Antidiabetic drugs Dr Hashem Mansour Introduction Diabetes mellitus

Antidiabetic drugs Dr. Hashem Mansour

 It is a metabolic disorder characterized by hyperglycaemia, glycosuria, hyperlipidaemia,")
Introduction �Diabetes mellitus (DM) It is a metabolic disorder characterized by hyperglycaemia, glycosuria, hyperlipidaemia, negative nitrogen balance and sometimes ketonaemia. �A widespread pathological changes resulting in macrovascular, microvascular and metabolic complications

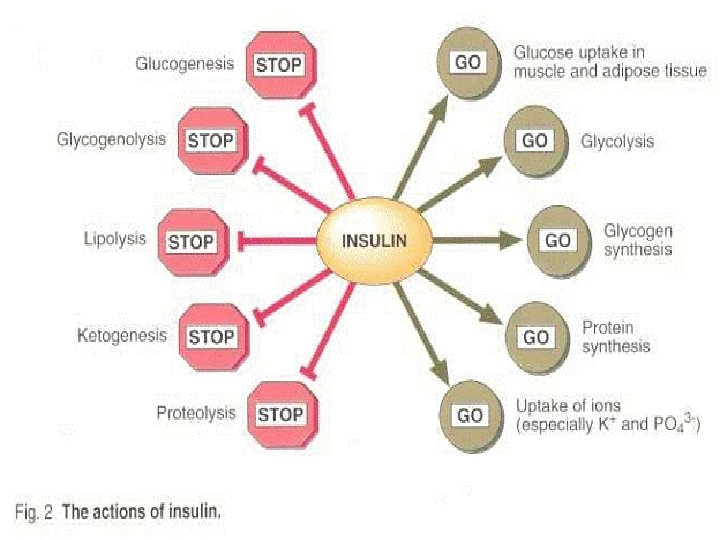
Insulin Action �The insulin receptor is expressed on all human cells. �Tissues that are critical for regulation of blood glucose are liver, skeletal muscle, fat, and specific regions of the brain and the pancreatic islet. �The actions of insulin is anabolic, and insulin promote the uptake, use, and storage of the major nutrients: glucose, lipids, and amino acids. �Insulin stimulates glycogenesis, lipogenesis, and protein synthesis; it also inhibits the catabolism of these compounds.

Insulin action In fasting state

Insulin action in prandial state

Types of DM �The ADA recognizes four clinical classifications: �Type 1 diabetes (formerly insulin- dependent D. M). �Type 2 diabetes (formerly non–insulin-dependent D. M). �Gestational diabetes is defined as carbohydrate intolerance with onset or first recognition during pregnancy. �Uncontrolled gestational diabetes can lead to fetal macrosomia (abnormally large body) and shoulder dystocia (difficult delivery), as well as neonatal hypoglycemia.

Type 1 vs type 2

Nonpharmacologic Aspects of Diabetes Therapy �Diabetic pt should be educated about nutrition, exercise, and medications aimed at lowering the plasma glucose. �In type 1 diabetes, matching caloric intake and insulin dosing is important. �In type 2 diabetes, the diet is directed at weight loss and reduction of blood pressure and atherosclerotic risk.

Insulin � Is a polypeptide hormone consisting of two peptide chains that are connected by disulfide bonds. �It is synthesized as a precursor (proinsulin) that undergoes proteolytic cleavage to form insulin and C-peptide, both of which are secreted by the β cells of the pancreas. �Thus, measurement of C-peptide provides a better index of insulin levels.

Actions of Insulin �It facilitates glucose transport across cell membrane and alters the activity of enzymes involved in carbohydrate, fat and protein metabolism in liver, muscle and adipose tissue to lower blood glucose level. �Concurrently, the actions prevent rise in free fatty acid level, ketone production and protein breakdown of the diabetic state.

Pharmacokinetics and fate �Insulin preparations vary primarily in their onset and duration of activity. �Dose, injection site, blood supply, temperature, and physical activity can also affect the onset and duration of various insulin preparations. �Administered by S. C or I. V or continuous S. C insulin infusion called the insulin pump. �D. Nav insulin pump is the first basal bolus pump for type II DM approved 4/3/2019. �The pump is programmed to deliver a basal insulin in addition to a bolus of insulin to cover

Onset of action Insulin preparations

Adverse reactions to insulin �Hypoglycemia is the most serious and common adverse reaction to insulin. �Weight gain. �Local injection site reactions. �Lipodystrophy, can be minimized by rotation of injection sites. �Diabetics with renal insufficiency may require a decrease in insulin dose.

Adverse effects

Goal of treatment of DM �The purpose of therapy in diabetes mellitus is to restore metabolism to normal, avoid symptoms due to hyperglycaemia and glucosuria, prevent short term complications (infection, ketoacidosis, etc. ) and long-term squeals (cardiovascular, retinal, renal, etc. )
 Not controlled by diet and")
When to use of insulin in D. M (i) Not controlled by diet and exercise. (ii) Primary or secondary failure of oral hypoglycaemics. (iii) Underweight patients. (iv) Temporarily to tide over infections, trauma, surgery, pregnancy and during labour. (v) Any complication of diabetes, e. g. ketoacidosis, diabetic or non-ketotic hyperosmolar coma, gangrene of extremities.


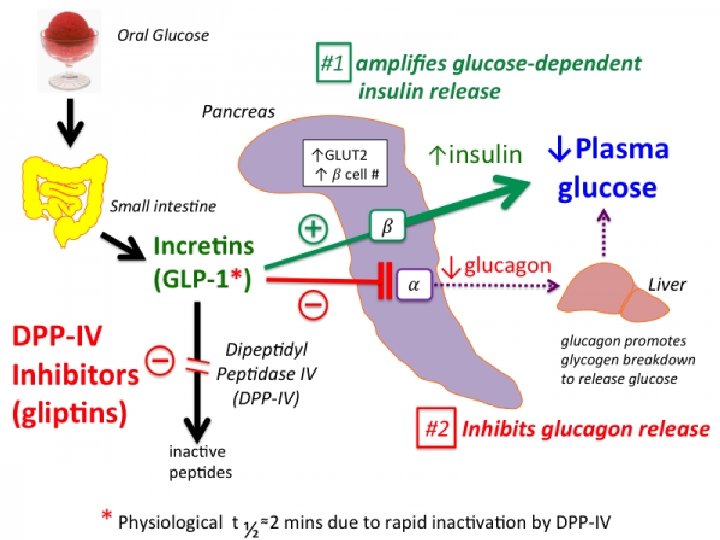
INCRETIN MIMETICS �Oral glucose results in a higher secretion of insulin than occurs when an equal load of glucose is given IV. �This effect is referred to as the “incretin effect” and is markedly reduced in type 2 diabetes. �The incretin effect occurs because the gut releases incretin hormones, notably glucagon like peptide-1 (GLP-1) and glucosedependent insulinotropic polypeptide, in response to a meal.

Mechanism of action �The incretin mimetics are analogs of GLP-1 that exert their activity by acting as GLP-1 receptor agonists. �These agents improve glucose dependent insulin secretion, slow gastric emptying time, reduce food intake by enhancing satiety, decrease postprandial glucagon secretion, and promote β-cell proliferation. �Consequently, weight gain and postprandial hyperglycemia are reduced, and Hb. A 1 c levels decline.

Pharmacokinetics and fate �Exenatide and liraglutide must be administered S. C. �Liraglutide has a long half-life, allowing for once-daily dosing without regard to meals. �A once-weekly extended-release preparation of liraglutide is also available. �Semaglutide is the first oral GLP 1 approved orally for type 2 DM and CKD on 24/7/2019. �This group is the best choice for T 2 DM among CHF and CKD patients.

Adverse effects �The main adverse effects of the incretin mimetics consist of nausea, vomiting, diarrhea, and constipation and pancreatitis. �Patients should be advised to discontinue these agents immediately if they experience severe abdominal pain.

Oral hypoglycemic �SULFONYLUREAS: Glyburide, Glipizide, Gliclazide, Glimepiride �BIGUANIDE: Metformin �MEGLITINIDE: Repaglinide Nateglinide �THIAZOLIDINEDIONES: Rosiglitazone Pioglitazone �DIPEPTIDYL PEPTIDASE-4 (DPP-4) INHIBITOR: Sitagliptin, Vildagliptin �Sodium glucose cotransporte inhibitors SGLT 2 inhibitors: canagliflusin

Sulfonylureas �These agents are classified as insulin secretagogues, because they promote insulin release from the β cells. �Mechanism of action: Stimulation of insulin release from the β cells of the pancreas. �In addition, sulfonylureas may reduce hepatic glucose production and increase peripheral insulin sensitivity.

Pharmacokinetics and fate �Given orally �These drugs bind to serum proteins �Metabolized by the liver �Excreted in the urine and feces. �The duration of action ranges from 12 to 24 hours.

Adverse effects �Weight gain, hyperinsulinemia, and hypoglycemia. �They should be used with caution in hepatic impairment. �Contra indicated in Renal impairment increase the risk of hypoglycemia. �Glipizide is safer options in renal dysfunction and in elderly patients.

General adverse effects of oral hypoglycemic drugs


Glinides �Glinides (repaglinide and nateglinidea 0 are also considered insulin secretagogues. �Mechanism of action: Stimulate insulin secretion. �Have a rapid onset and a short duration of action. �They promote release of insulin that occurs after a meal and are categorized as postprandial glucose regulators.

Pharmacokinetics and fate �Glinides should be taken prior to a meal and are well absorbed after oral administration. �Both glinides are metabolized to inactive products by the liver �Excreted through the bile.

Adverse effects �Glinides can cause hypoglycemia and weight gain, the incidence is lower than that with sulfonylureas. �These agents should be used with caution in patients with hepatic impairment.

Biguanides �Metformin the only biguanide, is classified as an insulin sensitizer. �It increases glucose uptake by target tissues, thereby decreasing insulin resistance. �Metformin does not promote insulin secretion. �Therefore, hyperinsulinemia is not a problem, and the risk of hypoglycemia is far less than that with sulfonylureas.

Mechanism of action �Presence of some insulin is essential for their action. � 1. Suppress hepatic gluconeogenesis and glucose output from liver: the major action. � 2. Enhance insulin-mediated glucose disposal in muscle and fat. � 3. Retard intestinal absorption of glucose, amino acids and vit B 12. � 4. Promote peripheral glucose utilization by enhancing anaerobic glycolysis.

Pharmacokinetics and fate �Metformin is well absorbed orally. �Is not bound to serum proteins �Is not metabolized. �Excretion is via the urine.

Adverse effects �These are largely gastrointestinal. �Metformin is contraindicated in sever renal dysfunction due to the risk of lactic acidosis. �It should be discontinued in cases of acute myocardial infarction, exacerbation of heart failure, sepsis, or other disorders that can cause acute renal failure. �Metformin should be used with caution in patients older than 80 years and in those with heart failure. �It should be temporarily discontinued in patients undergoing procedures requiring IV radiographic contrast. �Decrease vitamin B 12 absorption.

Other uses �In addition to type 2 diabetes, metformin is effective in the treatment of polycystic ovary syndrome. �It lowers insulin resistance seen in this disorder and can result in ovulation and, therefore, possibly pregnancy. �In the last year 3/2019 study found that metformin is beneficial n reducing VTE among diabetic patients
 are also insulin sensitizers. �The two members of this class")
Thiazolidinediones �The thiazolidinediones (TZDs) are also insulin sensitizers. �The two members of this class are pioglitazone and rosiglitazone. �Although insulin is required for their action, the TZDs do not promote its release from the β cells, so hyperinsulinemia is not a

Mechanism of action �The TZDs lower insulin resistance by acting as agonists for the peroxisome proliferator–activated receptor-γ (PPARγ), a nuclear hormone receptor. �Activation of PPARγ resulting in increased insulin sensitivity in adipose tissue, liver, and skeletal muscle.

Pharmacokinetics and fate �Well absorbed after oral administration. �Undergo extensive metabolism by liver. �Excreted in the bile and eliminated in the feces. �No dosage adjustment is required in renal impairment. �These agents should be avoided in nursing mothers.

Adverse effects �Liver toxicity need periodic monitoring of liver function �Weight gain can occur because TZDs may increase subcutaneous fat and cause fluid retention. �Contra indicated in patients with severe heart failure. �Osteopenia and increased fracture risk. �Other uses: As with metformin, TZDs can resume ovulation in premenopausal women with polycystic ovary syndrome.

")
Dipeptidyl peptidase-4 inhibitors �Vildagliptin , linagliptin, saxagliptin, and sitagliptinare orally active dipeptidyl peptidase-4 (DPP-4) inhibitors used for the treatment of type 2 diabetes.

Mechanism of action �These drugs inhibit the enzyme DPP-4, which is responsible for the inactivation of incretin hormones such as GLP-1. �Prolonging the activity of incretin hormones increases insulin release in response to meals and reduces inappropriate secretion of glucagon. �These drugs are weight neutral.

Pharmacokinetics and fate �Well absorbed after oral administration. �Metabolized by liver �The primary route of elimination is renal. �Adverse effects: Nasopharyngitis and headache. Dizzy, diarrhea, pancreatitis has occurred with use of all DPP-4 inhibitors. �Saxagliptin had an increase in hospitalization for heart failure.

Sodium–glucose cotransporter 2 inhibitors � Canagliflozin, empaglifluzin and dapagliflozin are the agents in this category of drugs for type 2 diabetes. � Sotaglifluzin is recently approved for type I DM in Europe on 1/3/2019
 is responsible for reabsorbing filtered")
Mechanism of action �The sodium–glucose cotransporter 2 (SGLT 2) is responsible for reabsorbing filtered glucose in the tubular lumen of the kidney. �By inhibiting SGLT 2, these agents decrease reabsorption of glucose, increase urinary glucose excretion, and lower blood glucose. �Inhibition of SGLT 2 also decreases reabsorption of sodium and causes osmotic diuresis. �Therefore, SGLT 2 inhibitors may reduce systolic blood pressure.

Pharmacokinetics and fate �These agents are given once daily in the morning. �Metabolized by liver. �Excretion for canagliflozin is via the feces, about one-third of a dose is renally eliminated. �These agents should be avoided in patients with 3 rd stage renal impairment except Dapaglifluzin is used in this category of renal disease.

Adverse Effects; Drug Interactions �Urinary tract infections and genital mycotic infections. �Urine glucose losses cause mild diuresis, which can lead to hypotension usually older, patients. �Recent analyses of clinical trials with SGLT inhibitors suggested that they may increase the risk of fractures. �Rare cases of diabetic ketoacidosis reported. �Canagliflozin is associated with an increased risk of lower extremity amputation

Indication �These are the best drugs among patients with type 2 DM and CHF or cardiac disease. �In 30/9/2019 canaglifluzine approved to dreduce risk of end stage renal diseasde, worsening of kidney function, reduce cardiovascular death and heart failure hospitalization among patiets with type 2 DM. �In 21/10/2019 dapaglifluzine approved to dreduce risk of heart failure hospitalization and cardiovascular risk factors among patiets with type 2 DM.

Emerging Therapies for Diabetes �Activators of GK, glucagon antagonists, and inhibitors of 11β-hydroxysteroid dehydrogenase are being investigated as novel therapies for type 2 diabetes. �Imiglimin the first drug of new generation of antidiabetic drug group (glimin) will approve next year. �Most of these incorporate GLP-1 receptor agonism with the capacity to activate receptors for glucagon, GIP, or gastrin. �These compounds have been potent in pre-clinical models and are now in human trials. Some drugs developed for type 2 diabetes are being tested as adjunctive therapy for type 1 diabetes

Physiotherapy implication �Over weight , hypoglycemia or hyperglycemia are limited factors for physiotherapy. �Hyper or hypoglycemia can cause coma, so before physiotherapy session you should measure blood sugar level. �Overweight limit movement and exercise. �Sweet or sugar must be available to overcome hypoglycemia. �Adverse drug reactions should kept in mindespecially hypoglycemia.

- Slides: 57