 -50%
Clinical Presentation • CP – severe, abrupt, sharp or “tearing” (72. 7%) – ant. CP – dissection in asc Ao – post. CP or back pain or abdominal pain distal to L subclavian – can radiate anywhere in the thorax or abdomen – can occur alone or associated with: syncope CVA M. I. CHF
Clinical Presentation Cont… • • • HPN – more common in type B (70% vs 35%) CHF – (7%) syncope – (12. 7%) cardiac arrest or sudden death neurologic – CVA paralysis • M. I. – (1 -2%) – involvement of coronaries – RCA>L – with thrombolytic – mortality >70%
Clinical Presentation cont… • Involvement of desc. Ao sphlancnic ischemia renal insufficiency lower extremity ischemia spinal cord ischemia CP or back pain 86% abdominal pain 43% abrupt onset 89% HPN 69% hypotension/shock 3% peripheral neuropathy 2% migratory pain ARF 25% 14% IRAD Registry
Differential Diagnosis • • • myocardial ischemia M. I. with or w/o ST elevation pericarditis pulmonary embolism AR without dissection AA with dissection musculoskeletal pain mediastinal tumor pleuritis PUD/perforating ulcers acute pericarditis
Diagnosis of Aortic Dissection • Prediction model for early diagnosis of Ao dissection – – In analysis of 250 patients with CP or back pain, 128 with dissection 96% can be identified by combination of 3 clinical predictors: 1. immediate onset of CP with tearing and or ripping character 2. mediastinal and or aortic widening on xray 3. variation in pulse BP > 20 mm. Hg between R and L arm
Diagnosis of Aortic Dissection cont… incidence of dissection • • when all variables absent aortic pain mediastinal/Ao widening pulse or BP difference or any combination of the 3 7% 31% 39% 83% Von Kodolitsch et al. , Arch Intern Med 2000; 160: 2977 -2982
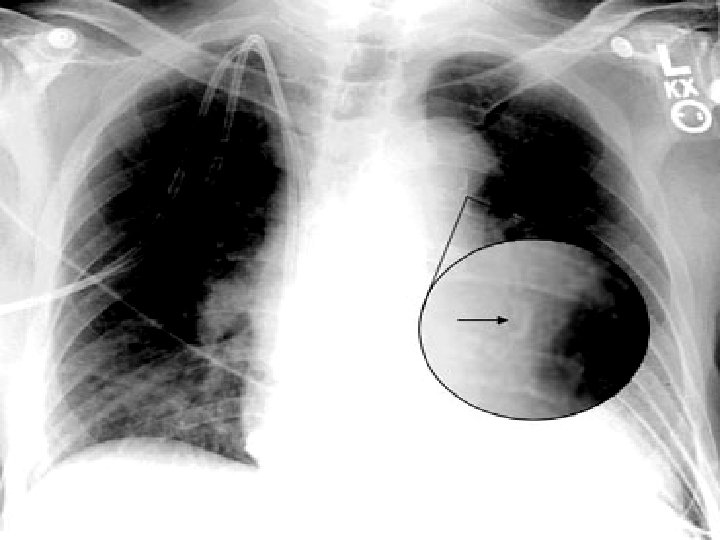
Diagnostic Procedures • CXR – widening of mediastinum (60 -70% sensitivity) – Ca sign – separation of intimal calcification from outer aortic soft tissue border by 1 cm
Diagnostic Procedures • ECG – no specific findings associated with dissection – 1/3 – LVH – 1/3 – normal – ischemia
Diagnostic Procedures • TEE – can be done fast, safely and in any environment • high sensitivity up to 98% • high specificity up to 97% – specifically informative AR PE ostia of coronaries involved CT
Diagnostic Procedures • TEE limitations: – unable to visualize distal ascending and descending abdominal aorta – technically difficult in esophageal structures or varices
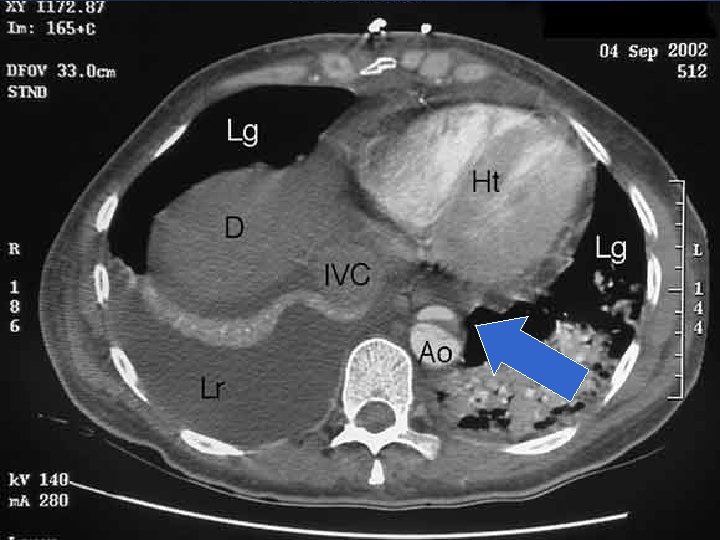
Diagnostic Procedures • CT Scan – identifies 2 distinct lumen with intimal flap – sensitivity with contrast 83 -98% no contrast - 76 -90% – specificity with contrast 87 -100% no contrast - 70 -82% • advantages: – readily available in most hospitals even on emergency basis – identifies intraluminal thrombus and PE
Diagnostic Procedures • limitations: – intimal flap seen in < 75% – site of entry rarely identified – contrast potentially nephrotoxic – cannot assess AR or coronary involvement
Diagnostic Procedures • Spiral CT – gives accurate 3 D view of aorta • sensitivity – 91 - 100% • specificity – 96 -100% – disadvantages • Potentially nephrotoxic, site of entry difficult
Initial interpretation was findings c/w aortic dissection, with thrombosis of the false lumen. Only a small amount of flow is present in the false channel at this point in time, suggesting the dissection may be healing, and stablilizing.
Diagnostic Procedures • MRI – currently gold standard • sensitivity – 98% • specificity – 98% – determines location of intimal tear, secondary tears and branched vessels – no contrast needed – can detect AR – disadvantages • limited availability • time consuming • contraindicated in metallic implants
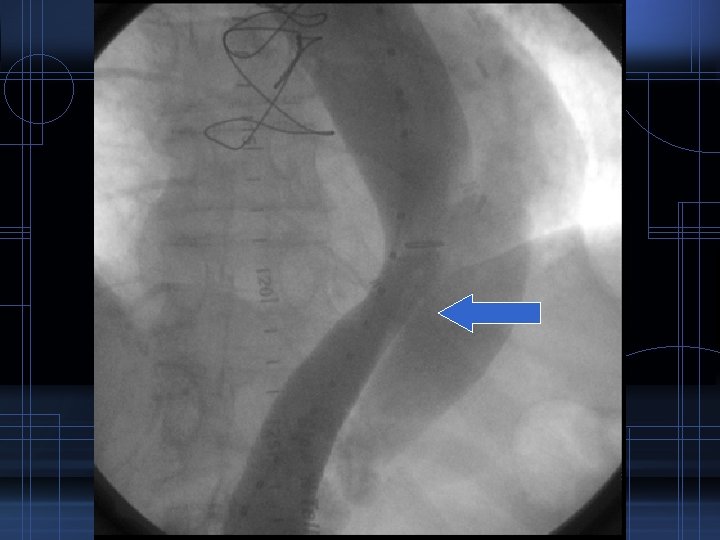
Diagnostic Procedures • Aortography • sensitivity – 86 -88% • specificity – 75% – procedure of choice in earlier days – now rarely used because it is invasive, needs contrast and consumes time
What is the Best Modality? • Depends on: – accesibility – expertise of the institution
Management • General principle – Aortic dissection of ascending aorta – surgical emergency – If confined to descending aorta – medical except when there is hemorrhage into pleural or retroperitoneal space – In all – prompt control of BP if HPN present
Management • Medical – uncomplicated distal dissection – stable dissection isolated to aortic arch – stable chronic dissection
Medical Management • ICU admission • target BP – 100 -120 mm. Hg SBP or lowest level tolerated to d. P/d. T (force of ejection of flow from LV) – nitroprusside/nicardepine – β blocker (esmolol, propranolol or labetatol) • if β blocker contraindicated – verapamil or diltiazem • if with refractory HPN – evaluate renal artery involvement
“Disease is very old, and nothing about it has changed It is us who change as we learn to recognize what was formerly imperceptible” Dr. Jean Martin Charcot
Take Home Message • Despite recent advancement in diagnosis and treatment, mortality remains high • We need to continue improvement in prevention, prompt diagnosis and management of this frequently fatal condition
Thank You!