ANXIETY DEPRESSION STRESS How Mental Health Effects Us


 47%")


: About 20% of American")



 whose mother has untreated depression and father has untreated bipolar")

")

















: � Exposed 4")












 has been on rise since 1980’s � Question #11")



 2. Therapy (counseling)")

 act on serotonin")
 are intended for short-term use, and not regarded as")



 � Cognitive-Behavioral Therapy � � � Based on theory that negative thinking")







 Symptoms")


 which effect")





, The Brain that Changes Itself. Eagleman,")
- Slides: 73
ANXIETY, DEPRESSION, & STRESS How Mental Health Effects Us and Our Students Larry Scott lscott 2@ktufsd. org
Agenda I. II. III. IV. V. VII. Current State of Mental Health General Characteristics of Anxiety & Depression Anxiety Self-Harm & Suicide Addiction Mental Health Treatment/Intervention
Community Mental Health Crisis � North of NYC (over a 5 year period) 47% of people killed by police suffered from a mental illness or were emotionally disturbed � 56% of NYS prison population have a “mental health problem” including substance abuse (5 x the rate of general public) � 8, 000 inmates are cared for by NYS Office of Mental Health � About 17% of U. S. prison population have mental illness (3 x the rate of the general public)
Community Mental Health Crisis � Mentally ill are more likely to be victims of crime, than criminals, and they are more likely to be harmed by police, than harm police � Law enforcement have become primary providers for those with serious mental illness � Cuts, consolidations, and closings in mental health continue � In 1955 the U. S. had 558, 000 beds for mentally ill; today we have about 40, 000
Poverty & Mental Health � The number of poor in the entire Buffalo Niagara metropolitan area grew from 120, 861 in 1970 to 162, 917 in 2011 � 52 percent of this area’s poor reside in the suburbs � Mobile Safety-Net Team (John R. Oishei Foundation): � Free/reduced lunch in Ken-Ton (#1): 27% in March of 2001 compared to 41% in March of 2013 � Ken-Ton agencies School District is the largest human service of 38
Youth & Mental Health � Question #4 � CDC (2012): About 20% of American youth (aged 3 – 17) suffer from a mental health disorder � Chronic health problems (i. e. asthma & diabetes) are associated with mental illness in adulthood � Question #3 � � $247 Billion is spent per year for mental health services from medical bills, special education, and juvenile justice Question #2 � Suicide has become the 2 nd leading cause of death among youth (aged 10 -19) behind accidents
Emotion & Mood � Everyone experiences varying emotion and mood, including symptoms of anxiety and depression � “Emotion is the weather, mood is the climate. ” (C. Smith) � Mood: sustained emotional state which impacts how we respond on a regular basis; becomes more of an internal state, independent of external circumstances � Emotion: short-term and more influenced by external factors � Mood exists across species; the more developed the species the more intensely mood exists independent of external events � Some manage the interaction of mood, personality, and stress well, while it becomes problematic for others
Anxiety & Depression � Anxiety & Depression often co-exist and influence each � Share a single set of genes, which are also involved in alcoholism � Depression: a response to loss; Anxiety: a response to future loss � Intervention is needed when anxiety and/or depression interferes with a life function (i. e. work, school, family relationships/functioning…. ).
“Biopsychosocial” Model Genetics Personality Environmental Neuropsychological
Case History Sherri (13) whose mother has untreated depression and father has untreated bipolar disorder, is having meltdowns in school and failing many subject areas. Sherri lives in a duplex in a poverty stricken and violent neighborhood. Sherri was born premature and was separated from her mother several times until the age of two, due to hospitalizations for medical issues. Last summer, a friend of Sherri’s was shot and killed in her neighborhood. Sherri exhibits high irritability and often perceives others as untrustworthy and guilty of mistreating her. A socialemotional assessment indicates that she perceives limited internal control over events in her life. Blood work indicates high levels of the stress hormone, cortisol, which is associated with depression and cognitive deficits.
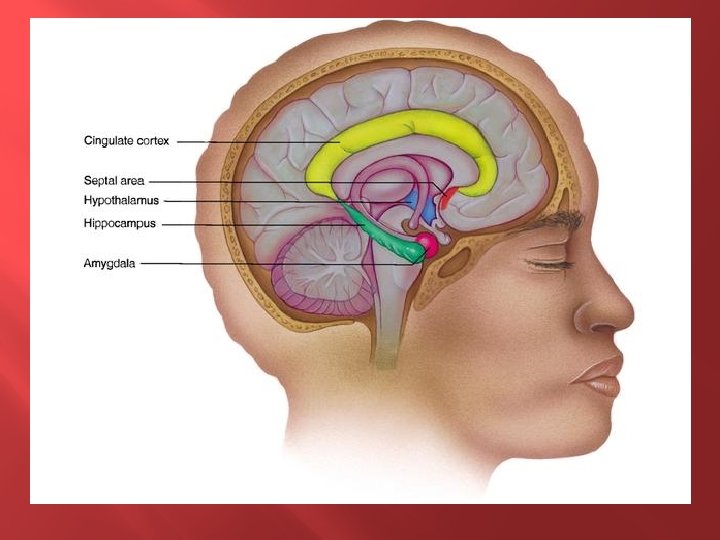
The Brain � Brain Plasticity � Between approximately 10 to 18 months of age is a critical period of plasticity and shaping of the brain (right frontal lobe) for attachments & emotional regulation � Neglect/trauma during this period can negatively shape “wiring” for attachments & emotional regulation, which can continue into adulthood � Limbic System (amygdala, hypothalamus, hippocampus, & thalamus) is involved in emotional regulation
Depression � About 19 million Americans suffer chronic depression (over 2 million are children) � About 15% will commit suicide � 2. 3 million suffer from Bipolar Disorder � Could be leading cause of death when considering its influence on suicide, substance abuse, heart disease, and other health issues � Anger & violence may be symptoms of depression, particularly in males
Depression � Females are 2 x more likely to suffer depression, a ratio consistent throughout Western societies � Rate of depression is about the same among working and non-working married females � Males synthesize serotonin 50% more rapidly than females � Males are more likely to have ADHD, autism, and alcoholism � Those who are not open about LGBTQ status and single people have a higher rate of depression
Depression � Question #5 � Leading cause of disability in U. S. for those over the age of 5 and leading cause worldwide (WHO); costs tens of billions yearly in lost productivity � Question #6 � Women who are pregnant or have just given birth are more likely than anyone else to suffer depression, but least likely to commit suicide � Question #7 � Poverty & parent depression are highest predictors of child depression � Question #8 � LGBTQ are at increased risk for depression and anxiety problems. Suicide is the number 1 cause of death for this group � Question #9 � Those in poverty represent the highest rate of depression compared to any other class in U. S. � Question #10 � 85 – 95% of those with serious mental illness are unemployed
Characteristics of Depression � � � � � Fewer social skills and close relationships Fewer social interactions Limited interest in activities Limited motivation and academic achievement Irritability Limited energy Limited affect Worsened with the presence of learning weaknesses Most challenging during adolescence
Genes & Depression � There are particular genes involved in serotonin regulation which predispose depression, but whether one suffers depression is dependent on life events/experiences � There are three possible gene combinations, one from each parent: short/short, short/long, and long/long � A short/short combination with multiple uncontrollable bad life events makes it about twice as likely to suffer from depression than long/long combination
Genes and Depression Short/Short High Predisposition 2 x more likely to suffer Depression than Long/Long Multiple Uncontrollable Events
The Brain & Depression/Trauma � Significant episodes of depression alter brain chemistry (i. e. decrease Serotonin receptors) and structure (i. e. hippocampus) � With each episode of depression there is an increased 10% risk depression will become chronic and inescapable � Early childhood trauma causes major changes to the brain’s hippocampus, shrinking it & inhibiting new, long-term memories � Depression, high stress, and childhood trauma all cause the release of stress hormone (glucocorticoid)- kills cells in the hippocampus � The longer someone is seriously depressed or under high stress the smaller their hippocampus. � Antidepressants have been found to increase stem cells that become new neurons in the hippocampus � It takes about 3 -6 weeks on an antidepressant for new neurons to mature and connect with other neurons
Mothers with Depression � Depressed mothers greatly influence the likelihood that a child will suffer depression or other emotional / behavioral issues � Having a depressed mother is often more detrimental than a schizophrenic mother � With a depressed mother, signs of depression can be seen in infants, as early as 3 months: weepy, angry, & aggressive � If mother’s depression is treated early, children show improvement, reversal becomes more challenging with age
The Course of Depression � Depressed children usually go on to be depressed adults � Occurs in many before puberty, but peaks in adolescence � The earlier the onset the more resistance to treatment � Early/preventative intervention is critical
Why So Much Depression? � Four possible theories: 1. Served an important purpose in pre-human times 2. The stresses of modern life are incompatible with the brains we have evolved. 3. It serves a useful function. 4. It is a secondary result of other characteristics.
Why So Much Depression? � Self-Consciousness: high awareness of self, metacognition, and awareness of competing cognitive functions (i. e. rational and emotional thinking) makes us unlike any other species � Humans have the slowest brain maturation and are most plastic at older ages � Humans exhibit significant capacity to regulate emotions � Linguistic-Evolutionary Model (Crow, Timothy) mental illness is on a continuous spectrum and is determined by difference in intensity of symptoms
Linguistic-Evolutionary Model Low Intensity Moderat e Intensity High Intensity
Video � Out of the Shadows
Anxiety � 10 – 20% Americans suffer from Anxiety Disorder � About ½ of those with true anxiety disorders develop major depression within 5 years � Worsens with time if untreated � Anxiety is often overlooked, misdiagnosed as ADHD, left untreated, and sometimes worsened when misdiagnosed � Anxiety is difficult to detect- internal, not easily observed � Children and self-awareness � Medication
When Does Anxiety Confront Us? � When doing something new � When uncertain about plans � When there “what ifs” � When you have to perform � When doing something scary
Anxiety � The opposite of peace and feeling safe � “Curse” of sensitivity & empathy: a capacity for feeling deeply, including emotional pain, which both can be helpful and hindering. � Often obsessive thinkers without compulsive tendencies � Anticipatory anxiety
Characteristics of Anxiety � Strong episodes of anxiousness and panicky feelings � Feelings of bewilderment and unreality � Feelings of depression and hopelessness � Restless feelings, insomnia, sleeping too much � Picking at self or objects � Uncontrollable bouts of anger/crying � Obsessive-compulsive tendencies � Withdrawing � Frightening, gruesome thoughts (diversion from conflict)
Temperament & Personality � Temperament: inborn, biological ways of responding emotionally/behaviorally in infancy and early childhood � Personality: outcome of an interaction of biological traits with social and personal experiences S. Cain (2013): Quiet
Anxious Children � Longitudinal study by Jerome Kagan, 1989 (500 infants): � Exposed 4 month-olds to novel experiences: strange visuals, loud noise, and odd smells � 20% were found to be “high reactive” S. Cain (2013): Quiet
“High Reactive” Children Novel Stimuli Traits Development • Cried vigorously, pumped arms/legs • Higher activity in amygdala • Higher heart rate, and more eye dilation and cortisol in saliva • Introverted, sensitive, deep processors • Highly attentive to others, environment, and experiences • Sensitive to sensory stimuli (amygdala) and family challenges (abuse, marital tension, and death of a parent) • Prone to be shy and more likely to experience anxiety/depression • Socially- usually empathetic, caring, and cooperative, while easily upset with injustice, cruelty, and irresponsibility • With good home life/parenting- often have fewer emotional problems and better developed social skills
Panic Attacks � Experiencing severe panic attacks can be debilitating � Often develop from life events where there is a loss of security or perceived loss of security � Most difficult factor- it is uncontrollable, feelings occur for absolutely no reason � About 1/3 of panic attacks related to depression occur during deep, dreamless sleep
Panic Attacks Cognitive Symptoms: � “I’m going to have a heart attack. ” � “I’m about to die. ” � “I can’t breathe properly. I’m going to suffocate. ” � “I’m about to pass out. ” � “I’m going to lose control and go crazy. ”
Panic Attack: Physical Symptoms Pounding heart Tight, tense muscles Chest pain / tightness Shortnes s of breath Feeling unreal or detached Nausea / dizzy Trembling Hot / cold flashes Numbness / tingling
Fear � What is the difference between fear and danger? � When is it smart and useful to be scared?
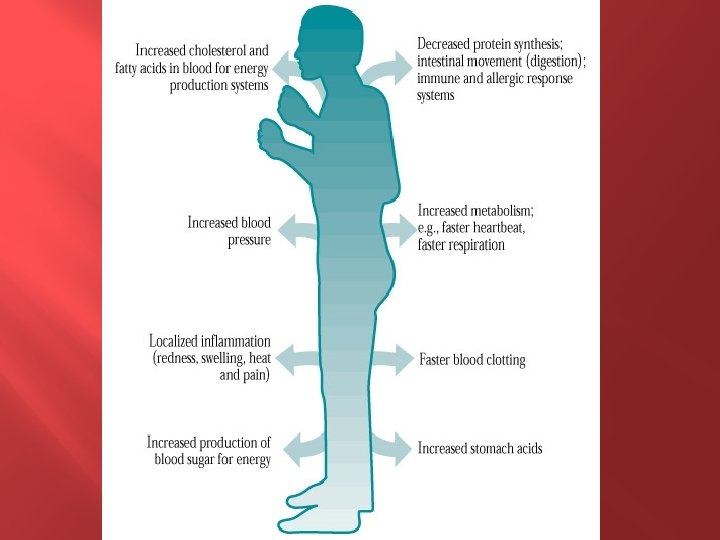
Physiology of Anxiety/Panic � Anxiety is one of the most basic emotions found in almost all animal species � Is a response to danger or threat- perceived or real � It’s primary purpose is to protect us, not harm us � “Fight/Flight/Freeze” response � Sympathetic nervous system releases energy to respond to threat � Parasympathetic nervous system restores the body to normal function
ANXIETY CYCLE Control Anxiety Control
The Brain & Anxiety � People with high anxiety lock onto worry and can’t let go � Their brains are haunted with horrific scenarios that present as quite real and can’t be ignored � Norepinephrine and serotonin are neurotransmitters which play a role in anxiety � Locus coeruleus controls norepinephrine production & the lower bowel
Brain chemistry changes = feeling unpleasant Perceive threat/fear Do something to feel better: AVOID, seek reassurance ask a lot of questions, etc… Dr. K. Morrow
AVOID, AVOIDING VALIDATE STUDENT’S FEELINGS & CHALLENGE ANXIETY
Suicide � Depression is not always the primary reason or only reason; often committed after coming out of a depression or long after recovery � Suicide is more a response to anxiety and a tortured mind, rather than a solution to depression and purposeless mind � Many unknowns � There is a significant difference between wanting to die and wanting to kill yourself � Question #12 � Prior attempt to commit suicide is highest predictor of suicide
Suicide � Statistics: � Most often on Mondays, between late morning & noon, and spring � Evidence suggests that the best-intentioned prevention programs introduce the idea to a vulnerable population & increase the rate � Suicide rate for age group of 10 – 14 increased by 120% between the early 80’s to the mid-90’s; 85% use aggressive means (guns, hanging, and poisoning) � Question #13 � � U. S. is the only country where guns are the primary means of suicide; more Americans kill themselves with guns than murder others with guns, yearly 10 states with lax gun-control laws have a suicide rate 2 x that of states with the strongest gun-control laws
Self-Harm � Deliberate Self-Harm (DSH) has been on rise since 1980’s � Question #11 � Average of onset is about 13 � Females are 3 x more likely than males � Reasons from an Inpatient Population: � � To stop bad feelings To relieve feeling numb or empty even to feel pain To punish themselves To get help or attention out of desperation
Self-Harm & Suicide Differentiation � Self-harm: intentional, non-life threatening bodily harm or disfigurement while in a state of distress � Suicidal behavior: act of self-inflicted, self-intended cessation of life � Question #14 � � Less than 1% kill selves from cutting Self-harm is usually life sustaining act associated with the following: � � “Life preserver” rather than exit strategy May become angry if described as suicidal
The Brain & Suicide � Low levels of serotonin in brain areas associated with inhibition and freedom to act impulsively on emotion (similar to impulsive murders/arsonists) � Excessive number of serotonin receptors (possible brain compensating) � Stress reduces serotonin making the combination of stressful events and depression high risk for suicide
Dialectal Behavior Therapy � A cognitive-behavioral treatment empirically supported to treat self-harm in patients with Borderline Personality Disorder � Views self-harm behavior as a combination of dysfunction in emotional regulation in the brain & invalidating social environment, causing confusion of self, impulsivity, emotional instability, & interpersonal problems � Provides a comprehensive structure for treatment providers in dealing with a complex behavior
Treatment � Two Broad Treatment Methods: 1. Medical (medication and/or electroshock) 2. Therapy (counseling) � Medication & therapy should be complimentary, not competitive; used together or separately depending on the situation and individual � Large study by NIMH (2004) on moderately to severely depressed youth (aged 12 – 17): � � � CBT: 69% success Prozac: 65% A combination of Prozac and CBT: 85%
Medication � U. S. use of psychiatric medications is far higher than any other country � Question #15 � Anti-depressants have become the most used drug in U. S. (about 10% of adults) � About 28 Million Americans are on SSRIs (Selective Serotonin Reuptake Inhibitors) � About 16% of females, compared to 6% of males � About 5% of adolescents (aged 12 – 19) take an antidepressant � White adolescents are 5 x more likely to use antidepressants than black adolescents and 2 x more than Latino � 1996 – 2005: 40% drop in those receiving therapy
Antidepressants � Selective Serotonin & Norepinephrine Reuptake Inhibitors (SSRI’s & SNRI’s) act on serotonin and some also act on norepinephrine � Are useful in treating chronic anxiety � Are relatively safe drugs, but do have side effects and unpleasant withdrawal symptoms (sometimes dangerous)
Anti-Anxiety Medication � Benzodiazepine (tranquilizers) are intended for short-term use, and not regarded as safe drugs for long-term treatment of anxiety � Physical tolerance and dependence requiring the need for more of the medication can lead to addiction and abuse � Dangerous when mixed with alcohol � Withdrawal symptoms can be very unpleasant and dangerous
Medication Limitations � In isolation, does not address a psychological understanding of anxiety and depression � Limited research and education on long-term use and effectiveness, especially with children/adolescents � Weaning off medication can be a challenge and withdrawal can be unpleasant � Side effects, stigma, and uncertainties make medication a challenging decision for parents
Big Pharma � Question #16 � 1997: FDA permitted drug companies to advertise prescription drugs directly to the public � 1997 – 2004: Money on advertising quadrupled to $4. 35 Billion � 2000: Every dollar spent on advertising translated to an additional $4. 20 in sales � Profiting off of benefit and not just need � Most funding for mental health research comes from pharmaceutical companies � Few psychiatrists provide therapy, just prescribe medication � Payments from drug companies to doctors sways prescription patterns � Perpetual increase in “polypharmacy”
Talk-Therapy � Research shows strong evidence that talk therapy can be effective � About 75% report improvement: diminished symptoms and greater length of time between episodes � Two most critical predictors of success: 1. 2. Rapport Trust in framework being used by patient & therapist
Psychotherapy (Talk-Therapy) � Cognitive-Behavioral Therapy � � � Based on theory that negative thinking and habits drive anxiety/depression Alter thinking, self-beliefs, and behavior Limited focus on emotion Youth anxiety Psychodynamic Therapy Builds self-awareness and understanding of hidden/unresolved conflict & denied feelings to elicit change � Deeper understanding of emotion and it’s meaning � Less intensive than psychoanalysis � � Interpersonal Therapy � � � Communication Relationships Family Therapy
The Brain & Secrets � Keeping secrets may be unhealthy for the brain � Study- when subjects shared intimate secrets- health improved, doctor visits and stress hormones decreased � Competing operations (telling and withholding) may influence stress/inner tension � May explain the need for some to vent to strangers and the appeal of prayer/confession amongst religions � Venting a secret to an open ear (human or human-like) is the intervention and advice is not intended/needed
Psycho-Education with Youth � Fosters positive therapeutic relationship � Reduces self-blame & guilt � Instills hope � Increases motivation � Reduces anxiety � Promotes self help & reliance
School Supports � Adjusted school schedule � Staff support person � Lunch support group or social skills group � Time away in safe place � In-school counseling � Test accommodations/program modifications through 504 Plan/IEP � In severe cases: Home Instruction (short-term with plan for reintegration, only part-time if possible) � Special education programming
Relaxation Techniques � Yoga � Meditation � Mindfulness � Etc…
Treatment Challenges � Children & most adolescents don’t seek help on there own � Therapy cannot begin to be successful until a patient willingly accepts help � Alternative therapies (i. e. play therapy) can be helpful with young children � Asking a child to provide wishes or things they wish they had the power to change can provide much insight into a child’s view of self, life, and others � Parent anxiety and resistance
Problem Solving & Collaboration � Challenge to get all involved on the same page � Varying agendas and sense of urgency � Respect youth’s pace/comfort level � Communication and clear plan is needed for gradual exposure
Cost-Effective Approach Exercise Sleep Diet
Thoughts Emotions Behaviors Physical (Body) Symptoms
The Connection � The way we think effects the way we feel, behave, and how our bodies operate. � The opposite is also true- if we are physical ill or in pain it effects how we think, feel, behave. � Neurotransmitters: Ø chemicals in our bodies that play a role in our thoughts, feelings, and behaviors
Stress The most successful people I know have gotten there by choosing to underact to stressful conditions and keep moving forward. Lucinda Bassett
Stress � What is it? � Our response to external conditions (stressors) which effect our thoughts, feelings, and bodies � Stressors: � Adrenaline & Cortisol: chemicals that are released in our bodies when we experience stress
Emotional Symptoms � � � � � Nervousness Irritability Crying Anxiety Lack of motivation or excitement Angry outbursts Feeling powerless Easily upset Loneliness
Cognitive Symptoms � � � � Trouble thinking clearly Forgetfulness Lack of creativity Memory loss Inability to make decisions Constant thoughts of worry Racing thoughts or mind going blank Lack of sense of humor
Behavioral Symptoms � � � Bossiness Compulsive tendencies- repeating something over & over (eating, chewing gum, playing video games…. . ) Critical attitude of others Grinding teeth Not able to complete important tasks Smoking or abusing alcohol and drugs
Physical Symptoms � � � � Headaches Stomach aches and indigestion Sweaty palms Difficulty sleeping Dizziness Back pain Tight neck and shoulders � � � � Feeling nauseous Hot & Cold Flashes Numbness or strange aches/pains Chest pain Racing heart Restlessness Tiredness Frequent illness
Managing Stress � � � � � Change the way we think about certain situations or events Eat healthy and get good SLEEP Physical activity: exercise, sports, walking, weightlifting, etc… Relaxed breathing techniques Meditation Yoga / Tai Chi Talk to a trusted person Listening to or playing music Reading, drawing, & writing Spending time having fun with self or others
References � � � � Doidge, N. (2007), The Brain that Changes Itself. Eagleman, D. (2011), Incognito: The Secret Lives of the Brain. Pearrow, M. (2013), Students who Self-Injure: School-based Strategies Based on DBT, NASP Convention, Seattle, WA, Februay 15, 2013. Solomon, A. (2001), The Noonday Demon Burns, D. (2006) When Panic Attacks Bassett, L. (1995), From Panic to Power www. nydailynews. com (2013), One in five U. S. kids has a mental disorder; ADHD the most common: CDC, May 17, 2013 The Buffalo News (2013), Today’s Mental Health Squad: The Police, May 19, 2013. The Buffalo News (2013), Does Training Prepare Cops for the Mentally Ill, August 4, 2013. The Buffalo News (2013), Suburban Poverty on the Rise, June 8, 2013. Sharpe, K. (2012), Coming of Age on Zoloft: How Antidepressants Cheered Us Up, Let Us Down, and Changed Who We Are. Rapee, R. , Craske, M. , & Barlow, D. The Causes of Anxiety and Panic Attacks, http: //algy. com/anxiety/index. php. Pratt, D. (2012), Anxiety Disorders in Children & Adolescents (power point)