ANTIHYPERTENSIVE DRUG UPDATE Jessica Schwenk Pharm D September

ANTIHYPERTENSIVE DRUG UPDATE Jessica Schwenk, Pharm. D. September 14, 2013

Objectives � Review pharmacologic treatment of hypertension, including drug combinations and management of hypertension with other disease states � Discuss updates in the use of antihypertensive drugs � Describe medications used for hypertensive urgencies and emergencies

Review of Hypertension

Review of Hypertension � How many people in the US have hypertension?

Review of Hypertension � How many people in the US have hypertension? � 58 to 65 million adults (estimated in 2008) � 29 -31% of US adults � Treatment of hypertension �#1 reason for doctor visits (non-pregnant adults) �#1 reason for use of prescription drugs

Review of Hypertension � Definitions �Normal blood pressure: systolic <120 mm. Hg and diastolic <80 mm. Hg �Prehypertension: systolic 120 -139 mm. Hg or diastolic 80 -89 mm. Hg �Hypertension: �Stage 1: systolic 140 -159 mm. Hg or diastolic 90 -99 mm. Hg �Stage 2: systolic ≥ 160 or diastolic ≥ 100 mm. Hg

Review of Hypertension � Definitions �Isolated systolic hypertension: systolic ≥ 140 mm. Hg and diastolic <90 mm. Hg �Isolated diastolic hypertension: systolic <140 mm. Hg and diastolic ≥ 90 mm. Hg

Review of Hypertension � Definitions continued �Malignant hypertension: hypertension with retinal hemorrhages, exudates, or papilledema �Hypertensive encephalopathy �Acute renal failure �Hypertensive urgency: Diastolic blood pressure > 120 mm. Hg without symptoms
 hypertension �Pathogenesis �Increased sympathetic neural activity (beta-adrenergic) �Increased")
Review of Hypertension � Primary (essential) hypertension �Pathogenesis �Increased sympathetic neural activity (beta-adrenergic) �Increased angiotensin II activity �Mineralocorticoid excess �Genetics �Reduced adult nephron mass

Review of Hypertension � Risk Factors �Ethnicity �Genetics �Diet �Sodium intake �Alcohol �Obesity �Tobacco use �Decreased physical activity �Hyperlipidemia �Age > 65 years �Personality Traits �Vitamin D Deficiency

Review of Hypertension � Complications �Risk factor for other disease states �Heart failure �Left ventricular hypertrophy �Stroke �Intra-cerebral hemorrhage �Kidney disease �Malignant hypertension

Review of Hypertension � Treatment benefits �Reduce risk of cardiovascular events, kidney disease, eye damage, morbidity and mortality � Only 46 -51%have blood pressure under control �Poor access to healthcare, medications �Lack of adherence �Side effects, disadvantages of therapy �Benefits not obvious to patients

Treatment of Hypertension Lifestyle Modifications Treatment Algorithm Treatment Goal Medication Classes

Treatment of Hypertension � Lifestyle Modification Systolic BP reduction Sodium restriction 4. 8 mm. Hg (2. 5 mm HG diastolic) Weight loss 0. 5 -2 mm. Hg per 1 kg weight loss Diet (DASH) 2 -8 mm Hg Physical activity 4 -8 mm. Hg Moderation of alcohol consumption 2 -4 mm. Hg
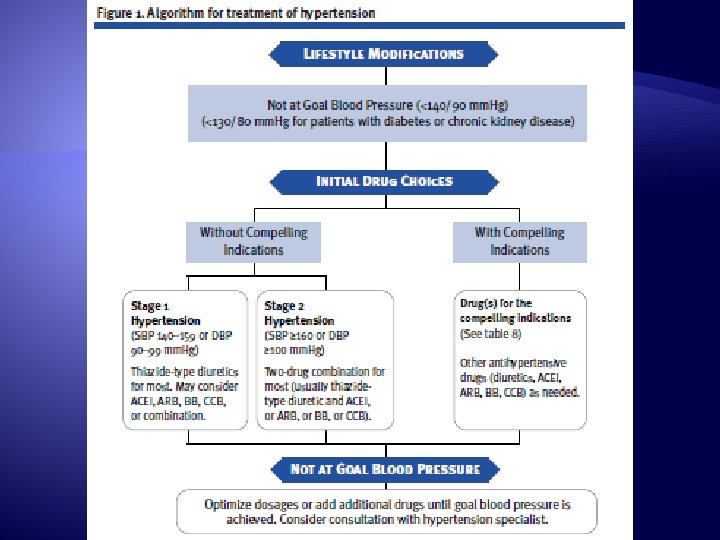

Treatment Goal � JNC 7 blood pressure goals �Generally <140/<90 mm. Hg �Complications or increased risk factors <130/<90 �Diabetes �Chronic kidney disease

Treatment of Hypertension � Medications �Monitor �Blood pressure �Side effects: hypotension, orthostatic hypotension, dizziness
 12. 5 -25 mg daily � Hydrochlorothiazide (Microzide, Hydro.")
Thiazide Diuretics � Chlorthalidone (generic) 12. 5 -25 mg daily � Hydrochlorothiazide (Microzide, Hydro. DIURIL) 12. 5 -50 mg daily � Indapamide (Lozol) 1. 25 -2. 5 mg daily � Metolazone (Zaroxolyn) 2. 5 -5 mg daily

Thiazide Diuretics � Side effects �Hypokalemia �Hypomagnesemia �Hypercalcemia �Hyperuricemia �Hyperglycemia �Hyperlipidemia �Sexual dysfunction �Monitoring � Fluid status � Electrolytes � Renal function �Loses efficacy with Cl. Cr < 40 m. L/min �Dose-related side effects � Limiting dose to chlorthalidone or HCTZ 2550 mg greatly reduces risk of metabolic side effects
 0. 5 -2 mg daily-BID � Furosemide (Lasix) 20")
Loop Diuretics � Bumetanide (Bumex) 0. 5 -2 mg daily-BID � Furosemide (Lasix) 20 -80 mg daily-BID � Torsemide (Demadex) 2. 5 -10 mg daily

Loop Diuretics � Side Effects �Hypokalemia �Hypomagnesemia �Hypocalcemia �Hyperuricemia �Sexual dysfunction � Monitoring �Fluid status � Weight loss/gain �Electrolytes � Usually need electrolyte supplementation �Renal function �Hearing (high doses)
 5 -10 mg daily-BID � Triamterene (Dyrenium) 50 -100")
Potassium-Sparing Diuretics � Amiloride (Midamor) 5 -10 mg daily-BID � Triamterene (Dyrenium) 50 -100 mg daily-BID Aldosterone Antagonists � Eplerenone (Inspra) 50 -100 mg daily � Spironolactone (Aldactone) 25 -50 mg daily

Potassium-Sparing Diuretics/ Aldosterone Antagonists � Side effects �Similar to thiazide diuretics: hypomagnesemia, hypercalcemia, hyperuricemia, sexual dysfunction �Hyperkalemia �Especially eplerenone (contraindicated in impaired renal function or DM II with proteinuria) �Gynecomastia (10% with spironolactone) � Monitoring �Electrolytes, fluid status, renal function
 Inhibitors Benazepril (Lotensin) 10 -40 mg daily � Captopril (Capoten)")
Angiotensin Converting Enzyme (ACE) Inhibitors Benazepril (Lotensin) 10 -40 mg daily � Captopril (Capoten) 25 -100 mg BID � Enalapril (Vasotec) 5 -40 mg daily-BID � Fosinopril (Monopril) 10 -40 mg daily � Lisinopril (Prinivil, Zestril) 10 -40 mg daily � Moexipril (Univasc) 7. 5 -30 mg daily � Perindopril (Aceon) 4 -8 mg daily � Quinapril (Accupril) 10 -80 mg daily � Ramipril (Altace) 2. 5 -20 mg daily � Trandolapril (Mavik) 1 -4 mg daily �
 Inhibitors � Side effects �Hyperkalemia �Dry cough (20%) �Increased serum")
Angiotensin Converting Enzyme (ACE) Inhibitors � Side effects �Hyperkalemia �Dry cough (20%) �Increased serum creatinine/kidney insufficiency �Angioedema (2%) �Rare (<1%) �Neutropenia and agranulocytosis, proteinuria, glomerulonephritis, acute kidney failure � Monitoring: potassium, kidney function � Absolute contraindication in pregnancy
 � Candesartan (Atacand) 8 -32 mg daily � Eprosartan")
Angiotensin II Receptor Blockers (ARBs) � Candesartan (Atacand) 8 -32 mg daily � Eprosartan (Teveten) 400 -800 mg daily-BID � Irbesartan (Avapro) 150 -300 mg daily � Losartan (Cozaar) 25 -100 mg daily-BID � Olmesartan (Benicar) 20 -40 mg daily � Telmisartan (Micardis) 20 -80 mg daily � Valsartan (Diovan) 80 -320 mg daily-BID
 � Side effects �Hyperkalemia �Increased serum creatinine/kidney insufficiency �Possible")
Angiotensin II Receptor Blockers (ARBs) � Side effects �Hyperkalemia �Increased serum creatinine/kidney insufficiency �Possible angioedema (cross-reactivity with ACEIs reported) �No bradykinin-induced dry cough � Monitoring: potassium, kidney function � Should not be used in pregnancy
 180420")
Calcium Channel Blockers � Non-Dihydropyridines �Diltiazem �Extended release (Cardizem CD, Dilacor XR, Tiazac) 180420 mg daily �Extended release (Cardizem LA) 120 -540 mg dialy �Verapamil �Immediate release (Calan, Isoptin ) 80 -320 mg BID �Long acting (Calan SR, Isoptin SR ) 120 -480 mg daily-BID, (Coer, Covera HS, Verelan PM) 120 -360 mg daily † †
 2. 5 -10 mg daily �Felodipine (Plendil)")
Calcium Channel Blockers � Dihydropyridines �Amlodipine (Norvasc) 2. 5 -10 mg daily �Felodipine (Plendil) 2. 5 -20 mg daily �Isradipine (Dynacirc CR) 2. 5 -10 mg daily �Nicardipine sustained release (Cardene SR) 60 -120 mg BID �Nifedipine long-acting (Adalat CC, Procardia XL) 30 -60 mg daily �Nisoldipine (Sular) 10 -40 mg daily

Calcium Channel Blockers � Side effects �Flushing, headache, gingival hyperplasia, peripheral edema �Non-dihydropyridines: bradycardia, AV block (high doses), heart failure, anorexia � Precautions/Contraindications �Contraindicated in heart failure �Multiple drug interactions due to CYP 450 3 A 4 inhibition �Combination of non-dihydropyridine with beta blocker increases chance of heart block
 �Atenolol (Tenormin) 25 -100 mg daily �Metoprolol (Lopressor,")
Beta Blockers � Beta-1 selective (cardioselective) �Atenolol (Tenormin) 25 -100 mg daily �Metoprolol (Lopressor, Toprol XL) 50 -100 mg daily-BID �Betaxolol (Kerlone) 5 -10 mg daily �Bisaprolol (Zebeta) 2. 5 -20 mg daily � Non-selective �Nadolol (Corgard) 40 -120 mg daily �Propranolol (Inderal, Inderal LA) 40 -160 mg BID (60 -180 mg daily for LA) �Timolol (Blocadren) 20 -40 mg BID
 200 -800 mg BID �Penbutolol (Levatol)")
Beta Blockers � Intrinsic sympathomimetic activity �Acebutolol (Sectral) 200 -800 mg BID �Penbutolol (Levatol) 10 -40 mg daily �Pindolol (generic) 10 -40 mg BID � Combined alpha-1 and beta blockers �Carvedilol (Coreg) 12. 5 -50 mg BID �Labetalol (Normodyne, Trandate ) 200 -800 mg BID �Nebivolol (Bystolic) 5 -40 mg daily †

Beta Blockers � Side effects �Bradycardia, heart block, heart failure �Monitoring: HR �Increased blood glucose �Sexual dysfunction (impotence) �Abrupt cessation: rebound hypertension, unstable angina/myocardial infarction �Specific groups �More CNS effects (dizziness/drowsiness ) with more lipophylic agents (propranolol) �Non-selective agents: β 2 -receptor activation, bronchospasm �Non-ISA agents: increased triglycerides
 1 -16 mg daily � Prazosin (Minipress) 2 -20")
Alpha-1 Blockers � Doxazosin (Cardura) 1 -16 mg daily � Prazosin (Minipress) 2 -20 mg BID-TID � Terazosin (Hytrin) 1 -20 mg daily-BID � Side effects � 1 st dose phenomenon: dizziness, palpitations, syncope �Orthostatic hypotension �CNS effects: vivid dreams, depression �Sodium and water retention
 0. 1 -0.")
Central alpha-2 agonists and Other centrally acting drugs � Clonidine (Catapres) 0. 1 -0. 8 mg BID �Clonidine patch (Catapres-TTS) 0. 1 -0. 3 weekly � Clonidine (Catapres) 0. 1 -0. 8 mg BID � Methyldopa (Aldomet ) 250 -1, 000 mg BID † � Reserpine (generic) 0. 1 -0. 25 mg daily � Guanfacine (Tenex ) 0. 5 -2 mg daily †

Central alpha-2 agonists and Other centrally acting drugs � Side effects �Sodium and water retention �Orthostatic hypotension �CNS side effects: depression �Anticholinergic: dry mouth, sedation, constipation, urinary retention, blurred vision �Reserpine: parasympathetic activity (increased secretions, bradycardia) Abrupt cessation: rebound hypertension � Clonidine often used for resistant hypertension � Methyldopa is a first-line agent in pregnancy �
 25 -100 mg BID � Minoxidil (Loniten) 2. 5")
Direct vasodilators � Hydralazine (Apresoline) 25 -100 mg BID � Minoxidil (Loniten) 2. 5 -80 mg daily-BID � Side effects �Sodium and water retention �Tachyphylaxis (use with beta blocker) �Hydralazine �Lupus-like syndrome, dermatitis, drug fever, peripheral neuropathy, hepatitis, vascular HA �Minoxidil �Hypertrichosis (hirsutism of face, arms, back, chest), pericardial effusion, nonspecific T-wave change

Treatment of Hypertension Treatment of hypertension with concurrent disease states or compelling indications Choice of medication for hypertension Treatment of hypertensive urgency & emergency New Recommendations
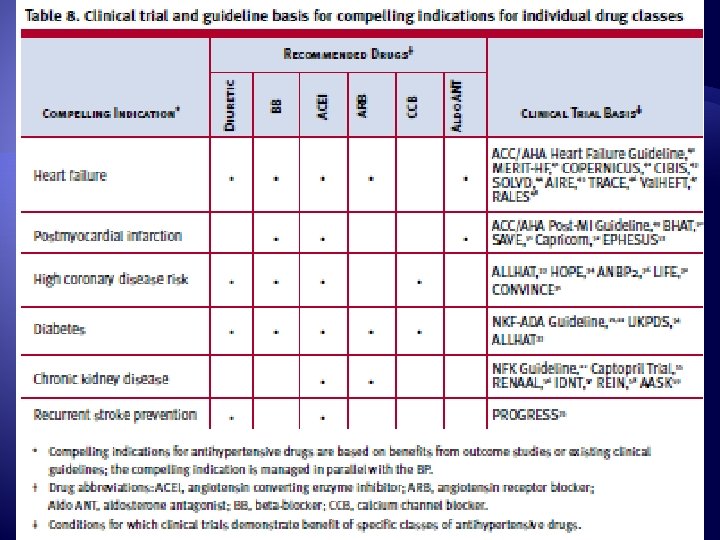

Ischemic Heart Disease � Stable angina �Beta blocker, or CCB � Acute coronary syndrome �Beta blocker (without ISA), ACEI � Post-MI �Beta blocker, ACEI, aldosterone antagonist
, beta blocker � Symptomatic ventricular")
Heart Failure � Asymptomatic heart failure �ACEI (or ARB), beta blocker � Symptomatic ventricular dysfunction or end- stage heart disease �Beta blocker, ACEI or ARB, aldosterone antagonist, loop diuretic

Diabetes � ACEI or ARB �Reduce diabetic nephropathy and albuminuria �ARBs reduce progression to macroalbuminuria � Thiazide diuretics, BBs, ACEIs, ARBs, and CCBs �Prevent CVD and stroke incidence � Caution with beta blockers �Mask signs of hypoglycemia

Chronic Kidney Disease � ACEI or ARB �Slow progression of renal disease �Limited rise in Scr acceptable (up to 35% increase) � Advanced CKD �Loop diuretics (volume control) � Thiazide diuretics lose efficacy with Cl. Cr < 40

Cerebrovascular Disease � Combination of thiazide diuretic and ACEI �Reduce recurrent stroke rate

Left ventricular hypertrophy � All classes of antihypertensive agents except the direct vasodilators hydralazine and minoxidil �Regression of LVH � Severe hypertension with ECG evidence of LVH �ARB �Only indication where ARB has proven benefit over ACEI

Ethnicity � African-American �Monotherapy: thiazide diuretic or CCB �Reduced BP responses with BBs, ACEIs, or ARBs �Caution: ACEI-induced angioedema occurs 2– 4 times more frequently �Heart failure �Hydralazine/Isosorbide dinitrate (Bidil)

Elderly � Follow same principles of therapy � Start at lower doses, increase more slowly �Avoid side effects � Classes to avoid �Alpha-1 blockers, alpha-2 agonists, centrally acting agents, direct vasodilators � Treatment of HTN may slow progression of cognitive impairment and dementia

Pregnancy � Preferred agents �Methyldopa, beta blockers, and vasodilators � Contraindicated: �ACEIs and ARBs
")
Other indications � Atrial tachyarrythmias/fibrillation � Beta blockers or calcium channel blockers (rate control) � Migraine, tremor � Beta blockers � BPH � Alpha-1 blockers � Asthma, reactive airway disease, second or third degree heart block � Avoid beta-blockers (especially non-selective) � Gout, hyponatremia � Avoid thiazide diuretics � Hyperkalemia � Avoid potassium-sparing diuretics, aldosterone antagonists

Choice of initial medication

Choice of initial medication � First line options �Thiazide diuretic �Calcium channel blocker (long acting) �ACEI or ARB � If treatment with second medication likely (ACCOMPLISH trial) �Calcium channel blocker (long acting) �ACEI or ARB

Hypertensive Urgency vs. Emergency � Hypertensive urgency �Severe hypertension: SBP ≥ 180 mm. Hg and/or DBP ≥ 120 mm. Hg �Asymptomatic (other than headache) �No evidence of acute end-organ damage � Hypertensive emergency �Malignant hypertension �Marked hypertension with retinal hemorrhages, exudates, or papilledema �Hypertensive encephalopathy �Acute renal failure (malignant nephrosclerosis)

Hypertensive Urgency � Treatment �Goal: gradual reduction of BP to < 160/100 �Previously: rapid reduction of BP, but no proven benefit �Cerebral or myocardial ischemia or infarction can be induced �Sublingual nifedipine now contraindicated

Hypertensive Urgency � Treatment: oral medications �Previously treated HTN �Increase dose of existing medication or add new medications �Previously untreated HTN �Furosemide 20 mg PO(or higher if renal insufficiency) �Clonidine 0. 2 mg PO �Captopril 6. 25 -12. 5 mg PO �Monitor until BP decreases 20 -30 mm. Hg (or < 160/100) �Prescribe longer acting agent(s), follow-up with provider

Malignant Hypertension � Goal: rapidly reduce DBP to 100 -105 mm. Hg in 2 -6 hours (25% reduction) � Treatment: IV medications �Nitroprusside (Nitropress) �Arteriolar and venous dilator �IV infusion 0. 25 -0. 5 mcg/kg/min �Max 8 -10 mcg/kg /min. �Onset: seconds. Duration of action: 2 -5 minutes �Cyanide toxicity possible with prolonged use �Nicardipine �IV infusion 5 mg/hr; max 15 mg/hr

Malignant Hypertension � Treatment: IV medications �Clevidipine �Dihydropyridine calcium channel blocker �IV infusion 1 mg/hr; max 21 mg/hr �Labetalol �IV bolus 20 mg initially, followed by 20 -80 mg every 10 min �Infusion: 0. 5 -2 mg/min �Max dose 300 mg in 24 hours �Fenoldopam �Peripheral dopamine-1 receptor agonist, �IV infusion 0. 1 mcg/kg/min, titrate as needed every 15 minutes

Malignant Hypertension � Treatment: oral medications �Not recommended unless IV meds not available �Uncontrolled hypotensive response �Sublingual nifedipine 10 mg �Sublingual captopril 25 mg � Monitoring �When BP controlled, switch to oral therapy �Decrease DBP to 85 -90 mm. Hg over 2 -3 months

What’s to come?

New Recommendations � Chlorthalidone preferred over HCTZ �More potent �Longer acting �Potential lower risk of cardiovascular events � Beta blockers should NOT be used as 1 st line therapy �In absence of compelling indications �Especially for patient’s > 60 years old � Higher SBP goals may be more appropriate �Elderly: <150/<60 �Diabetes: SBP < 130 may not improve CV risk

References � � � � Chobanian AV, Bakris GL, Black HR et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 2003; 42(6): 1206 -52. Cupp M. Antihypertensives. Pharmacist’s Letter 2013; 29(4): 290401. [Electronic version]. Available at: http: //www. pharmacistsletter. com. Accessed April 14, 2013. DRUGDEX® System [Internet database]. Greenwood Village, Colo: Thomson Healthcare. Updated periodically. Kaplan NM. Malignant hypertension and hypertensive encephalopathy in adults. In: Up. To. Date, Basow, DS (Ed), Up. To. Date, Waltham, MA, 2013. Kaplan NM, Domino FJ. Overview of hypertension in adults. In: Up. To. Date, Basow, DS (Ed), Up. To. Date, Waltham, MA, 2013. Lacy CF, Armstrong LL, Goldman MP, Lance LL. Lexi-Comp’s Drug Information Handbook. 17 th ed. Hudson (OH): Lexi-Comp; 2008. Saseen JJ, Carter BL. Hypertension. In: Di. Piro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM, editors. Pharmacotherapy. A Pathophysiologic Approach. 6 th ed. New York (NY): Mc. Graw Hill; 2005: 185 -218. Systematic Evidence Reviews in Development: Cardiovascular Disease Risk Reduction in Adults (June 2013). National Institutes of Health Web site. Available at: http: //www. nhlbi. nih. gov/guidelines/indevelop. htm#status. Accessed August 14, 2013.
- Slides: 60