ANTIMICROBIAL DRUGS ANTIMICROBIAL DRUGS Antimicrobial Drugs Different types

ANTIMICROBIAL DRUGS

ANTIMICROBIAL DRUGS

Antimicrobial Drugs �Different types of antimicrobial drugs: �Antibacterial drugs �Antifungal drugs �Antiprotozoal drugs �Antihelminthic drugs

Features of Antimicrobial Drugs: Antimicrobial Action �Bacteriostatic: inhibit growth of microorganisms �Bactericidal: Kill microorganisms


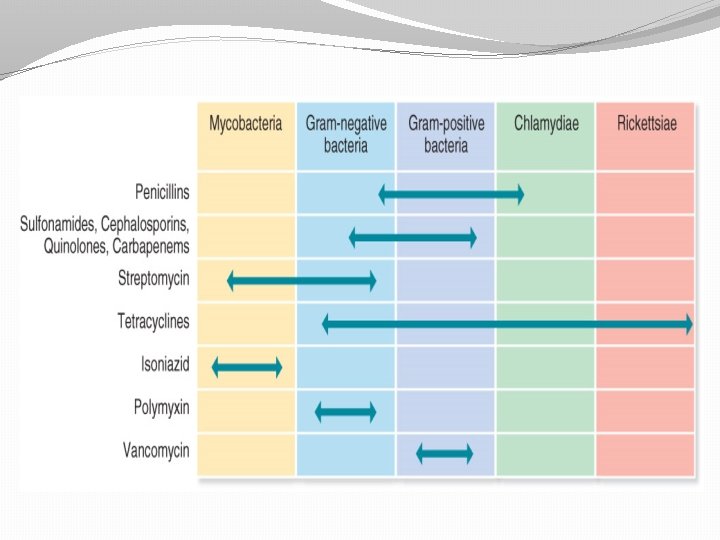
Features of Antimicrobial Drugs: Spectrum of Activity �Antimicrobial medications vary with respect to the range of microorganisms they kill or inhibit �Some kill only limited range : Narrow-spectrum antimicrobial �While others kill wide range of microorganisms: Broad-spectrum antimicrobial

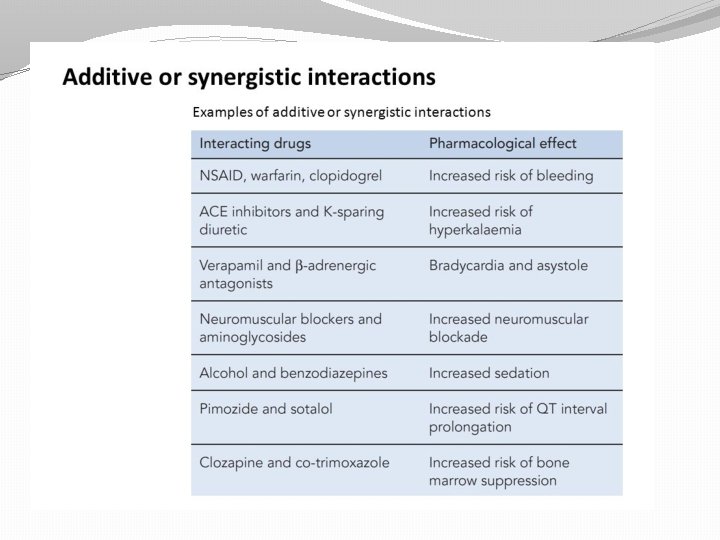
Features of Antimicrobial Drugs: Effects of Combining Drugs �Combinations are sometimes used to fight infections �Synergistic: action of one drug enhances the activity of another �Antagonistic: activity of one drug interferes with the action of another.
 together with Penicillin (bacteriocidal)? What")
Antagonism �Lets see, what if I give Tetracycline (bacteriostatic) together with Penicillin (bacteriocidal)? What will happen? Are they synergizing each other, or antagonizing each other? Ok, let us take one step at a time; we try to enumerate the mechanism of action of Tetracycline and Penicillin separately
 It acts by inhibiting 50 S ribosomal subunit and inhibiting the binding")
�Tetracycline 1) It acts by inhibiting 50 S ribosomal subunit and inhibiting the binding of t. RNA � 2) As we all clear, protein synthesis is crucial for cell to replicate as it needs to double it’s cellular components in order to divide into 2 progeny cells. � 3) When protein synthesis is halted, cell doesn’t have enough protein to get ready for replication. Thus, it wont divide � 4) So, the bacteria remains dormant and eventually weakens and make it easy to be destroyed by immune cells.
 It acts by inhibiting the cross linking of nascent (NEW) peptidoglycan")
�Penicillin � 1) It acts by inhibiting the cross linking of nascent (NEW) peptidoglycan through binding to Penicillin Binding Protein (PBP). � 2) It must be clear that cross linking only happens when there is a NEWLY synthesized peptidogycan � 3) Peptidoglycan only be synthesized when the cell is starting to replicate.

�If you give Tetracycline, it will eventually stop bacterial replication. Without replication, there will be no synthesis of new peptidoglycans. �Without new peptidoglycans, there will be no cross linking. �Without cross linking, Penicillin couldn’t elicit its response.

Features of Antimicrobial Drugs: Adverse Effects 1. 2. 3. Allergic Reactions: some people develop hypersensitivities to antimicrobials Toxic Effects: some antimicrobials toxic at high concentrations or cause adverse effects Suppression of normal flora: when normal flora killed, other pathogens may be able to grow to high numbers

Features of Antimicrobial Drugs: Resistance to Antimicrobials �Some microorganisms inherently resistant to effects of a particular drug �Other previously sensitive microorganisms can develop resistance through spontaneous mutations or acquisition of new genes (more later).

So, The Criteria of the Ideal Antibiotic: �Selectively toxic to microbe but nontoxic to host. �Soluble in body- tissue distribution – BBB. �Remains in body long enough to be effective resists excretion and breakdown. �Shelf life. �Does not lead to resistance. �Cost not excessive. �Microbiocidal rather than microbiostatic. �Concerns suppression of normal flora - antibiotic associated colitis with Clostridium difficule and it’s toxins or Candida albicans.

Mechanisms of action of Antibacterial Drugs 1. 2. 3. 4. 5. Inhibit cell wall synthesis Inhibit protein synthesis Inhibit nucleic acid synthesis Injury to plasma membrane Inhibit synthesis of essential metabolites

Figure 20. 2

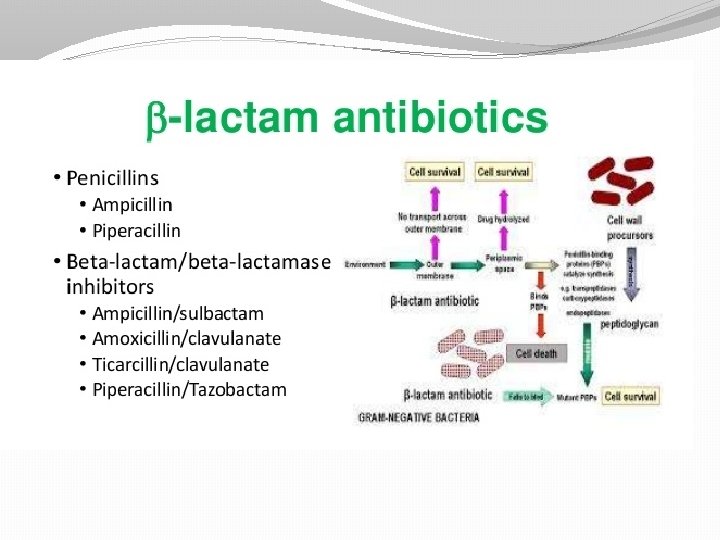
Inhibition of Cell Wall Synthesis: b-Lactam Drugs �Irreversibly inhibit enzymes involved in the final steps of cell wall synthesis
 are a broad class of antibiotics �Antibiotic agents")
β-lactam antibiotics �β-lactam antibiotics (beta-lactam antibiotics) are a broad class of antibiotics �Antibiotic agents that contain a β-lactam ring in their molecular structures. �This includes penicillin derivatives (Pens), cephalosporins (cephs), monobactams, and carbapenems.
 �Gram+ bacteria. �So, take phenoxymethylpenicillin. �Large Vd, but penetration into brain: poor,")
Penicillins (Benzylpenicillin) �Gram+ bacteria. �So, take phenoxymethylpenicillin. �Large Vd, but penetration into brain: poor, except when the meninges are inflammed. �Broad spectrum penicillins: amoxicillin and ampicillin are more hydrophillic and therefore, are active against gram- bacteria.

Broad-Spectrum Penicillins �Ampicillin and amoxicillin – very active against non-β-lactamase-producing gram+ bacteria. �Because they diffuse readily into Grambacteria, also very active against many strains of E. coli, H. influenzae, and Salmonella typhimurium. �Orally, amoxicillin is better because absorption is better.

b-Lactam Drugs �Some bacteria produce b-lactamaseenzyme that breaks the critical b-lactam ring �b-lactam drugs include: penicillins and cephalosporins

Cephalosporins �Used for treatment of meningitis, pneumonia, and septicemia. �Same mechanism and pharmacology as that of pens. �Similar to pens in broad-spectrum antibacterial activity.

 in case of antibacterial resist. Cefuroxime (prophylactic in surgery) – Resistant")
Cefelexin (for UTI) in case of antibacterial resist. Cefuroxime (prophylactic in surgery) – Resistant to inactivation by β-lactamases and used in severe infections (others ineffective). Ceftazidime – wide range of activity against gramincluding Pseudomonas aeruginosa), but is less active than cefuroxime against gram+ bact (Staph. aureus). Used in meningitis (CNS-accessible) caused by gram- bacteria.

Vancomycin �Not well absorbed orally. �Inhibits peptidoglycan formation. �Active against most gram+ organisms. �I. v. treatment for septicemia or endocarditis caused by MRSA. �Used for pseudomembranous colitis (superinfection of the bowel by Clostridium difficile – produces a toxin that damages the colon mucosa)

Antibacterial Drugs that Inhibit Cell Wall Synthesis

Antibacterial Medications that Inhibit Protein Synthesis �Target ribosomes of bacteria �Aminoglycosides: bind to 30 S subunit causing it to distort and malfunction; blocks initiation of translation �Tetracyclines: bind to 30 S subunit blocking attachment of t. RNA. �Macrolides: bind 50 S subunit and prevents protein synthesis from continuing.

Aminoglycosides �Against many gram- and some gram+. �Narrow TI – very potentially toxic. �Most important adverse side-effect: 8 th cranial nerve damage. (ototoxicity) and kidney damage. � (The vestibulocochlear nerve/auditory vestibular nerve, known as the eighth cranial nerve, transmits sound and equilibrium (balance) information from the inner ear to the brain. )

Aminoglycosides �Gentamicin – used for acute, lifethreatening gram- infections. Has synergism with pens and vanco. �Amikacin – used for bacteria that are genetically resistant. �Netilmicin – less toxic than gentamicin. �Neomycin – too toxic for parenteral use. Used for topically for skin infections and orally for sterilizing bowel before surgery.

�Streptomycin – active against Mycobacterium tuberculosis. But because of its ototoxicity, rifampicin replaces. �Rifampicin – resistance develops quickly alone; so, with TB, combine with isoniazid, ethambutol, and pyrazinamide for the 1 st 2 months of treatment, followed by another 4 months with rifampicin and isoniazid.

Macrolides �Usually given orally. �Erythromycin and clarythromycin �Effective against gram- bacteria and can be used as an alternative to penicillin-sensitive patients, especially in infections caused by streptococci, staphylococci, pneumococci, and clostridia. �Don’t cross the BBB – ineffective against meningitis.

�Erythromycin – in high doses, may cause nausea and vomiting (less so with clarithromycin and azithromycin). �Azithromycin – very long t 1/2 (~40 -60 hr) and a single dose is as effective in treating chlamydial non-specific urethritis as tetracycline admin over 7 days,

Tetracyclines �Broad-spectrum. �Penetrate micro-organisms well. �Sensitive organisms accumulate it through, partly passive diffusion and partly through active transport. �Tetracyclines bind to Ca in growing bones and teeth can discolor teeth. So, should be avoided in children < 8 yrs old. �Tetracycline, doxicycline, minocycline

Chloramphenicol �Broad-spectrum. �Serious side-effects: bone marrow aplasia, suppression of RBCs, WBCs, encephalopathy, optic neuritis. �So, periodic blood counts required, especially in high doses.

�Large Vd, including CNS. �Inhibits the actions of other drugs and may increase the actions of phenytoin, sulphonylureas, and warfarin. �Neonates cannot met the drug rapidly accumilation ‘grey baby’ syndrome (pallor, abdominal distension, vomiting, and collapse).

Antibacterial Drugs that Inhibit Protein Synthesis

Sulphonamides �Sulfadiazine well-absorbed orally. Used to treat UTIs. �But many strains of E. coli are resistant. �Adverse effects: allergies, skin rashes, fever. �Trimethoprin – used for UTIs and RTIs �Co-trimoxazole (trimethoprin + sulfamethoxazole) – used mostly for pneumonia, and toxoplasmosis.
 � Inhibit folic acid synthesis � Broad")
Antibacterials – Competitive Inhibitors �Sulfonamides (Sulfa drugs) � Inhibit folic acid synthesis � Broad spectrum Figure 5. 7

Quinolones �Inhibit DNA gyrase. �Nalidixic acid – used only for UTIs. �Ciprofloxin (6 -fluoro substituent) that greatly enhances its effectiveness against both gram- and gram+ bacteria. Well-absorbed both orally and i. v. Eliminated largely unchanged by the kidneys. Side-effects (headache, vomiting, nausea) are rare; but convulsions may occur.

5 -Nitroimidazoles �Wide-spectrum �Metronidazole – against anaerobic bacteria and protozoan infections. �Tinidazole – longer duration of action. �Diffuses into the organism where the nitro group is reduced chemically reactive intermediates are formed that inhibit DNA synthesis and/or damage DNA.

Antibacterial Drugs that Inhibit Nucleic Acids

Antibacterial medications that damage Plasma Membrane �Polymyxin B: binds to membrane of Gram- bacteria and alters permeability �This leads to leakage of cellular contents and cell death �These drugs also bind to eukaryotic cells to some extent, which limits their use to topical applications

Antibacterial Drugs that Inhibit Synthesis of Essential Metabolites �Competitive inhibition by substance that resembles normal substrate of enzyme �Sulfa drugs

Antiviral Drugs �Effective against a very limited group of diseases �Targets for antiviral drugs are various points of viral reproduction

Drugs that Prevent the Virus from Entering or Leaving the Host Cells �Amantadine – interferes with replication of influenza A �Zanamivir – inhibits both influenza A and B �Immunoglobulins – Human Ig contains specific Antibodies against superficial Antigens of viruses can interfere with their entry into host cells. Protection against hep. A, measles, and rubellla (German measles).

Drugs that Inhibit Nucleic Acid Synthesis Nucleoside and Nucleotide Analogs �Acyclovir- used to treat genital herpes �Cidofovir- used for treatment of cytomegaloviral infections of the eye �Lamivudine- used to treat Hepatitis B

Acyclovir �HSV and VZV �Viral enzymes have a much higher affinity than the host enzymes for the drug. �Effective against HSV, but does not eradicate them. �Need high doses to treat shingles.
 –so, given only for severe CMV infections in immunosuppressed patients.")
Ganciclovir �Quite toxic (neutropenia) –so, given only for severe CMV infections in immunosuppressed patients. �CMV is resistant to acyclovir

Antiretrovirals �Currently implies a drug used to treat HIV �Tenofovir- nucleotide reverse transcriptase inhibitor �Zidovudine- only used orally for AIDS. -Severe adverse effects: anemia, neutropenia, myalgia, nausea, and headaches. �Stavudine, didanosine, zalcitabine – �Nevirapine, efavirenz –

Interferons �Cells infected by a virus often produce interferon, which inhibits further spread of the infection �Alpha-interferon - drug for treatment of viral hepatitis infections

Resistance to Antimicrobial Drugs �Drug resistance limits use of ALL known antimicrobials �Penicillin G: first introduced, only 3% of bacteria resistant �Now, over 90% are resistant

Slowing the Emergence and Spread of Antimicrobial Resistance 1. Responsibilities of Physicians: must work to identify microbe and prescribe suitable antimicrobials, must educate patients 2. Responsibilities of Patients: need to carefully follow instructions

Slowing the emergence and spread of antimicrobial resistance 3. Educate Public: must understand appropriateness and limitations of antibiotics; antibiotics not effective against viruses 4. Global Impacts: organism that is resistant can quickly travel to another country - in some countries antibiotics available on nonprescription basis

Fungal Infection in Humans = Mycosis �Major Types of Mycoses �superficial �cutaneous �subcutaneous �systemic �opportunistic �Symptoms vary from cosmetic to life threatening

Antifungal Agents �Polyene antibiotic �The polyene antibiotics bind with sterols in the fungal cell membrane, . �Nystatin �Amphotericin B �Natamycin �Rimocidin �Filipin �Pimaricin

Antifungal Agents �Imidazole and triazole �The imidazole and triazole groups of antifungal drugs inhibit the enzyme that is required in fungal cell membrane synthesis. These drugs also block steroid synthesis in humans.

�Imidazoles: � Miconazole � Ketoconazole � Clotrimazole � Mebendazole � Isoconazole � Sertaconazole � Thiabendazole Bifonazole Butoconazole Econazole Fenticonazole Oxiconazole Sulconazole Tiaconazole

Antifungal Agents �The triazoles are newer, and are less toxic and more effective: �Fluconazole �Itraconazole

Questions ?

THANK YOU
- Slides: 66