Antihypertensive Drugs Assoc Prof Ivan Lambev www medpharmsofia
")
Antihypertensive Drugs Assoc. Prof. Ivan Lambev (www. medpharm-sofia. eu)

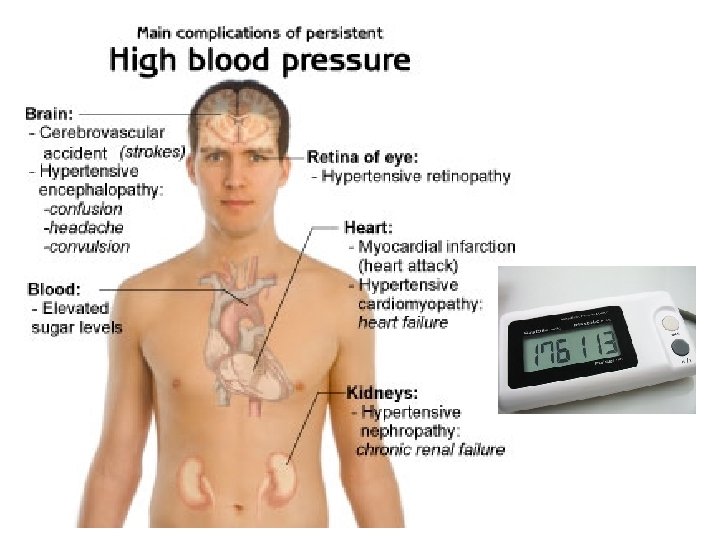
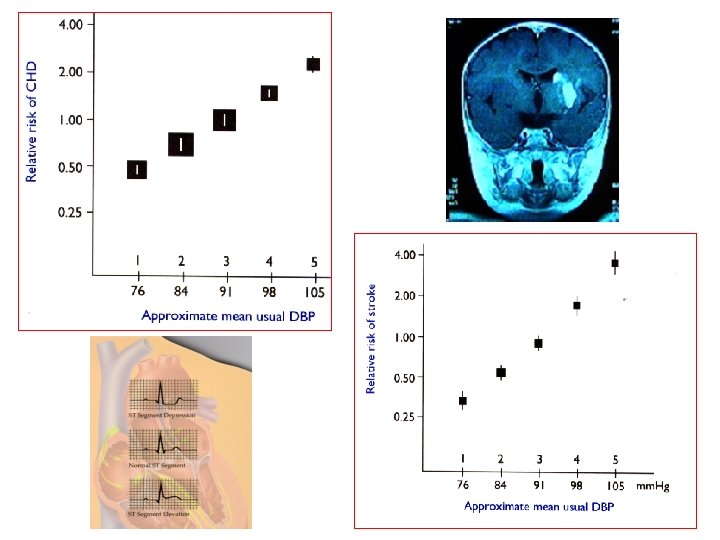
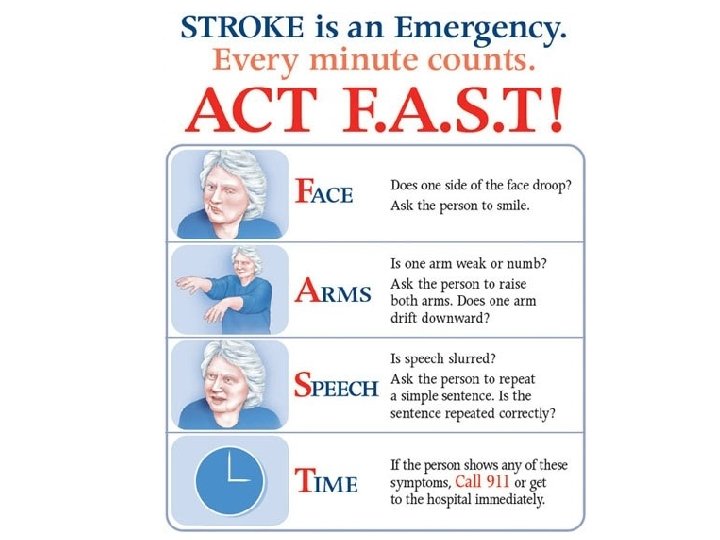
HYPERTENSION is the strongest modifiable risk factor for coronary heart disease. It is also responsible for considerable (potentially preventable) disability from stroke, heart and renal failure. Despite this, usually, hypertension continues to be underdiagnosed and undertreated. Many clinical investigations show the relationship between mean blood pressure (BP) and the risk of coronary heart disease (CHD) and stroke (insultus cerebri).

Most patients with persistent arterial disease have ESSENTIAL HYPERTENSION. But hypertension is occasionally secondary to some distinct disease: • Coarctation of aorta • Renal artery stenosis • Parenchymal or obstructive renal disease • Cushing’s syndrome

Essential hypertension 90% l a n e R r e h Ot 5% s 5% 5%
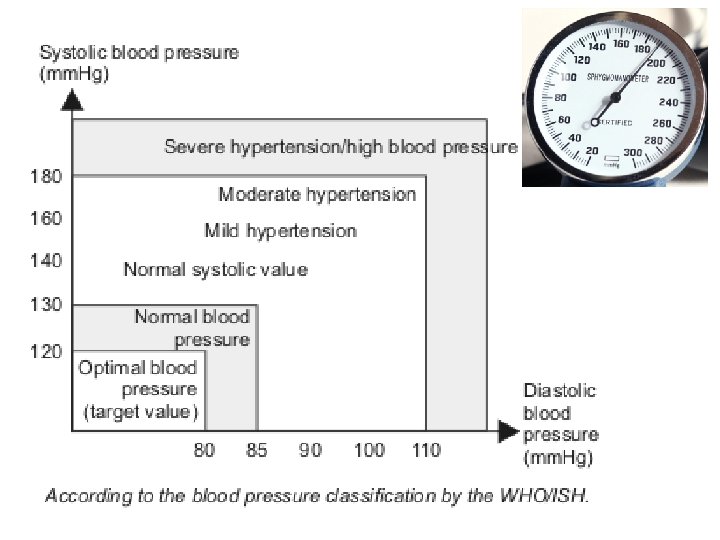

There is changes in perceived norms recently target values for blood pres Norm now taken 135/85 mm Hg. For patients over 60 years old today accepted by cardiologists targeted values for blood pressure are 140/90 mm Hg, and in people over 80 years old they are 150/90 mm Hg.

Cushing’s syndrome is a side effect of glucocorticosteroids (hydrocortisone, betamethasone, etc. The main symptom i arterial hypertension

ARTERIAL BLOOD PRESSUR is determined by cardiac output and peripheral vascular resistance. The kidney plays a key role in its contro • Excretion of salt and water controls intravascular volume, which influen the forces of contraction of the hea • Excretion of renin influences vascu tone and electrolyte balance.

Arterial blood pressure >>> 120/80 mm Hg at rest • Increased: peripheral vessel resistance, cardiac output, tone of sympathetic nervo system, synthesis of AII, aldosterone, ETs • Inhibited synthesis of NO, kinins, PGE, P

Hypertension of white apro

SHRSP

Drugs acting on the RA
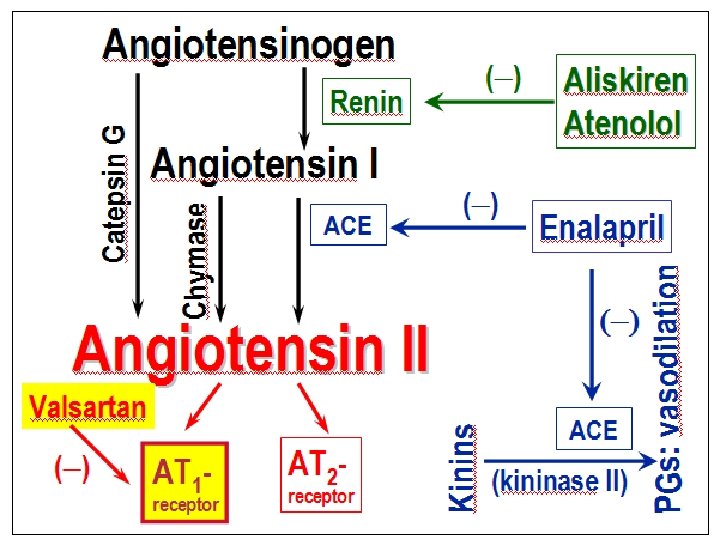
 ACE inhibitor • Competitive inhibition of ACE reduces generation of AT II and")
a) ACE inhibitor • Competitive inhibition of ACE reduces generation of AT II and release of aldosterone. Inhibition of tissue ACE in the vasscular wall is more important for the hypotensive effect of these drugs than its action on the circulating renin-angiotensin system. • Reduced tissue concentrations of AT lead to arterial and venous dilation.
 Kallikrein Bradykinin Degradation products")
Kininogen Angiotensinogen Renin Angiotensin II Aldosterone release ACE (kininase II) Kallikrein Bradykinin Degradation products

Angiotensin II and ACE inhibitors • Captopril • Cilazapril • Enalapril • Fosinopril • Lisinopril • Perindopril • Ramipril • Trandolapril
")
CAPTOPRIL (prodrug)

ACE inhibitors – used in: AH, CHD, atherosclerosis, DM, sclerodremal crisis Unwanted effects: • Cough: unproductive; may be due to accumulation of kinins in the lung; occurs up to 10– 20 % of patients (more common in women!). • Postural hypotension (sometimes after the first dose) • Disturbances of taste, K+ • Rashes, angioneurotic edema • Teratogenicity (PRC: D)
 AT 1 -blockers (sartan Losartan Irbesartan Valsartan Oral: in a once daily dosing")
b) AT 1 -blockers (sartan Losartan Irbesartan Valsartan Oral: in a once daily dosing regimen Expensive, but with small ARs.
: • They")
AT 1 -antagonists differ from ACE inhibitor following ways (by Tripathy, 2003): • They do not interfere with degradation of kin (so no rise in level or potentiation of bradyk • They block completely AT 1 -receptors and th alternative pathways of AT generation do no any importance. • They result in indirect AT 2 -receptor activatio ACE inhibitors result in depression of both A and AT 2 -activation.
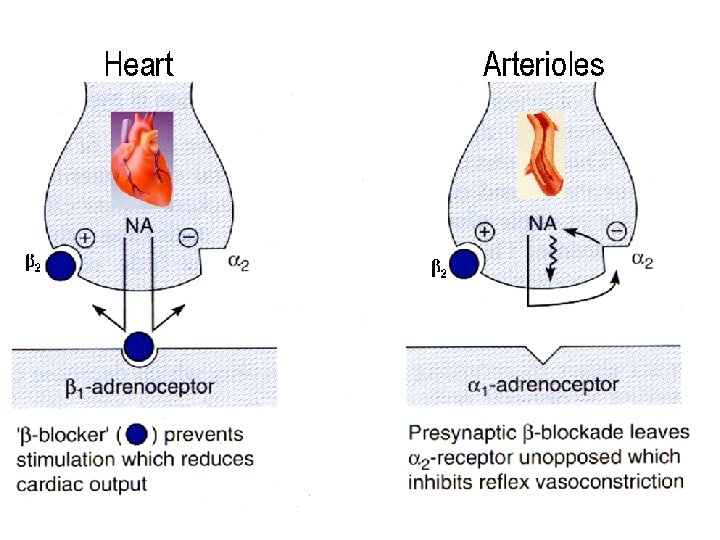
 Beta-blockers (β 1) (β 1 & β")
Drugs acting on the S a) Beta-blockers (β 1) (β 1 & β 2 ) (β & α ) Atenolol Bopindolol Carvedilol Acebutolol (β 1 ISA) (antioxidant) Propranolol Bisoprolol Oxprenolol (β 1 ISA) Labetalol Celiprolol (β 2 ISA) Pindolol (with β 1 ISA) Metoprolol Nebivolol releases NO

Mechanism of antihypertensive effect • Blockade of β 1 -adrenoceptors in heart reduces heart rate and myocardial contractility. • Blockade of renal juxtaglomerular β 1 receptors reduces renin secretion. • Blockade of presynaptc β 2 -adrenoceptors inhibits exocytose of NA. • Carvedilol and labetalol also block a-receptors and produce vasodilation.
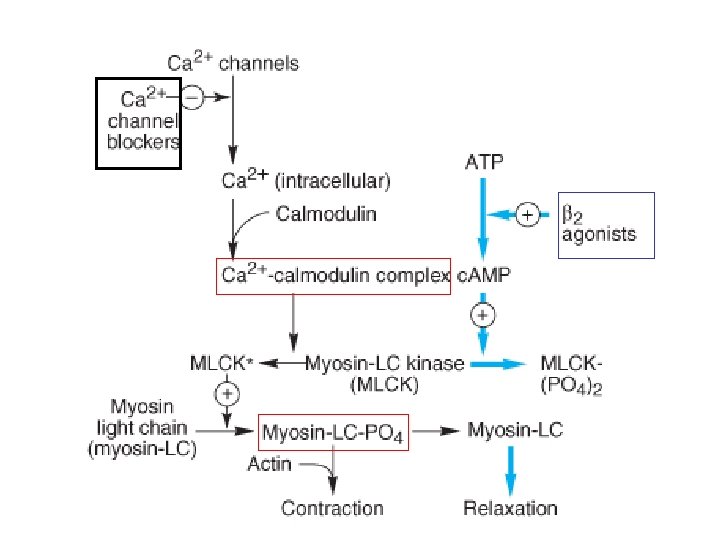
 AP Ca 2+ (–) Cell wall Receptor ROCC VDCC Ca 2+ Sarcoplasmatic")
Beta-blockers (–) AP Ca 2+ (–) Cell wall Receptor ROCC VDCC Ca 2+ Sarcoplasmatic reticulum AP – action potential, NA – noradrenalin VDCC – voltage dependent calcium chan ROCC – receptor operating calcium chan
 are well absorbed from the gut, but undergo extensive")
Lipophilic β-blockers (e. g. propranolol) are well absorbed from the gut, but undergo extensive first-pass metabolism in the liver, with considerable variability. Hydrophilic β-blockers (e. g. atenolol) ar less completely absorbed from the gut are eliminated unchanged by the kidney The dose range to maintain effective pla concentrations is narrower than that of which undergo metabolism and the clin response is more predictable.

Adverse reactions of β-blockers • Blockade of β 1 -receptors may cause bradycardia, AV block, heart failure. • Blockade of β 2 -receptors may cause bronchospasm, intermittent claudication (reducing peripheral blood flow) and hypoglycemia. Beta-blockers (-) ATP AC PDE c. AMP 3’, 5’ AM

• CNS effects: sleep disturbance, dreams and hallucinations (more common with lipophilic drugs which cross the BBB). • Most β-blockers raise plasma concentratio of triglycerides and lower concentration of antiatherogenic HDL (probably β 3 -effect ? • Induratio penis plastica (fibrosis …) • Sudden withdrawal syndrome: beta-blockers should be stopped graduall Nebivolol Selective β 1 -blocker, releases NO (causes vasod It has 24 h effect. End Effect/Maximum Effect >90

Selectivity β-blockers Atenolol Bisoprolol Metoprolol Nebivolol Propranolol β 1/β 2 -blocking activity 15 50 (55 -65/min 24 h) 25 293 (55 -65/min 24 h) 1, 9
 Postsynaptic α 1 -blockers Blockade of postsynaptic α 1 -receptors lowers blood pressure")
b) Postsynaptic α 1 -blockers Blockade of postsynaptic α 1 -receptors lowers blood pressure by: • Lowering tone in arteriolar resistance vessels. • Dilating venous capacitance vessels, which reduces venous return and cardiac output. • Selective α 1 -adrenoceptor antagonists spare the presynaptic α 2 -adrenoceptors and do not produce reflex tachycardia.

Postsynaptic α 1 -blockers Doxazosin Prazosin

Prazosin • It has potentially beneficial effect: - an increase in HDL; - a reduction in triglycerides • Adverse reactions (AR): - postural hypotension due to venous pooling (this can be troublesome after the first dose) - lethargy, tolerans

Doxazosin Indications: arterial hypertension and hyperplasia of the prostate gland (men > 45 yea Selective postsynaptic alpha-1 А-blocker: It blocks alpha-1 А-receptors into the smooth musc prostate gland, and the prostatic part of the urethra.
 α 2 a-agonists There are several different α 2 -adrenoceptor subtypes have been")
c) α 2 a-agonists There are several different α 2 -adrenoceptor subtypes have been identified: α 2 a, α 2 b and α 2 a-adrenoceptors appear to mediate sed analgesia and hypotension while the α 2 b-adrenoceptor mediates vasoconstric and hypertension (i. e. postsynaptic α 2 -adrenoceptors are probably of the α 2 b su

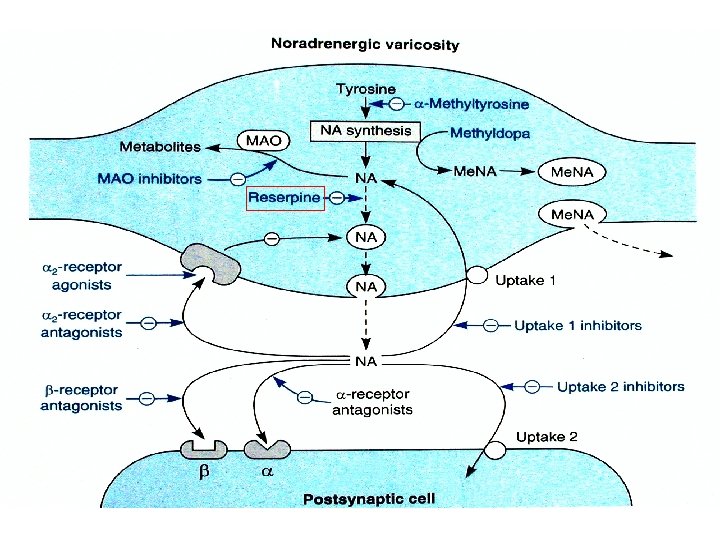
The stimulation of presynaptic α 2 a-receptors in CNS inhibits NA release, reduces sympathetic influence on the vasomotor centre; reduces peripheral arterial and venous tone. • Clonidine ( HCl) - xerostomia (dry mouth) - withdrawal phenomenon - sedation - postural hypotension • Methyldopa (prodrug: α-methyl-NA is an α 2 a-agonist)
 (+) a Clonidine α-methyl-NA")
Dopegyt® (α-methyl-DOPA) (+) a Clonidine α-methyl-NA
 I 1 (Imidazoline-1)-agonists (> t 1/2: 1 time daily p. o. ) The")
) I 1 (Imidazoline-1)-agonists (> t 1/2: 1 time daily p. o. ) The stimulation of I 1 -receptors: • in CNS reduces sympathetic tone and lowers blood pressure; • in kidney inreases secretion of ANP • Moxonidine • Rilmenidine
 Rauwolfia serpentina")
• Guanethidine • Reserpine – Numerous adverse reactions (out of date) Rauwolfia serpentina e) Adrenergic neuron blockers

Adrenergic neuron blockers use the active transport mechanisms for monoamines to accumulate in the adrenergic ne terminal. Inside the cell they pre the release of NA from vesicles.

Calcium antagonists
 Cell wall NA Receptor ROCC VDCC Ca 2+")
Calcium antagonists AP Ca 2+ (–) Cell wall NA Receptor ROCC VDCC Ca 2+ Sarcoplasmatic reticulum AP – action potential, NA – noradrenali VDCC – voltage-dependent calcium cha ROCC – receptor operating calcium cha

Calcium antagonist Amlodipine norm frequent dihydropyridine t 1/2 31– 47 h, 55– 91% p. o. bioavailabil 5– 10 mg/24 h p. o. (once daily) Nifedipine (tachycardia!) – effective in vasospastic angina Diltiazem (in SR dosage forms) Verapamil (Isoptin SR® – tabl. 24 (22% p. o. bioаvailability, first pass eff extensive liver metabolism; constipati
")
Adverse reactions • Arterial dilation: headache, flushing and dizziness, ankle edema (resistant to diuretics) • Bradycardia and AV block (verapamil and diltiazem), constipation (verapamil) • Verapamil has potentially hazardous additive effects with beta-blockers, reducing the force of myocardial contraction and slowing the heart rate. • Tachycardia (nifedipine, nisoldipine).

Gingivitis haemorrhagica

Diuretics (p. o. in low daily dos Hydrochlorothiazide Chlorthalidone Indapamide 5% Indapamide • Vasodilator • It does not influence serum level of Na+, K+, Mg 2+ and Ca 2+ Amiloride Triamterene Spironolactone 3% 20 -30% Furosemide Torsemide

In small doses thiazide and loop diuretics reduce the intracellular sodium in the smooth muscle of the resistance vessels, which decreases responsiveness to vasopressor substances. ARs of thiazide and thiazide-like diuretics • Hypokalemia, salt and water depletion, hyperuricemia, nocturia, glucose intolerance (dose-related) and hyperglycemia, hyperlipidemia (increased LDL and triglycerides), impotence.
 • Sodium nitroprusside (direct NO donor):")
Other antihypertensive vasodilators (used in hypertensive emergencies) • Sodium nitroprusside (direct NO donor): i. v. infusion • Diazoxide: bolus i. v. (ADRs: hyperglycemia) • Nifedipine: sublingually • Clonidine: sublingually, i. m. • Nitrolingual® or Isoket® spray: sublingually

Nitroprusside is an inorganic nitro- vasodilator with a mechanism of action similar to that of organic nitrates. It is reserved for hypertensive emergenc It dilates arterioles and veins, reducing both peripheral resistance and venous return. It is given by i. v. infusion and has a duration of effect of less than 5 mi Metabolism to cyanide within red blood cells terminates its effects. ADRs: Confu psychosis, metabolic acidosis.

Rational antihypertensive combina • ACE inhibitor + thiazide diuretic • Sartan + thiazide diuretic • Beta-blocker + thiazide diuretic • Beta -blocker + amlodipine or felodipin

Clinical classification A: ACE inhibitors and AT 1 -blockers B: Beta-blockers C: Calcium antagonists D: Diuretics

ADJUVANT DRUGS • Platelet antiaggregants • Antidyslipidemic drugs • Anxiolytics, etc. NONPHARMACOLOGICAL METHODS – avoiding of the risk factors

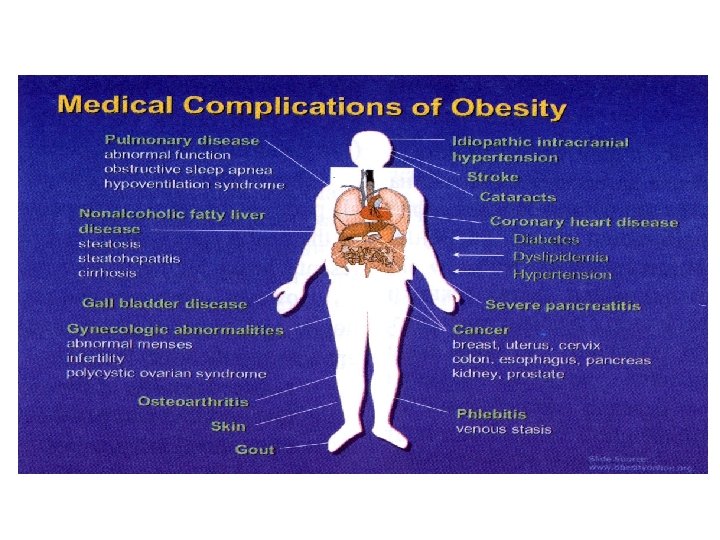
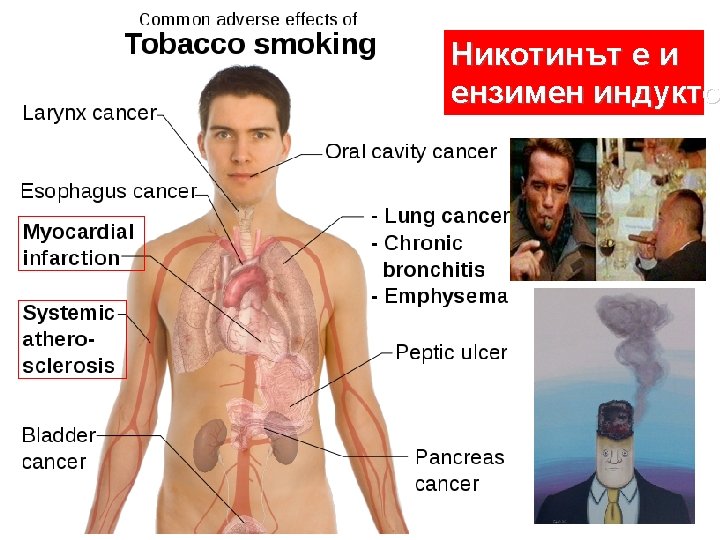
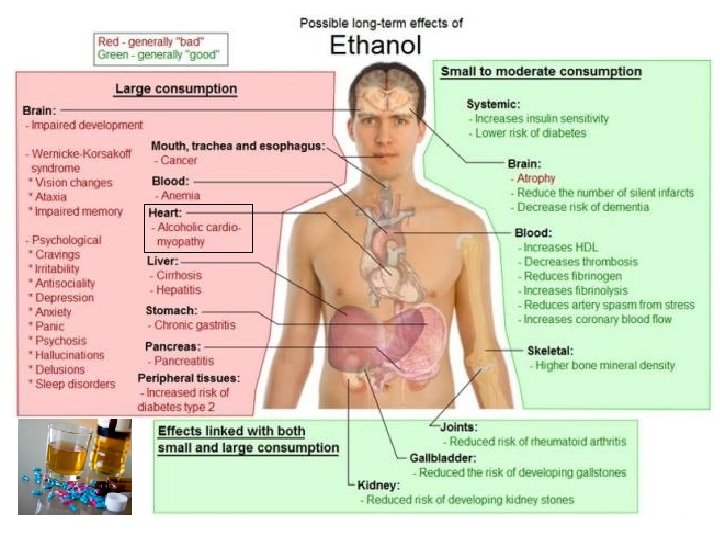
• Smoking 2/3 of • Lipid statusthe risk Risk factors for CV Chomocysteine > 15 mmol/l • Diabetes mellitus • Metabolic syndrome • Sedentary life style • Tachycardia • BMI > 30: >>> saturated fatty acids >>> salt and >>> sugar >>> alcohol <<< fruits and vegetables • Stress

Rating of cardiovascula r risk
- Slides: 62