Antimicrobial agents Pharm Dr Ondej Zendulka Ph D

Antimicrobial agents Pharm. Dr. Ondřej Zendulka, Ph. D.

Antimicrobial agents • difference antibiotics-chemotherapeutics • classification: chem. structure mechanism of action extent of effect antibacterial spectrum

Antimicrobial agents Mechanisms of action: selective toxicity • interference with the cell wall • block of bact. cell metabolism • nucleic acid synthesis inhibition • proteosynthesis inhibition

Antimicrobial agents Bacterial cell wall

Antimicrobial agents Bacterial cell wall

Antimicrobial agents Bacterial cell wall

Terminology • selective toxicity • antimicrobial spectrum • MIC, MBC, MAC • postantibiotic effect • resistance

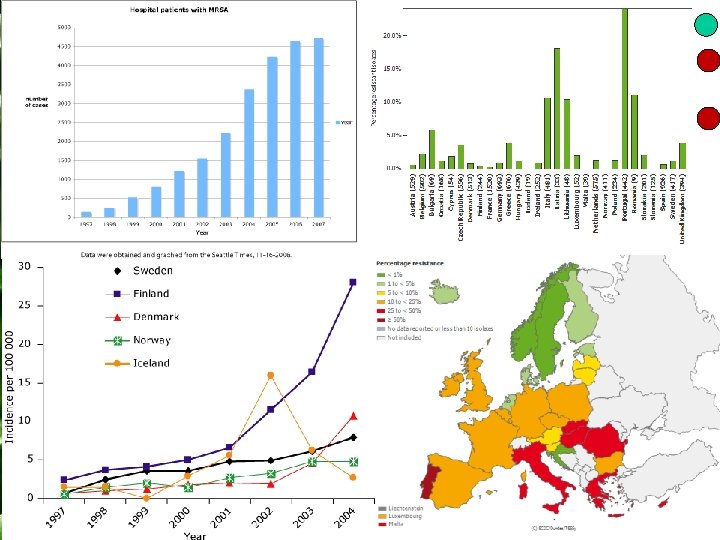
Antimicrobial agents Resistance = ability of microbial cells to withstand the effect of ATB Mechanisms of resistance: • decrease of ATB‘s intracelullar conc. • inactivation of ATB • modification of ATB‘s target site

Antimicrobial agents • absolute • relative • primary • secondary • coupled • cross

Antimicrobial agents Combinations of ATBs: • spectrum widening • resistance development restriction • decrease in AE incidence • increase in effectivity • effects: synergistic, additive, indifferent, antagonistic

Antimicrobial agents Which ATB? • empirical x bacterial sensitivity • pharmacokinetics • Antibiotic policy in CR • prophylactic administration of ATBs

Antimicrobial agents Antibiotics • β-lactams • amphenicols • tetracyclines • macrolides • azalides • streptogramines • ketolides • oxazolidinones • lincosamides • aminoglycosides • glycopeptides • miscellaneous ATBs • local ATBs • sulphonamides • quinolones • imidazoles

• β-lactams penicillins cephalosporins cephamycins monobactams carbapenems + inhibitors of β-lactamases

Penicillins Mof. A: binding to PBP, inhibition of transpeptidases, autolysis => bactericidal

Penicillins • produced by Penicillium mould • resistance : β-lactamases modification of PBP cell wall penetration block • low toxicity, AE hypersensitivity
 • for parenteral use only • destroyed by")
Narrow spectrum penicillines Benzylpenicillin (Penicillin G) • for parenteral use only • destroyed by β-lactamases • spectrum: Streptococc. , Meningococc. and gonococc. • crystalic, procain or benzathin salt
 • for peroral administration Penamecillin • ester of")
Narrow spectrum penicillines Fenoxymethylpenicillin (Penicillin V) • for peroral administration Penamecillin • ester of penicilline G • for peroral use

Narrow spectrum penicillines Penicillines stable against lactamases • efective only against Staphylococc. and Streptococc. • oxacillin, cloxacillin, flucloxacillin, dicloxacillin • 4 -6 h 0, 5 -1 g p. o. or parent.

Wide spectrum penicillines Aminopenicillins • wider spectrum - Haemophilus influenzae • lower efficacy against β-hemolytic streptoc. • combination with inhibitors of lactamases • ampicillin (becampicillin, pivampicillin), amoxycillin

Wide spectrum penicillines Carboxypenicillins • effective against Pseudomonas aeruginosa • nonstable in stomach • combination with lactamases inhibitors • ticarcillin, carbenicillin

Wide spectrum penicillines Ureidopenicillins • widest spectrum, pseudomonades, klebsiellas • not stable in acid environment • combined with lactamases inhibitors • piperacillin, azlocillin, mezlocillin

Inhibitors of β-lactamases • usually without own antimicrobial properties • clavulanic acid, sulbactam, tazobactam • coamoxicillin (clavulanic ac. ) • cotikarcillin (clavulanic ac. ) • coampicillin (sulbactam) • sultamicillin (sulbactam) • copiperacillin (tazobactam)

Cephalosporins Mof. A: the same as in penicillins • produced by Cephalosporinum

Cephalosporins Spectrum: • differs between generations • NOT EFFECTIVE: Campylobacter jejuni Legionella pneumophilla Clostridium difficile Enterococcus fecalis mycoplasmas, mycobacterias, chlamydias
 • from")
Cephalosporins I. generation • high efficacy against G+ (streptoc. , staphyloc. ) • from G- against E. coli, K. pneumoniae, H. influenza • partially stable against lactamases • crossed resistance with penicillines • cefazolin, cefalotin, cefapirin – parenteral • cefalexin, cefadroxil - peroral
, enteroc. •")
Cephalosporins II. generation • high efficacy against G+ (streptoc. , staphyloc. ), enteroc. • from G- like I. gen, Shigella, Enterobacter • mainly against respeiratory infections • cefuroxim, cefamandol – parenteral • cefuroxim-axetil, cefaclor, cefprosil, cefpodoxim-proxetil - peroral

Cephalosporins III. generation • high efficacy against G+ but lower on staphyloc. • G- sensitive including Pseudomonas • more resistant to lactamases than I. And II. gen. • cefotaxim, ceftriaxon, cefmenoxim, ceftazidim, cefoperazon, cocefoperazon, cefsulodin – parenteral • cefixim, ceftibuten, cefetamet-pivoxil - peroral

Cephalosporins IV. generation • wide spectrum, high efficacy • serious infections • cefpirom, cefepim Cephamycins • good results against anaerobes • cefoxitin

Monobactams • bactericidal G- aerobes • β-lactamases resistant • aztreonam, carumonam Carbapenems • wide spectrum • imipenem, meropenem

Amphenicols Mof A. : proteosynthesis inhibition – 50 S subunit Spectrum: majority of G + i G -, anaerobes, ricketsias, chlamydias, mycoplasmas • per os or parenterally • interferention with metabolism of other drugs • reversible or irreversible myelosuppresion, contraindicated in newborns • chloramphenicol, thiamphenicol

Tetracyclines Mof. A: proteosynthesis inhibition- 30 S subunit Spectrum: most of G + i G -, chlamydias, mycoplasmas • parenterally or per os • crossed resistance • deposition into bones and cartilages = discoloration, contraindicated in pregnant women and childrens (to 8 yrs) • doxycycline, minocycline

Macrolides Mof. A: proteosynthesis inhibition, 50 S subunit Spectrum: majority of G + i G -, chlamydias, mycoplasmas • bacteriostatic eff. • alternative for penicillines • crossed resistance • GIT intoleration, metabolism via CYP 450 3 A • erythromycin, spiramycin, josamycin, roxithromycin, clarithromycin, dirithromycin

Azalides Mof. A: like macrolides Spectrum: like erytromycin • bacteriostatic eff. • resistance crossed with erythromycin • GIT intolerance, metabolization via CYP 450 A 3 • azithromycin

ATBs related to macrolides Streptogramins • quinupristin, dalfopristin • parenterally, multiresistant G+ cocci Ketolides • telithromycin • does not inhibit CYP 450 Oxazolidinones • linezolid • against resistant strains

Lincosamides Mof. A. : proteosynthesis inhibition – 50 S subunit Spectrum: G+ cocc. and bacill. , G- cocc. • AE: GIT, pseudomembraneous colitis • clindamycin, lincomycin

Aminoglycosides Mof. A: proteosynthesis inhibition, binding to different ribosomal sites Spectrum: G - , staphylococcus, brucellias • slow developing resistance • only parenterally • postantibiotic effect • nephro-, oto-, neurotoxicity • streptomycin, sisomicin, tobramycin, netilmicin, amikacin, isepamicin

Glycopeptides Mof A: inhibition of cell wall synthesis Spectrum: only G + • slow developing resistance • not absorbed from GIT • nephro-, ototoxicity, release of histamine • vancomycin, teicoplanin

Miscellaneous ATBs Fusidic acid Mof. A: inhibition of cell waal proteins synthesis Spectrum: penicillin resistant staphyloc. • fast resistance => combinations Rifampicin Mof. A. : inhibition of bacterial DNA-dependent RNA-polymerases Spectrum: Staphylococc. , Haemophilus, neisserias, mycoplasmas • colours urine and salivas, induces CYP 450

Miscellaneous ATBs Rifaximin • rifampicin derivative Phosphomycin Mof. A. : inhibition of peptidoglycane synthesis Spectrum: Staphylococc. and Enterococc. • synergistic with cephalosporines and aminoglycosides
 • polypeptides • high system toxicity =>")
Miscellaneous ATBs Polymyxin B, colistin (polymixin E) • polypeptides • high system toxicity => locally • nephrotoxicity, neurotoxicity Spectinomycin Mof. A. : proteosynthesis inhibition Spectrum: Neiseria gonorrhoae • therapy of gonorrhea
 Bacitracin")
ATBs for local use Neomycin • aminoglycoside • in combination with bacitracin (Framykoin) Bacitracin • polypeptide • low resistance and allergy Mupirocin • inhibition of proteosynthesis • skin infections therapy

Chemotherapeutics • Sulphonamides • Trimethoprim • Quinolones • Metronidazole • Nitrofurantoin

Sulphonamides • one of the oldest • basic structure – sulfanilamide • small therapeutic importance • Mof. A: competitive inhibition of bacterial cell metabolism on the level of folic acid • bacteriostatic effect • spectrum: streptococcus, haemophillus, nocardia, actinomycets, chlamydia, Toxoplasma gondi, Neisseria meningitidis • today – therapy of urinary tract infections and in the combination with trimethoprim

Sulphonamides • strong binding to plasmatic proteins = drug interactions • AE: skin – phototoxicity, Stevens-John‘s syndrome; myelotoxicity; haemolytic anaemia; allergic reaction; crystalluria

Sulphonamides Sulfisoxazole • short acting, fast absorption and elimination • protein binding up to 92% • urinary infections Sulfathiazole • for topicall administration Sulfamethoxazole • in combination with trimethoprim - cotrimoxazole • protein binding 70% Sulfasalazine • poor absorption from GIT = local effect in the intestine, ulcerative colitis
 •")
Trimethoprim • blocks dihydrofolate reductase (50 000 x more selective to bacterial enzyme) • synergistic effect with sulphonamides • high levels in prostate and vaginal mucus (lower p. H) • CYP metabolism • urine (low p. H = faster elimination) • combination: trimethoprim a sulfamethoxazole = co-trimoxazole 1: 5: Triprim, Biseptol Kotrimoxazol, Sumetrolin • I: respiratory infections, prevention and therapy of pneumonia, urinary infections

Quinolones • Mof. A: inhibition of DNA gyrase - nucleic acid synthesis inhibition (topoisomerase II) • bactericidal • spectrum: older molecules mainly G-; modern drugs wide spectrum

Quinolones • high F after p. o. administration, good distribution except CNS, excreted into urine • AE: 2 -8% nemocných GIT problems, – cephalgia, sleeping disorders – skin symptoms – risk of tendons rupture • I: urinary tract infections – prostatitits – bone and joint infections – skin infections – prophylaxis in neutropenic patients • CI: children, breastfeeding, pregnancy

Quinolones for therapy of urinary infections • poor tissue distribution, excreted unchanged • oxoline and nalidixic acid • norfloxacine – partial systemic effect, therapy of gonorrhea • high rate of mild adverse effects (GIT)

Quinolones • Quinolones for therapy of systemic infections. Fluoroquinolones • ciprofloxacin, lomefloxacin, pefloxacin…. • good tissue distribution • therapy of respiratory, skin, GIT and other severe infections • sparfloxacin, trovafloxacin, rufloxacin, grepafloxacin • bile elimination • life-threatening infections caused by multiresistant strains • AE: often, mild, GIT, artralgia, cartilage disruption

Imidazoles Mof. A: inhibition of DNA replication • spectrum: anaerobes and protozoa : Bacteroides, Clostrididum, Giardia Metronidazole • metabolized in liver and excreted into urine • AE: metallic taste – nausea, vommiting, diarrhoea – CNS (cephalgia, sleping disorders, depression) – disulfiram reaction • Ornidazole • Tinidazole – antiparasitic agent

Others Nitrofurantoin Mof. A: interferes with bacterial DNA • spectrum: E. coli, Klebsiella, Enterobacter, enterococci, staphylococci • administered orally • effective levels in urine, alkaline p. H decreases the efficacy AE: often – GIT irritation, polyneuropathy, myelotoxicity, chronic hepatitis, pulmonary disorders I: therapy and prophylaxy of urinary tract infections Furantoin, Nitrofurantoin
- Slides: 53