ANTIDEPRESSANTS Samaiya Mushtaq CHEM 5398 DEPRESSION Types Symptoms


 Atypical depression Bipolar disorder/Manic depression Seasonal")
")




 AND DEPRESSION MAO catalyze deamination of intracellular monoamines MAO-A oxidizes epinephrine,")
 History Isoniazid Iproniazid Current Drugs Mechanism of Action Side Effects")
 Phenelzine (Nardil) Tranylcypromine (Parnate) Isocarboxazid (Marplan) MAO-B")




 History Imipramine Current Drugs Mechanism of Action Side Effects Imipramine")
 Doxepin (Sinequan) Imipramine (Tofranil, Tofranil-PM) Nortriptyline (Pamelor)")



 Current Drugs Mirtazapine Mechanism of Action Same (Remeron) as TCAs Side")

 dapoxetine (Priligy) escitalopram (Lexapro) fluoxetine (Prozac) fluvoxamine (Luvox)")


 Side effects more manageable")
 Slightly greater efficacy than SSRIs Slightly fewer adverse effects than")

 Current drugs Bupropion (Wellbutrin) Mechanims of Action Similar to SSRIs")



- Slides: 33
ANTIDEPRESSANTS Samaiya Mushtaq CHEM 5398
DEPRESSION Types Symptoms Diagnosis Causes Treatment
TYPES OF DEPRESSION Major depression Chronic depression (Dysthymia) Atypical depression Bipolar disorder/Manic depression Seasonal depression (SAD)
SYMPTOMS persistently sad, anxious, or empty moods loss of pleasure in usual activities (anhedonia) feelings of helplessness, guilt, or worthlessness crying, hopelessness, or persistent pessimism fatigue or decreased energy loss of memory, concentration, or decision-making capability restlessness, irritability sleep disturbances change in appetite or weight physical symptoms that defy diagnosis and do not respond to treatment (especially pain and gastrointestinal complaints) thoughts of suicide or death, or suicide attempts poor self-image or self-esteem (as illustrated, for example, by verbal self-reproach)
DIAGNOSIS Extensive patient and family history Blood test for hypothyroidism Current medication DSM-IV One of the first two symptoms Five other symptoms
CAUSES OF DEPRESSION Genetics Death/Abuse Medications
TREATMENT FOR DEPRESSION Psychotherapy Electroconvulsive therapy Natural alternatives Medication SSRIs MAOIs TCAs SNRIs NDRIs Te. CAs
NEUROTRANSMITTERS AND THE CATECHOLAMINE HYPOTHESIS Neurotransmitters pass along signal Smaller amount of neurotransmitters causes depression
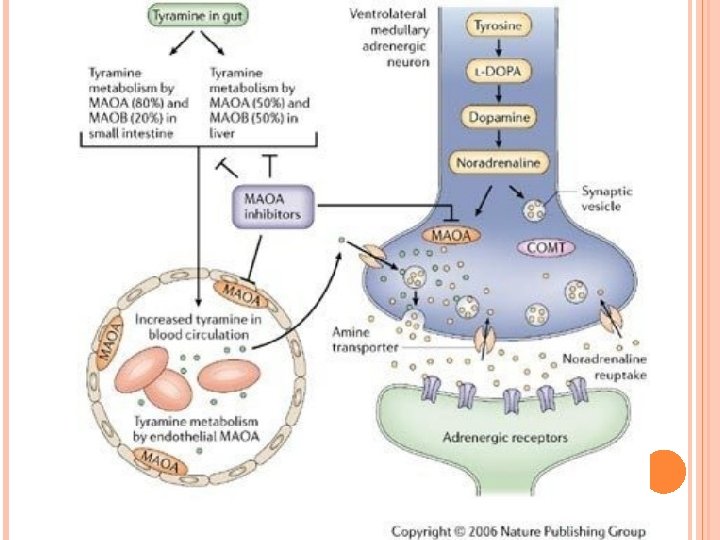
MONOAMINE OXIDASE (MAO) AND DEPRESSION MAO catalyze deamination of intracellular monoamines MAO-A oxidizes epinephrine, norepinephrine, serotonin MAO-B oxidizes phenylethylamine Both oxidize dopamine nonpreferentially MAO transporters reuptake extracellular monoamine
MONOAMINE OXIDASE INHIBITORS (MAOIS) History Isoniazid Iproniazid Current Drugs Mechanism of Action Side Effects Isoniazid Iproniazid
MAOIS ON THE MARKET MAO Inhibitors (nonselective) Phenelzine (Nardil) Tranylcypromine (Parnate) Isocarboxazid (Marplan) MAO-B Inhibitors (selective for MAO-B) Selegiline (Emsam)
MAOIS MECHANISM OF ACTION MAO contains a cysteinyl-linked flavin MAOIs covalently bind to N-5 of the flavin residue of the enzyme
MAOIS SIDE EFFECTS Drowsiness/Fatigue Constipation Nausea Diarrhea Dizziness Low blood pressure Lightheadedness, Decreased urine output Decreased sexual function Sleep disturbances Muscle twitching Weight gain Blurred vision Headache Increased appetite Restlessness Shakiness Weakness Increased sweating
MAOIS SIDE EFFECTS Side effects have put MAOIs in the second or third line of defense despite superior efficacy MAO-A inhibitors interfere with breakdown of tyramine High tyramine levels cause hypertensive crisis (the “cheese effect”) Can be controlled with restricted diet MAOIs interact with certain drugs Serotonin syndrome (muscle rigidity, fever, seizures) Pain medications and SSRIs must be avoided
THE RECEPTOR SENSITIVITY HYPOTHESIS Supersensitivity and up-regulation of post-synaptic receptors leads to depression Suicidal and depressed patients have increased 5 HT-α 2 receptors
TRICYCLIC ANTIDEPRESSANTS (TCAS) History Imipramine Current Drugs Mechanism of Action Side Effects Imipramine
TCAS ON THE MARKET Amitriptyline Desipramine (Norpramin) Doxepin (Sinequan) Imipramine (Tofranil, Tofranil-PM) Nortriptyline (Pamelor) Protriptyline (Vivactil) Trimipramine (Surmontil)
TCAS MECHANISM OF ACTION TCAs inhibit serotonin, norepinephrine, and dopamine transporters, slowing reuptake TCAs also allow for the downregulation of post-synaptic receptors All TCAs and SSRIs contain an essential amino group that appears to interact with Asp-98 in h. SERT
TCAS SIDE EFFECTS Muscarinic M 1 receptor antagonism - anticholinergic effects including dry mouth, blurred vision, constipation, urinary retention and impotence Histamine H 1 receptor antagonism - sedation and weight gain Adrenergic α receptor antagonism - postural hypotension Direct membrane effects - reduced seizure threshold, arrhythmia Serotonin 5 -HT 2 receptor antagonism - weight gain (and reduced anxiety)
TCAS SIDE EFFECTS Nonselectivity results in greater side effects TCAs can also lead to cardiotoxicity Increased LDH leakage Slow cardiac conduction High potency can lead to mania Contraindicated with persons with bipolar disorder or manic depression
TETRACYCLIC ANTIDEPRESSANTS (TECAS) Current Drugs Mirtazapine Mechanism of Action Same (Remeron) as TCAs Side Effects
SELECTIVE SEROTONIN REUPTAKE INHIBITORS Most commonly prescribed class Current drugs Mechanism of action Side effects Serotonin
SSRIS ON THE MARKET citalopram (Celexa) dapoxetine (Priligy) escitalopram (Lexapro) fluoxetine (Prozac) fluvoxamine (Luvox) paroxetine (Paxil) sertraline (Zoloft) zimelidine (Zelmid) (discontinued) indalpine (Upstene) (discontinued) Fluoxetine 1: 1 Sertraline
SSRIS MECHANISM OF ACTION Exact mechanism remains uncertain Ser-438 residue in the human serotonin transporter (h. SERT) appears to be a determining factor in SSRI potency Antidepressants interact directly with h. SERT http: //www. mayoclinic. com/health/antidepressants/ MM 00660
SSRIS SIDE EFFECTS Anhedonia Apathy Nausea/vomiting Drowsiness or somnolence Headache Bruxism (involuntarily grinding of the teeth) Extremely vivid and strange dreams Dizziness Fatigue Changes in sexual behavior Suicidal thoughts
SSRIS SIDE EFFECTS Many disappear within 4 weeks (adaption phase) Side effects more manageable compared to MAOIs and TCAs Sexual side effects are common SSRI cessation syndrome Brain zaps Sexual dysfunction
SEROTONIN-NOREPINEPHRINE REUPTAKE INHIBITORS (SNRIS) Slightly greater efficacy than SSRIs Slightly fewer adverse effects than SSRIs Current drugs Venlafaxine (Effexor) Duloxetine (Cymbalta) Mechanism of Action Very similar to SSRIs Works on both neurotransmitters Side effects Similar Suicide to SSRIs Venlafaxine 1: 1 Duloxetine
NOREPINEPHRINE-DOPAMINE REUPTAKE INHIBITORS (NDRIS) Current drugs Bupropion (Wellbutrin) Mechanims of Action Similar to SSRIs and SNRIs More potent in inhibiting dopamine Also anα 3 -β 4 nicotinic antagonist Adverse effects Lowers Bupropion 1: 1 seizure threshold Suicide Does not cause weight gain or sexual dysfunction (even used to treat the two)
ASSIGNED READING An Introduction to Medicinal Chemistry, by Graham L. Patrick, Chapter 20, pp. 593 -8. Kelly, John. Novel therapeutic targets for the treatment of depression. Current Medicinal Chemistry: Central Nervous System Agents (2003), 3(4), 311 -322. Optional Reading: Wong, David T. ; Perry, Kenneth W. ; Bymaster, Frank P. Case History: The Discovery of Fluoxetine Hydrochloride (Prozac). Nature Reviews Drug Discovery (2005), 4(9), 764 -774. Krishnan, K. Ranga. Revisiting monoamine oxidase inhibitors. Journal of Clinical Psychiatry (Memphis, TN, United States) (2007), 68(Suppl. 8), 35 -41.
HOMEWORK QUESTIONS 1. Many of the medications to treat depression are thought to involve systems utilizing the monoamine neurotransmitters, noradrenaline, dopamine, and serotonin (5 -HT). Draw the structures of these neurotransmitters. Why are they called monoamines? Illustrate their structural resemblance to one another. 2. Monoamine oxidase inhibitors (MAOIs) increase CNS synaptic concentrations of these monoamines by inhibiting an enzyme responsible for their degradation. Draw the reaction scheme for the biological degradation of noradrenaline by monoamine oxidase. 3. Illustrate how the TCAs and SSRIs might resemble the monoamine neurotransmitters, providing one example of each class of antidepressant.
REFERENCES http: //ajp. psychiatryonline. org/cgi/reprint/157/11/1901 http: //www. webmd. com/depression/ http: //pn. psychiatryonline. org/content/41/24/21. full http: //www. mayoclinic. com/health/maois/MH 00072 http: //www. springerlink. com/content/b 9 b 8668 ff 59 f 89 d 7/fulltext. pdf http: //www. emsam. com/pi_emsam. pdf http: //www. nevdgp. org. au/info/topics/depression_theory. htm http: //www. uspharmacist. com/content/t/psychotropic_disorders/c/11467/ http: //www. jbc. org/content/284/15/10276. full. pdf+html http: //www. aafp. org/afp/981200 ap/cadieux. html http: //www. mayoclinic. com/health/antidepressants/MH 00071 http: //books. google. com/books? id=R 0 W 1 Erps. Qpk. C&pg=PA 565&lpg=PA 565&dq=tcas+mechanism+of+ action&source=bl&ots=o. ASle 2 Zpr&sig=36 CB_3 JY 4 u. D 3 LIYvq. XWm. Ab 3 nli. Y&hl=en&ei=Hzf. FS 9 Or. B 4 Tu 9 g. TD 6_ix. Dg&sa=X&oi=book_res ult&ct=result&resnum=8&ved=0 CCo. Q 6 AEw. Bw#v=onepage&q=tcas%20 mechanism%20 of%20 action&f= false http: //www. informaworld. com/smpp/content~content=a 916036122&db=all