ANTIPHOSPHLIPID SYNDROME INTRODUCTION The antiphospholipid syndrome APS is

 is defined by two major components (see 'Classification criteria'")

 CNS Hematologic manifestations Cutaneous Renal disease Pregnancy loss")










 Ø Embolic")



- Slides: 25
ANTIPHOSPHLIPID SYNDROME
INTRODUCTION The antiphospholipid syndrome (APS) is defined by two major components (see 'Classification criteria' below: • The occurrence of at least one clinical feature: vascular event or pregnancy morbidity AND • The presence of at least one type of autoantibody known as an antiphospholipid antibody (a. PL). •
§ § § APL are directed against serum proteins bound to anionic phospholipids and may be detected by a: Anticardiolipin antibody ELISA Anti-ß 2 glycoprotein-I ELISA Lupus anticoagulant tests The full clinical significance of other autoantibodies, including those directed against prothrombin, annexin V, phosphatidylserine, and phosphatidylinositol, remain unclear.
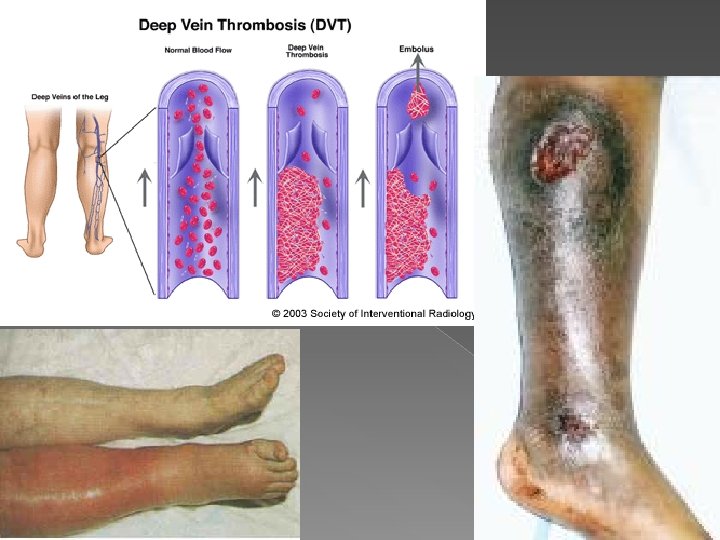
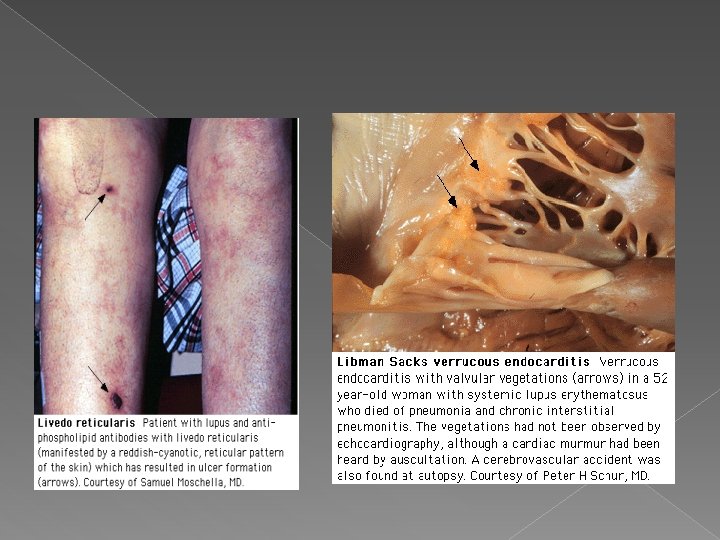
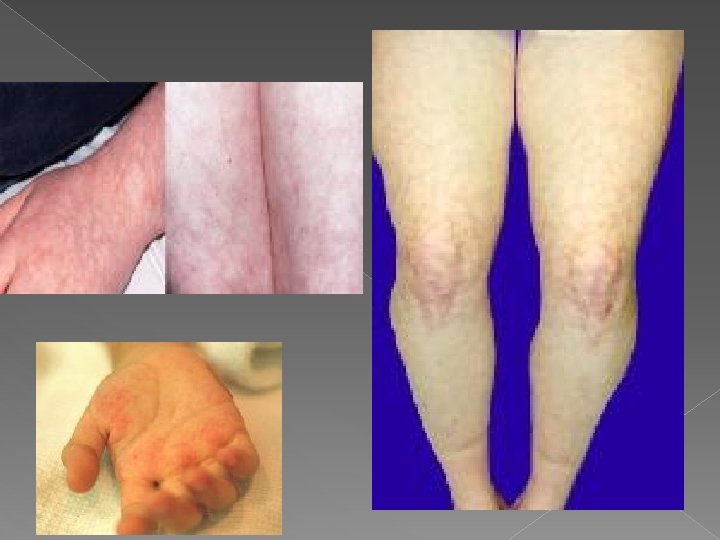
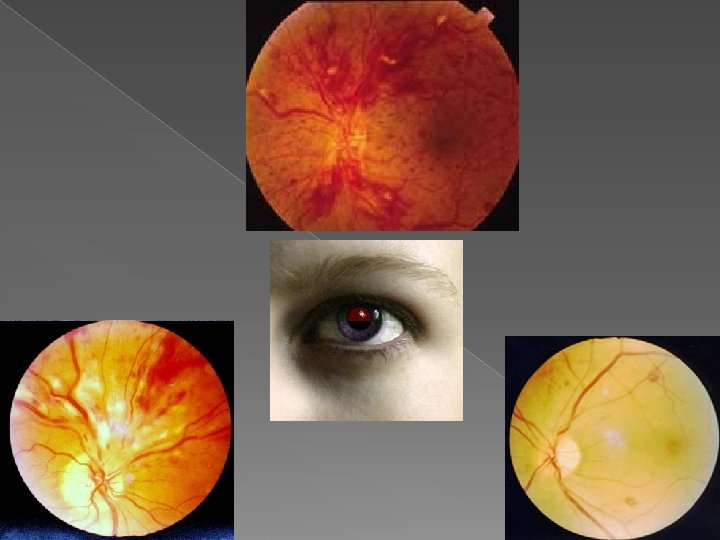
CLINICAL MANIFESTATIONS Cardiovascular Thrombosis (A, V) CNS Hematologic manifestations Cutaneous Renal disease Pregnancy loss Ocular manifestation s Gastrointest inal disease Adrenal disease Osteonecrosis — Pulmonary disease
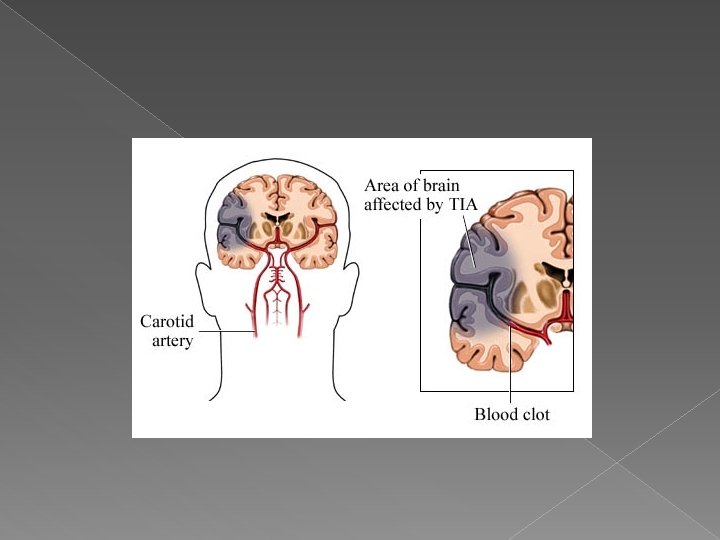
APAS � The most common site of DVT is the calf � The most common site of arterial thrombosis is the cerebral circulation � The initial and long-term manifestations of the disease are similar: in most, but not all the initial arterial thrombosis tends to be followed by an arterial event and the initial venous thrombosis by a venous event � Venous thrombosis are more common than arterial thrombosis
Catastrophic APS A small subset of patients with APS has widespread thrombotic disease with multiorgan failure, which is called "catastrophic APS. “ Patients with catastrophic APS may have laboratory features such as elevated fibrin degradation products, depressed fibrinogen levels, or elevated D-dimer concentrations that are more typically found with disseminated intravascular coagulation (DIC).
Diagnostic criteria The American College of Rheumatology proposed preliminary clinical classification criteria at Sapporo in 1999 but these were updated in Sydney in 2006. � At least 1 clinical criterion and 1 laboratory criterion must be present for a patient to be classified as having APS. � The laboratory results should be found at least 12 weeks after the clinical event; otherwise the event may produce a false positive result. �
Clinical criteria fall into two groups: Vascular thrombosis: › There must be one or more episodes of arterial, venous or small vessel thrombosis in any tissue or organ. › Objective criteria must be used to make the diagnosis. This includes imaging and histopathology but for the latter, there should be no significant evidence of inflammation of the vessel wall.
� Pregnancy morbidity: either, › One of more unexplained deaths of a morphologically normal fetus at the 10 th week of gestation or beyond. This should be confirmed by ultasound or post mortem examination. › One or more premature births of a morphologically normal baby before the 34 th week of gestation because of: �Severe pre – eclampsia or eclampsia, or �Placental insufficiency › Three or more unexplained consecutive spontaneous abortions with exclusion of gynaecological abnormalities or hormonal inadequacy as the cause and normal chromosomes in both parents. › Some patients may have features from more than one of these pregnancy criteria.
Laboratory criteria § Lupus anticoagulant; this should be found in plasma on at least 2 occasions at least 12 weeks apart. § Anticardiolipin antibody (a. CL); the a. CL antibody may be Ig. G or Ig. M. The titre should be medium or high being at least 40 GPL or MPL or above the 99 th centile. This should be on two or more occasions at least 12 weeks apart. § Anti-β 2 glycoprotein-I antibody; this can also be Ig. G or Ig. M and in a titre above the 99 th centile on two or more occasions at least 12 weeks apart.
Other laboratory features include Ig. A a. CL, Ig. A anti-β 2 GPI Antiphosphophatidylserine antibodies Antibodies against prothrombin (a. PT-A) Antibodies to the Anti-β 2 glycoprotein-I Antibody/anti-prothrombin (a. PS/PT) complex.
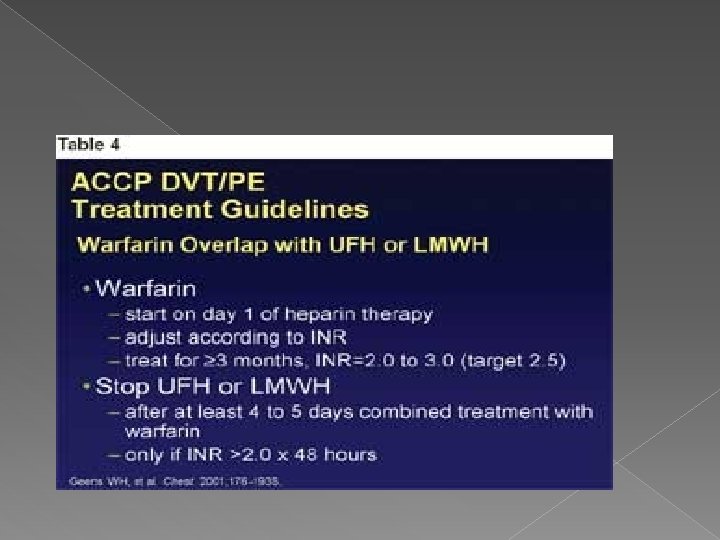
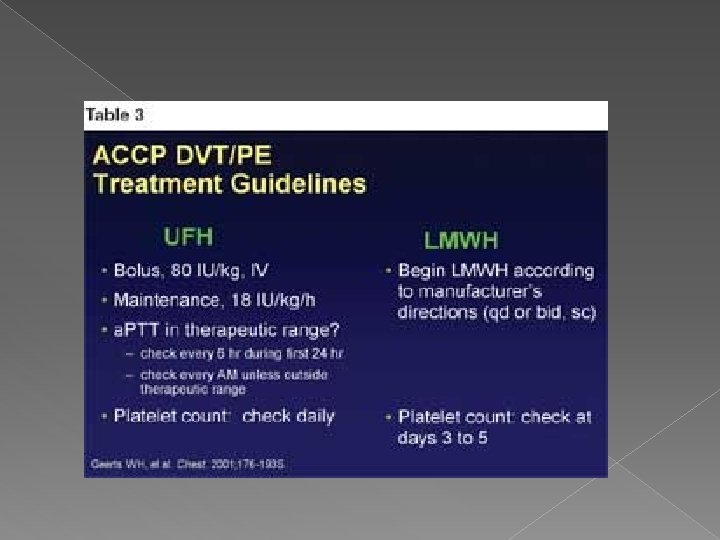
APS Treatment The therapy for the APS is largely the same regardless of whether the disorder is classified as primary APS or as being secondary to SLE. Current therapies for the APS include the following HEPARIN - Low molecular weight heparin - Unfractionated heparin WARFARIN Antiplatelet agents - Asprin - Clopidogrel Hyroxychloroquine
Therapeutic options for recurrent thromboembolism in APS Warfarin with a higher target INR (> 3. 0). Ø Addition of an antiplatelet agent to warfarin. Ø Change to an alternative anticoagulant (e. g. , low molecular weight heparin). Ø Immunomodulatory therapy Ø
Treatment of cardiac involvement Asymptomatic valve thickening: low dose aspirin (81 mg/d) Ø Embolic disease: Heparin followed by warfarin Ø MI: Heparin followed by warfarin + aspirin Ø
ACCP Guidelines: Pregnancy and a. PL Manifestation Recommendation Antiphospholipid antibody; no prior VTE or pregnancy loss. Surveillance, or mini-dose heparin, or prophylactic LMWH, &/or aspirin Antiphospholipid antibody; prior thrombotic event Adjusted dose UFH or LMWH, plus low-dose aspirin
References : Uptodate ü ACCP ü Emedicine ü
DONE BY OLA TARABZUNI 2/11/2010