ANTIPLATELET AND ANTICOAGULANT Dr Chirag Patel Classification of
















 Thrombocytopenia: platelet < 1 lac/mic. l or more than")








- Slides: 28
ANTIPLATELET AND ANTICOAGULANT Dr Chirag Patel
Classification of anti-platelet drugs
Anti-platelet drug: Mechanism of Action
Aspirin Produce antithrombotic effect by inhibiting platelet COX-1, used in biosynthesis of TXA 2. Widely use in AMI, CVA, PVD Dosage: 75 -325 mg/day Gastritis , peptic ulcer, bleeding are common side effects Poor absorption, drug interaction, over expression of COX 2 leads to Aspirin resistance
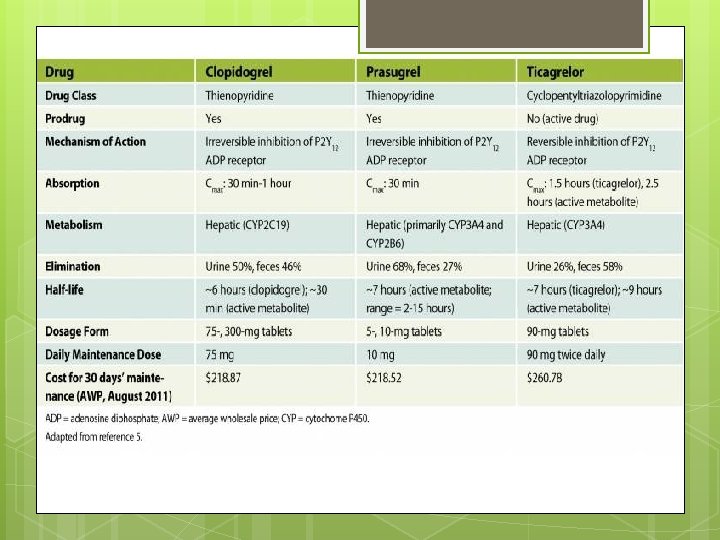
Clopidogrel Irreversibly blocks P 2 Y 12 component of ADP receptors, preventing activation of GP ll B/ lll. A complex & reduce platelet aggregation. Use in AMI, stroke, PVD, CAD Discontinuation of drug may cause stent thrombosis and subsequent AMI. § § Drug eluting stent- min. for 12 months Bare metal stent- min. 1 month Contraindicated in active bleeding Interaction with warfarin, omeprazole Loading dose 300 mg, f/b 75 mg od Resistance by CYP pleomorphisam
Prasugrel Inhibits platelet activation and aggregation through irreversibly binding its active metabolite to P 2 Y 12 ADP-receptor on platelet. Loading dose of 60 mg and followed by 10 mg od. Contraindicated in age>75 yrs, weight < 60 kg, history of TIA/CVA/ICH, ( risk of bleeding is more comparatively), End stage renal disease
Ticagrelor Orally active inhibitor of P 2 Y 12 Not a prodrug and its reversible inhibition of ADP receptor Rapid onset and offset of action In Studies found Ticagrelor is superior toclopidogrel for AMI. Dosage; loading dose 180 mg, followed by 90 mg bd.
Dipyridamole Coronary vasodilator and weak anti platelet drug Potentiates effect of endogenous prostacycline and in high conc. Inhibits phosphodiesterase so increase c AMP Used with Aspirin to prevent ischemic stroke in pts of TIA.
GP ll B/ lll A Receptor antagonists includes- Abciximab, Eptifibatide, Tirofiban which targets GP ll B/lll A recept. Mainly used in pts. Undergoing PCI and risk pts. With unstable angina. Renal dosage adjustment required in Tirofiban & with Eptifibatide.
Gp 2 b
Dosing of GP ll B/lll A Tirofiban: § § Loading dose: 25 mcq/kg infused in 5 min then infusion 0. 15 mcq/kg/min upto 18 hrs. if Cr. Cl < 60 ml/min : decrese post loading dose infusion by 50% to 0. 075 mcq/kg/min Eptifibatide: § § 180 mcq/kg iv bolus over 1 -2 min then 2 mcq/kg/min iv upto 12 hrs. If Cr. Cl < 50 ml/min then post loading dose would be 1 mcq/kg/min with additional bolus of 180 mcq/kg/min 10 min. after 1 st dose Abciximab: 0. 25 mg/kg iv bolus over 1 min. 10 -60 min before PCI then 0. 125 mg/kg/min iv infusion for 12 hrs.
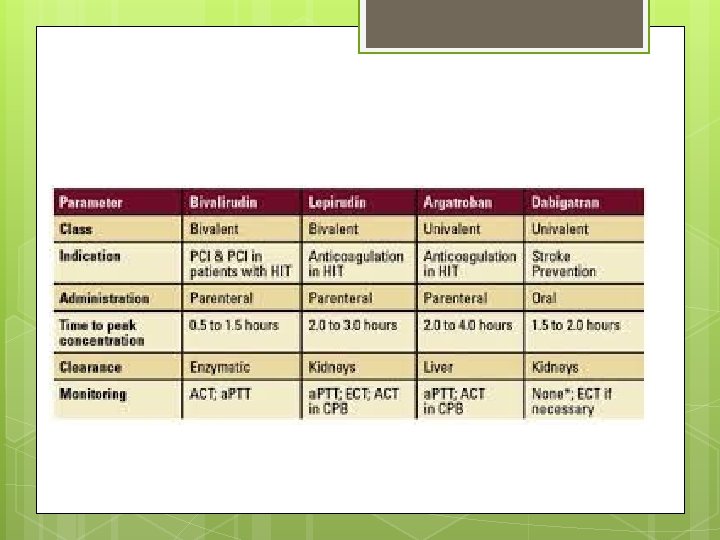
Anticoagulant drugs Parentral anticoagulants § Heparin, LMWH § Fondaparinux § Direct thrombin inhibitor: Lepirudin, Desirudin, Bivalirudin, Argatroban Oral anticoagulants § Warfarin § Thrombin inhibitor: Dabigatran § Xa inhibitor: Rivaroxaban, Apixaban, Edoxaban
Anti Coagulant Uses Aim to prevent thrombus extention & embolic complications by reducing rate of fibrin formation Uses: § § § § DVT, Pulmonary embolism Myocardial infarction Unstable angina Rheumatic heart dis. - atrial fibrillation Cerebrovascular disease Vascular Sx. , Prosthetiv heart valves Hemodialysis
Parentral anticoagulant HEPARIN Anticoagulant effect by inactivating thrombin & factor Xa through antithrombin Peak plasma time: 2 -4 hrs. T-half: 60 -90 min, longer at high doses Metabolised partially in liver and RES Monitored by a. PTT, ACT. Effect reversed by protamine sulfate, 1 mg= 100 u of heparin Safer in pregnancy
HEPARIN For DVT & PE prophylaxis: 5000 U BD/TDS For Rx. : 80 u/kg iv bolus, Then continuous infusion of 18 u/kg/hr Dose should be adjuted to maintain a PTT Of 50 -70 sec. For STEMI: iv bolus 60 -70 u/kg (ma. 5000 u) then 12 -15 u/kg/hr (max. 1000 u/hr)
Heparin-Adverse effects Hematoma, hemorrhage Local irritation, erythema Anaphylaxis, Increased liver enzymes Osteoporosis Contraindication: § § h/o heparin induced thrombocytopenia Uncontrolled active bleeding
Heparin induced thrombocytopenia (5 T’s) Thrombocytopenia: platelet < 1 lac/mic. l or more than 50% reduced from baseline Timing: platelet count falls after 5 -10 days of therapy Thrombosis: venous > arterial thrombosis Type of pt. : m/c in surgical & cancer pts. than general pts. Female > men affected Type of heparin: UFH > LMWH
HIT diagnosis & management Anti PF-4/heparin antibody Platelet activating Ig. G Abs. Manage by stop all heparin § § Alternative use of Lepirudin, Argatroban, Bivalirudin, Fondaparinux Not to give platelet transfusion Search for thrombosis (DVT) Don’t give warfarin till platelet count reaches baseline level.
Low Molecular Weight Heparin Acts by activating antithrombin, but more affinity for Xa than thrombin Not required monitoring Better bioavailability Longer & predictable half life Llow risk for HIT & osteoporosis Dose independent clearance Examples: Enoxaparine-40 mg s/c, & Dalteparin- 2500 -5000 anti-Xa U q 24 hr prophylactic dosage.
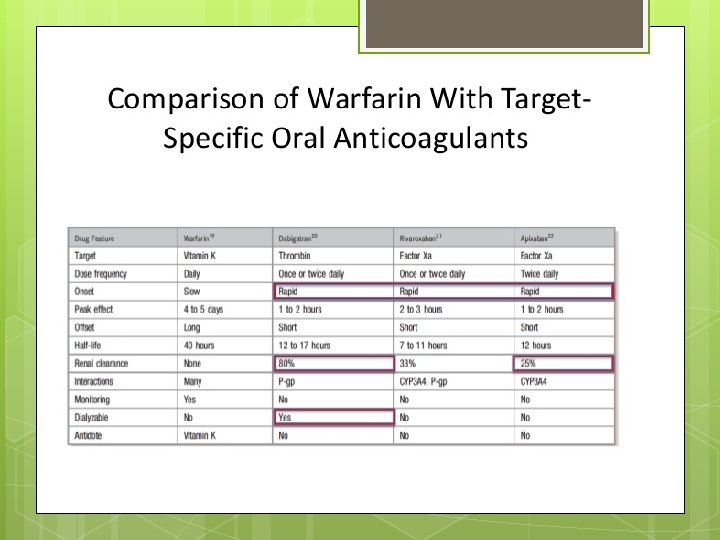
Oral Anti Coagulant Warfarin Interferes with synthesis of vit k dependant clotting factorsfactor ll, Vll, lx, x synthesis of vit k dependant protein C & S reduced Coagulation monitoring required bcs of variable response, targeting INR- 2 -3 Narrow therapeutic range Contraindicated in bleeding disorders and in pregnancy To be stopped 5 days before elective surgery Atleast 5 day course of parentral anti Coagulation recommended to ensure that levels of factor Xa & prothrombin reduced.
Newer Oral Anti Coagulant Advantages: § § § Rapid onset of action } no need for bridging Predictable anticoagulant effect } no need for routine monitoring Specific coagulation enzyme target } low risk of off-target adverse effect Low food interaction } no dietary restriction Low drug interactions
Uses Dabigatran, rivaroxaban & apixaban are used for alternative for stroke prevention in non valvular heart disease Rivaroxaban, apixaban approved for use in elective hip/ knee arthroplasty Rivaroxaban and dabigtran licensed for rx. Of DVT & PE.
Dosing Stroke prevention: § Rivaroxaban: 20 mg od § Dabigatran: 150 mg bd § Apixaban: 5 mg bd For DVT/ PE Rx. : § Rivaroxaban 15 mg bd for 3 wks then 20 mg od Post Sx. Prophylaxis: § Rivaroxaban : 10 mg od § Apixaban: 2. 5 mg bd
Newer Anti Coagulant Monitoring § § usually not required For Xa inhibitor: a PTT Dabigatran: PT Bleeding (G. I. )is major complication but less in comparison to warfarin. Antidote not available Contraindicated in pregnancy Renal clearance needed.
Thank You