Antimicrobial Stewardship Penicillin Allergies Emmanuel Cacio Pharm D

Antimicrobial Stewardship: Penicillin Allergies Emmanuel Cacio, Pharm. D – PGY 1 Pharmacy Resident

Objectives • Describe the incidence of penicillin allergies • Illustrate the role of the pharmacist in appropriate interventions in patients with penicillin allergies • Recognize when to recommend pharmacist intervention in patients with self-reported penicillin allergies • Illustrate the importance of properly documenting patient self-reported penicillin allergies

http: //www. toothpastefordinner. com/032307/
: • 10% Americans")
Introduction 1 Per the Center for Disease Control and Prevention (CDC): • 10% Americans report penicillin allergy • Fewer than 1% are truly allergic • 80% with Ig. E-mediated response lose sensitivity after 10 years
 Reactions 1 • Occur immediately or within the hour •")
Ig. E (Type I) Reactions 1 • Occur immediately or within the hour • Hives: pink/raised areas, itchy • Angioedema • Wheezing & shortness of breath • Anaphylaxis
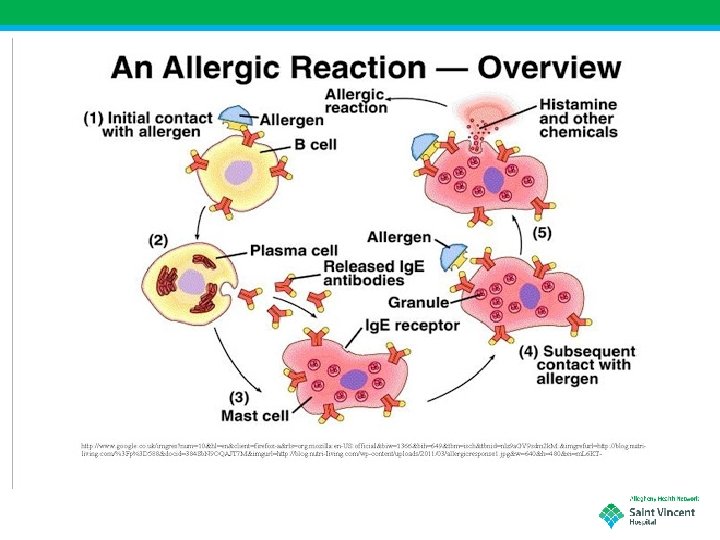

Anaphylaxis 2 • Sudden mast cell release that leads to sudden drop in: • Blood pressure • Blood volume • • • Flushing Itching Potential respiratory compromise Bowel edema Potential death

Documented Non-Anaphylactic Penicillin Allergies • • • Rash Nausea Diarrhea Not documented “I don’t remember…” “My mother told me not to take it”

The Problem… 3 • Alternative antimicrobial therapies are used • Tend to have more toxicities • i. e. Clostridioides difficile • Increased cost • Broader spectrum leading to poor outcomes • Resistance
 are responsible for more than 2 million")
The Problem… 3 • Multi-drug-resistant organisms (MDROs) are responsible for more than 2 million infections and result in 23, 000 deaths annually in the USA per the CDC • 2018 Report by Burnham and colleagues estimates that MDRO deaths actually reached 150, 000 • MDROs are expected to reach 10 million patients world-wide and cost over $100 trillion annually by year 2050

Appropriate AMS Interventions for Self. Reported Penicillin Allergies • Patient education • Allergy clarification • Penicillin Skin Testing

Patient Education 4 • Study in France targeted pregnant women with self reported penicillin allergies • Aim was to optimize prescribing of antibiotics for pregnant women • Two strategies were used: • Dissemination of printed educational material • Group education

Patient Education 4 • Study found: • Prevalence of self reporting penicillin allergy remained stable (6. 8% vs. 5. 4% after) • Clinical classification on penicillin allergy were more often used (68% vs. 100% after) • Appropriateness of antibiotics prescribed to self-reported penicillin allergic women increased from 17. 2% to 66. 7% (p<0. 001)
3 • Optimal way to rule out penicillin allergy • Time")
Penicillin Skin Testing (PST)3 • Optimal way to rule out penicillin allergy • Time consuming • Requires trained staff • Sacco et al. used a single-center allergistperformed PST • 78% of patients were able to receive betalactams after PST
3 • Median time was 5 days • Delayed time to")
Penicillin Skin Testing (PST)3 • Median time was 5 days • Delayed time to optimal therapy • Hospital protocol could expedite patient identification and allergist consultation for PST • Pharmacists have been identified as key providers of PST when allergist are unavailable.
3 • PST by allergist or pharmacist has potential for: •")
Penicillin Skin Testing (PST)3 • PST by allergist or pharmacist has potential for: • Reducing broad-spectrum antibiotic use • Allergy de-labeling after ruling out Type 1 reactions • Reduce outpatient prescription cost by $14 -193 per patient
5 • In 2014 over 35 million inpatient stays were documented")
Penicillin Skin Testing (PST)5 • In 2014 over 35 million inpatient stays were documented in the US • Diagnosis of septicemia and pneumonia ranking 3 rd and 6 th • In 2004 first published evidence of pharmacist involvement in inpatient PST • National certificate program newly available

https: //dailymed. nlm. nih. gov/dailymed/drug. Info. cfm? setid=2 fbcc 40 c-f 102 -4 abe-bce 5 a 93 de 95874 fe
: Procedure • Collect supplies: • 5 testing devices • Alcohol")
Penicillin Skin Testing (PST): Procedure • Collect supplies: • 5 testing devices • Alcohol swab • 4 syringes with: • • Pre-pen solution 0. 2 cc Pen. G dilution 0. 2 cc Histamine 0. 1 cc Saline 0. 2 cc • Labels • Recording form
: Procedure • Wipe volar aspect of arm with alcohol swab")
Penicillin Skin Testing (PST): Procedure • Wipe volar aspect of arm with alcohol swab • Label 4 sections for: • Histamine (+) • Saline (-) • PG • PRP • Drop test materials on skin
: Procedure • Wait 15 minutes • Analyze results • Positive:")
Penicillin Skin Testing (PST): Procedure • Wait 15 minutes • Analyze results • Positive: • PG (+) wheal ≥ 3 mm -or • PRP (+) wheal ≥ 3 mm • Negative: • PG (-) wheal ≤ 3 mm -and • PRP (-) wheal ≤ 3 mm

https: //www. penallergytest. com/

Conclusion • Approximately 99% of patients with self-reported penicillin allergies do not have true allergies • It’s been shown that patient’s receiving alternate therapies due to false or inaccurately classified penicillin allergies receive less than optimal care • Pharmacists and pharmacy technicians can play a significant role in determining and assessing the severity of these allergies and de-labeling as appropriate
. Is")
References 1. 2. 3. 4. 5. Center for Disease Control and Prevention (CDC). Is it Really a Penicillin Allergy? https: //www. cdc. gov/antibiotic-use/community/pdfs/penicillinfactsheet. pdf Bhattacharya, S. The Facts About Penicillin Allergy: A Review. J Adv Pharm Technol Res. 2010 Jan-Mar; 1(1): 11 -17 Cole, K. ; Rivard, K. ; Dumkow, L. Antimicrobial Stewardship Interventions to Combat Antibiotic Resistance: an Update on Targeted Strategies. Current Infectious Disease Reports. 2019; 21: 33 Thellier, C. , et al. An educational intervention about the classification of penicillin allergies: effect on the appropriate choice of antibiotic therapy in pregnant women. Int J Obstet Anesth (2019), https: //doi. org/10. 1016/j. ijoa. 2017. 005 Justo, JA; Kufel, WD; Avery, L; Bookstaver, PB. Penicillin Allergy Skin Testing in the inpatient Setting. Pharmacy 2019, 7, 120

https: //www. cartoonstock. com/directory/h/hospital_restaurant. a sp
- Slides: 25