ANXIETY AND RELATED DISORDER II OBSESSIVE COMPULSIVE DISORDER

ANXIETY AND RELATED DISORDER -II
")
OBSESSIVE COMPULSIVE DISORDER (OCD)

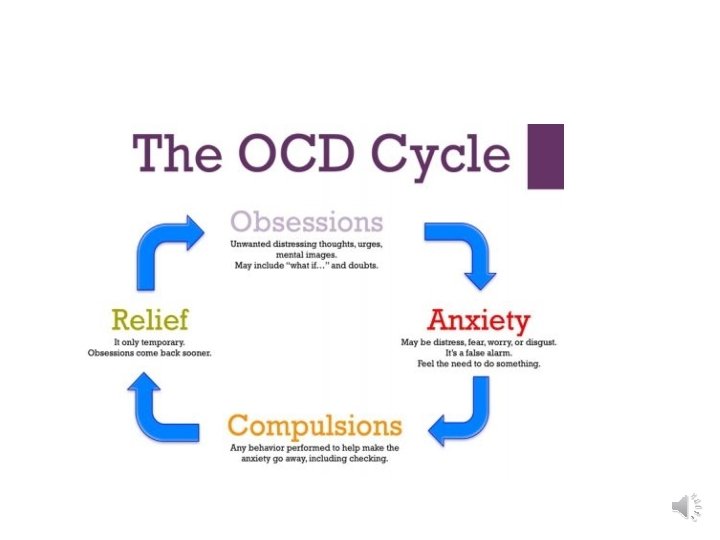
What is OCD? • Is a disorder characterized by recurrent , unwanted and seemingly bizarre thoughts , images , impulses , or doubts that evoke distress and repetitive behavioral and mental rituals performed to reduce this distress.

Obsessions? Compulsions? • Obsessions-recurrent persistent thoughts, images, or impulses that enter the mind despite efforts to exclude them. • Compulsions – repetitive and seemingly purposeful behaviors performed in a stereotyped way in response to an obsession

Obsessions - continued n Obsessions often accompanied by uncomfortable feelings such as fear, disgust, or doubt. n An obsession occurs when someone cannot get rid of a content of consciousness, although when it occurs he/she realizes that it is senseless/absurd or at least it is dominating and persisting n For example, people with OCD may worry excessively about dirt and germs, and obsessed with the idea that they are contaminated or may contaminate others

Compulsions • These are acts that are continually and deliberately performed to provide relief from discomfort caused by obsessions. • OCD compulsions do not give the person pleasure (unlike drinking, gambling, etc. ). • For example, a person may repeatedly check to see if their stove was left on checking the lock in the house.

Common Symptoms Common Obsessions Common Compulsions - Contamination fears of germs, dirt, etc. - Washing. - Imagining having harmed self or others. - Repeating. - Imagining losing control of aggressive urges. - Checking. - Intrusive sexual thoughts or urges. - Touching. - Excessive religious or moral doubt. - Counting. - Frobidden thoughts. - Ordering/Arranging. - A need to have things “just so”. - A need to tell, ask, and confess. - Hoarding or saving. - Praying.

Epidemiology of OCD n The life time prevalence in general population is between 2 and 3 percent n It is considered the fourth most common psychiatric condition, ranking after phobias, substance abuse disorders, and major depressive disorder.

Gender & Culture Ø Men and women are equally likely to be affected , but among adolescents slight male predominance. Ø The mean age of onset is about 20 years, although men have slightly earlier age of onset(about 19 years) than women (about 22 years) Ø Single people are more commonly affected , representing the difficulty people of OCD to maintain a relationship Ø OCD is more common in whites than African American children in clinical samples. However, epidemiologic data suggest no differences in prevalence as a function of ethnic group or geographic region. Ø OCD tends to go under-diagnosed and under-treated because people with the illness often act secretive about their symptoms.
 Major Depression (67%) Tourette’s Syndrome(5 -7%) Eating disorder Hypochondriasis")
Co-Morbid Disorders Phobias-social phobia (25%) Major Depression (67%) Tourette’s Syndrome(5 -7%) Eating disorder Hypochondriasis Impulse Control Disorder Panic Disorder PTSD Alcohol use disorders Generalized Anxiety Disorder Delusional Disorder Obsessive Compulsive Personality disorder

OCD and schizophrenia • About 25% of patients with chronic schizophrenia may also present with OCD symptoms (range 5 - 45%) and 15% of the patients with schizophrenia may fully qualify for the diagnosis of OCD. • The presence of OCD in schizophrenia predicts a poor prognosis • So , several studies among patients with schizophrenia and OCD reported an improvement in OCD symptomatology after the addition of SSRIs

What Causes OCD? Biological factors : Neurotransmitters 1. Serotonergic system : Abnormality of the Serotonergic system and particularly the hypersensitivity of postsynaptic 5 -HT receptors , constitutes the leading hypothesis for the underlying pathophysiology of OCD

Noradrenergic/dopaminergic system § Currently less evidence exists for dysfunction in the noradrenergic system in OCD § The most compelling evidence for dopaminergic involvement comes from the abundance of OCD symptoms in basal ganglia disorders , such as Tourette’s syndrome , Syndenham’s chorea and post encephalitic parkinsonism

Genetic studies • Relatives of probands with OCD consistently have 3 -5 fold higher probability of having OCD than families of control probands • Of the first degree relatives of patients with childhood onset OCD, 35% are also afflicted with the disorder. • Significantly higher concordance rate was found for monozygotic twins than for dizygotic twins.

Infection Causes • Recent research suggests that some children with OCD develop the condition after experiencing a type of streptococcal infection • This condition is referred as PANDAS (Paediatric Autoimmune Neuropsychiatric Disortder Associated With Group A Streptococcus ) • Its hallmark is a sudden and abrupt exacerbation of OCD symptoms after a strep infection. • The cause of this form of OCD appears to be antibodies directed against the infection mistakenly attacking a region of the brain and setting off an inflammatory reaction.

Brain imaging studies Ø The use of PET scan has demonstrated presence of increased activity (i. e metabolism and blood flow) in the frontal lobes, the basal ganglia (specially caudate nucleus)and the cingulum. Ø Both CT and MRI studies have shown decreased sizes of caudate lobe bilaterally. Ø Overall , brain imaging research suggests a role for the prefrontal cortex- basal ganglia thalamic circuitry.

Behavioral factors n According to learning theory , obsessions are conditioned stimuli. n Neutral stimulus + anxiety provoking stimulus = produce anxiety when presented alone n Consequently , avoidant behavior is being adopted in order to avoid the anxiety provoking stimulus and other stimulus n The compulsions are learnt as a way to reduce anxiety n The relief serves as reinforce to the compulsion and repeated by the patients. n Through the process of conditioning , reward and reinforcement , rituals and avoidant strategies are become fixed.

Psychological factors Ø The dynamic aspects of OCD were first described by Sigmund Freud , who coined the term ‘obsessional neurosis’ Ø The disorder was thought to result from regression from the oedipal phase to the anal phase with its characteristic ambivalence. Ø Freud believed the need to be clean and not to touch is related to anal sexuality. Ø Defense mechanisms: Isolation , Undoing and Reaction formation

DIAGNOSIS AND DIFFERENTIAL DIGNOSIS
, present on most days for")
ICD-10 Criteria A. Either obsessions or compulsions (or both), present on most days for at least 2 successive weeks and be a source of distress or interference with activities. B. The obsessional symptoms should have the following characteristics 1. They must be recognized as the individual’s own thoughts or impulses; 2. There must be at least one thought or act that is still resisted unsuccessfully, even though others may be present which the sufferer no longer resists; 3. The thought of carrying out the act must not in itself be pleasureable (simple relief of tension or anxiety is not regarded as pleasure in this sense); 4. The thoughts, images, or impulses must be unpleasantly repetitive.
 - Basal ganglia diseases(Syndenham;")
Differential diagnosis MEDICAL CONDITIONS : -Tic disorders (especially Tourette’s syndrome) - Basal ganglia diseases(Syndenham; s chorea , Huntinton’s disease) - Temporal lobe epilepsy -Head trauma - Post encephalitic complications PSYCHIATRIC DISORDERS : - Major depression -Schizophrenia -OCPD -PTSD -Phobias -Delusions -Hypochondriasis -Paraphilias

Course and prognosis v Typically begins in late adolescence , although onset in childhood is not uncommon. v Tends to exhibit waxing and waning course over the lifespan while others experience chronic course. v Many patients with OCD may have onset of symptoms after a stressful event (e. g. pregnancy, a loss, or a sexual problem). v About : 20 -30% show significant in their symptoms 40 -50% show moderate improvement 20 -40% become chronic or their symptoms worsen

Prognostic factors Poor prognosis -early onset -male gender -tic related forms of OCD with associated to hoarding /symmetry compulsions -need for hospitalization -psychotic features -coexisting MDD -delusional beliefs -Presence of personality disorder(specially Schizotypal PD) Good prognosis : good social and occupational adjustment and less avoidance The obsessional content does not seem to be associated to the prognosis except for hoarding (less favorable outcome )

Treatment 1. Pharmacological 2. Psychological

Treatment Considerations n Use of both medication and psychotherapy results in a better outcome than use of either alone. n Many patients have somatic complaints (eg, fatigue, pain, hypochondriacal symptoms, excessive worrying, chronic sadness). Thus, a comprehensive medical evaluation is essential to rule out any preexisting medical and psychiatric condition.

Pharmacological • Two categories of drugs have been mainly studied for the treatment of OCD : TCA (clomipramine )and SSRIs (fluoxetine, paroxetine , sertaline citalopram and escitalopram). • Doses of SSRIs should be higher than that used for treating depression(e. g. 40 -60 mg of fluoxetine, 200 mg – 300 mg of clomipramine)

Ø Other pharmacological approaches and neurosurgery - Clonazepam has been reported efficient in several uncontrolled studies and case series however the long term use raised questions of dependency - Adding drugs that affect dopamine function , especially the atypical antipsychotics to SSRI therapy in patients with treatment resistant OCD may result in improvement for pts. with family history of tics.

Neurosurgery and Deep Brain stimulation : • Have been reported to be effective in some patients with OCD. • Neurosurgery involves procedures that disconnect the outflow pathways originating from the orbitofrontal cortex. • Cingulotomy can help some intractable patients , but although the immediate results may be striking , the long term prognosis is more reserved

Psychological approach
 • The best established psychological intervention for OCD is behaviour")
Cognitive Behavioural Psychotherapy (CBT) • The best established psychological intervention for OCD is behaviour therapy including exposure to ritual provoking stimuli and response prevention often called ERP • Exposure – person remains in contact with something they usually fear until their anxiety is diminished. • Response intervention – person’s rituals or avoidance behaviours are blocked (those afraid of germs are not only exposed to germs but refrained from ritualized washing). • Exposure is usually more helpful in decreasing anxiety and obsessions, while response intervention is better at decreasing compulsive behaviours.
 • Techniques used – Desensitization, -Thought stopping , -Flooding , -Aversion conditioning")
CBT (Cont’d) • Techniques used – Desensitization, -Thought stopping , -Flooding , -Aversion conditioning • Patients who complete CBT report a 50 -80% reduction in OCD symptoms after 11 -20 sessions.

POST TRAUMATIC STRESS DISORDER
 • PTSD develops as intense and prolonged emotional responses")
POST TRAUMATIC STRESS DISORDER (PTSD) • PTSD develops as intense and prolonged emotional responses after experiencing or witnessing exceptionally traumatic or stressful events, that involve threatened or actual death or a serious threat to physical or emotional integrity. • The person experiences intense fear, horror and helplessness. • Symptoms generally develop within days or weeks but in some cases after months or years, in the form of delayed and atypical PTSD

Diagnostic criteria I. II. III. IV. The person experienced, witnessed or was confronted with an events or events that involved actual or threatened death/serious injury/threat to physical integrity of self or others. Traumatic event is re-experienced. - Recurrent & intrusive distressing recollections - Dreams - Acting or feeling as if traumatic events are recurring. - Intense psychological distress at exposure to internal on external cues that reasonable aspect of traumatic events. Traumatic events avoidances. Autonomic hyperarousal
 a) Exposure to traumatic events. b) Traumatic event re-experienced. c)")
Post Traumatic Stress Disorder(PTSD) a) Exposure to traumatic events. b) Traumatic event re-experienced. c) Avoidance of traumatic stimuli & numbing of general responsiveness. Avoids thoughts, feelings or conversations. Avoids activities, places or people. Inability to recall important aspect of trauma. ↓ interest in other activities.
 Increased arousal. - Sleep disturbance. - Irritability. - Difficulty concentrating. . - Hyper")
d) Increased arousal. - Sleep disturbance. - Irritability. - Difficulty concentrating. . - Hyper vigilance. - Exaggerated startle response. Acute Less than 3 months. Chronic More than 3 months.

D/D 1. 2. 3. 4. 5. 6. Depression Panic Disorders GAD Agoraphobia Dissociative Disorder Facticitous disorder or malingering. Etiology: Preceded by trauma.

Predisposing vulnerability factors in PTSD • Presence of childhood trauma • Borderline, paranoid, dependent or antisocial personality disorder traits • Inadequate family or peer support • Being female • Genetic vulnerability to psychiatric illness • Recent stressful life changes • Substance abuse

Management • Investigation Same as in GAD. • R/O Head injury Malingering Treatment Biological same as in GAD.
 PROGRESSIVE MUSCLE")
PSYCHOLOGICAL TREATMENT SUPPORTIVE PSYCHOTHERAPY GRADED EXPOSURE ( IMAGINAL AND/OR IN VIVO ) PROGRESSIVE MUSCLE RELAXATION COGNITIVE RESTRUCTURING THOUGHT STOPPING EMDR (EYE MOVEMENT AND DESNSITIZATION AND REPROCESSING) GROUP THERAPY PHARMACOLOGICAL TREATMENT same as in GAD.

THANK YOU
- Slides: 43