Antidepressant Antianxiety Drugs Dr R K Dixit Professor



 Depression ¨Adverse life events. ¨Physical illness. ¨Drugs. ¨Other psychiatric disorders.")
 Depression ¨ More than 60% of all depressions. ¨ Core depressive syndrome:")



 and most frequently cycles with Major/endogenous depression (Manic-Depressive Disease,")








 • CM Moclobemide , Clorgyline A • RITA-Don't-")
. 2. Inhibition of NE and")
 an enzyme Two types n MAO – A n -Peripheral")


 n Moclobemiden Reversible and selective MAO-A inhibitor n Short")
 n Imipramine represents the class (Prototype) n Inhibit monoamine reuptake (serotonin")
 n In Normal person n - Tiredness Light-headedness Sleepiness Difficulty in")


 Good oral absorption n Highly bound to Proteins (plasma and tissue) n")

 n n Usually suicidal attempt Presents as n Excitement n delirium,")
 n n n n n Potentiation of sympathomimetics (direct acting) Reduce action")

 n Limitations of TCAs n Anticholinergic effects n Alpha")













 n Chlordiazepoxide n n First BZD Long lasting effect Chronic anxiety")






- Slides: 57
Antidepressant, Anti-anxiety Drugs Dr. R. K. Dixit Professor Pharmacology and Therapeutics C. S. M. Medical University Lucknow, 226003
Classification of Major Affective Disorders
Episodal (reactive) Depression ¨Adverse life events. ¨Physical illness. ¨Drugs. ¨Other psychiatric disorders.
Reactive (episodal) Depression ¨ More than 60% of all depressions. ¨ Core depressive syndrome: feelings of misery, apathy, inadequacy, pessimism, anxiety, tension, guilt. Ugliness, Low self –esteem, ¨ Bodily complaints
Withdrawn. n Loss of interest in pleasurable activities. n Indecisiveness, loss of motivation. n Retardation of thought and action. n Sleep disturbance n
In severe cases, it is accompanied by hallucinations and delusions. n Recurrent suicidal ideation, a suicide attempt or a specific suicide plan. n • significant weight change (without dieting ) • Psychomotor agitation or retardation.
1. Has a genetic component. 2. Depression can be drug-induced. 3. Depression can be drug-repressed. 4. Depression can be treated with drugs. 5. Depression can be treated with Electroconvulsive Therapy (ECT).
Mania alone is rare (10%) and most frequently cycles with Major/endogenous depression (Manic-Depressive Disease, Bipolar Disorder). Core Symptoms: ØCharacterized by an elevated “high” mood. ØTalkative, go on-and-on about the things they will do. ØIncreased self-esteem. ØAuditory hallucinations. ØDecrease need to sleep. Expensiveness, unnecessary buying. ØLack judgment, Supermen
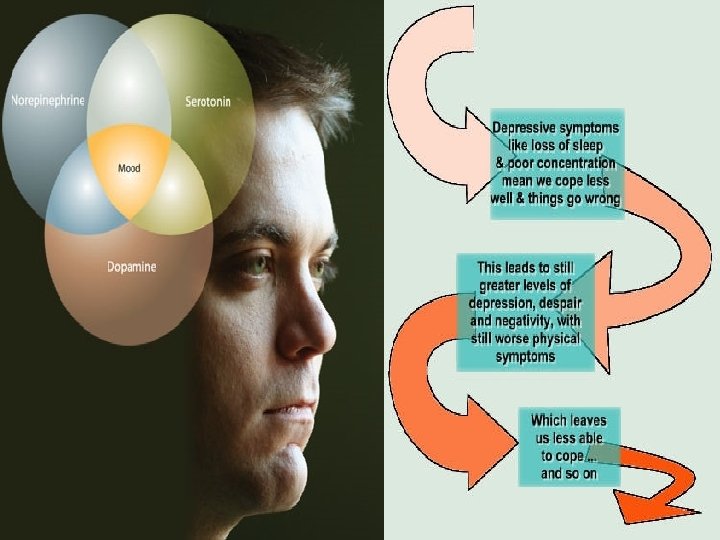
n The precise cause of affective disorders remains elusive. n Evidence implicates alterations in the firing patterns of a subset of biogenic amines in the CNS, Norepinephrine (NE) and Serotonin (5 -HT). Activity of NE and 5 -HT systems? .
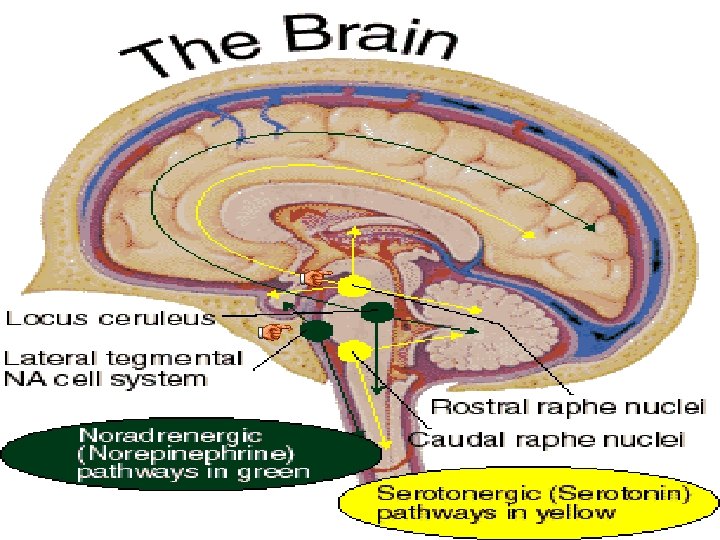
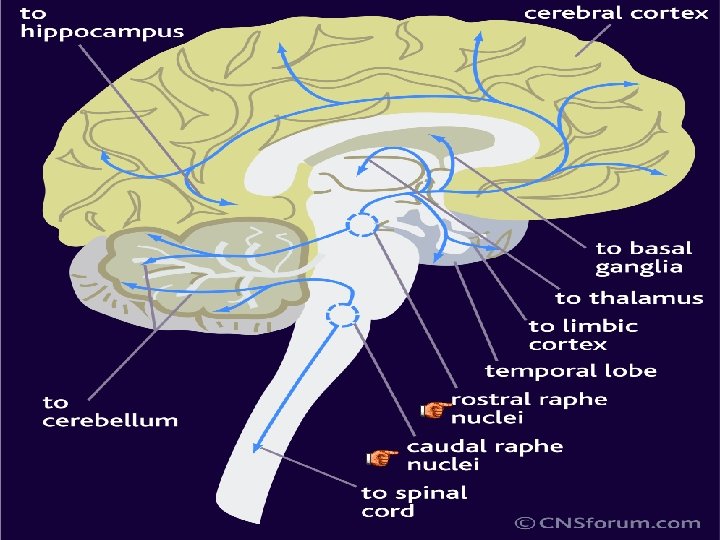
Almost all NE pathways in the brain originate from the cell bodies of neuronal cells in the locus coereleus in the midbrain, which send their axons diffusely to the cortex, cerebellum and limbic areas (hippocampus, amygdala, hypothalamus, thalamus). Ø Mood: -- higher functions performed by the cortex. Ø Cognitive function: -- function of cortex. Ø Drive and motivation: -- function of brainstem Ø Memory and emotion: -- function of the hippocampus and amygdala. Ø Endocrine response: -- function of hypothalamus.
Serotonin System As with the NE system, serotonin neurons located in the pons and midbrain (in groups known as raphe nuclei) send their projections diffusely to the cortex, hippocampus, amygdala, hypothalamus, etc. --same areas implicated in depression. This system is also involved in: • • • Anxiety. Sleep. Sexual behavior. Temperature regulation. CSF production.
Blocked by Blocked antidepressants by antidepressants
Serotonin receptors n 5–HT 1 n subtypes n n n 5–HT 1 A, 5–HT 1 B, 5–HT 1 D, 5– HT 1 E, 5–HT 1 F primarily responsible for therapeutic (antidepressant) effects of increased intrasynaptic serotonin 5–HT 2 n subtypes n n 5–HT 2 A, 5–HT 2 B, 5–HT 2 C primarily responsible for the toxic effects of increased intrasynaptic serotonin
Serotonin receptors Over all 14 types divided in to 1, 2, 3, and 4 -7 family n All are G-protein coupled receptors except 3 n 1 - decreases c. AMP while 4 -7 increase n 3 - ligand gated cation channel n
Alternative Therapies No way of a priori knowing which therapy will be best for a patient. n n Light Therapy Psychological Treatment ECT (patients with suicidal tendency and for quick action) St. John’s Wort (Plant)
Antidepressants A M Is SSR s I SSR Venflaxine V e n f l a x i n e TCAs O Is dox SSRIs T n TCAs epi CA MAOIs n s MAO Is TCAs e MAOIs d i z s a x I o b r O a TCAs c A iso M MAOIs maprotiline MAOIs. A SSRIs mo xe p. MAOIs Venflaxine i n e n i e l y t p i r t r No
? Reversible inhibitor of MAO-A (RIMAs) • CM Moclobemide , Clorgyline A • RITA-Don't- Copy n (Isocarboxacid, phenelzine, tranylcypromine. ) N • Exams-For-PCS T • MAD-Boy-turned-violent I Tricyclic antideprssants (TCAs) D E NA + 5 HT reuptake inhibitor Predominantly NA reuptake inhibitor P Imipramine, Amitriptyline Desipramine, Nortriptyline R Amoxapine, Reboxetine Trimipramine, Doxepin E S Dothiepin, Clomipramine S A N T Selective serotonin reuptake Atypical antidepressants S inhibitors (SSRIs) Trazodone, Mianserine Fluoxetine, Fluvoxamine Mirtazapine, Venlafaxine Duloxetine, Tianeptine Paroxetine, Sertraline Amineptine, Bupropion Citalopram, Escitalopram ? ? ?
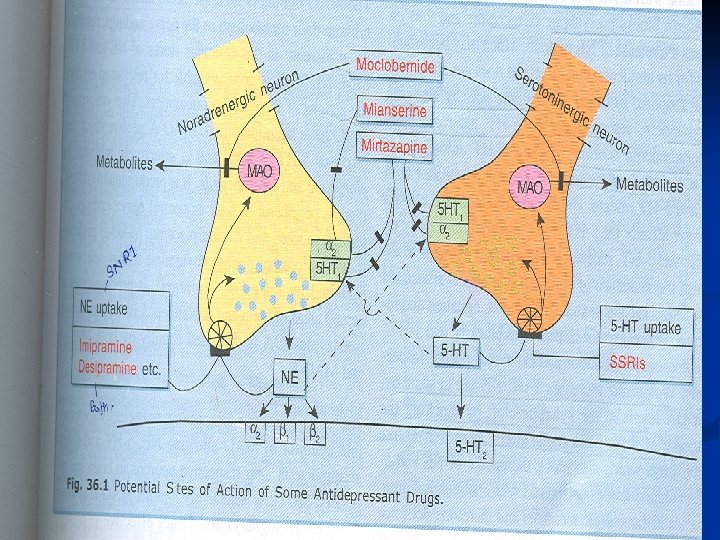
Mechanism of Action 1. Inhibition of MAO enzymes. (MAOIs). 2. Inhibition of NE and 5 -HT reuptake. (TCAs, SSRIs, Newer TCAs). A T Y P I C A L 3. Prominent alpha blocking and weak 5 -HT antagonists. (Nefazodone, trazodone, ) 4. Serotonin and noradrenalin reuptake inhibitor (SNRIs) (venlafaxine, duloxetine) 5. Noradrenergic and specific serotonergic antidepressants (Na. SSA) (Mirtazapine) 6. Inhibitor of Dopamine and Noradrenalin (Bupropion) 7. Blockade of pre-synaptic alpha 2 receptors (Mianserin) 8. Increases rather than inhibiting 5 -HT uptake (Tianeptine, Amineptine)
MAO ( monoamine oxidase) an enzyme Two types n MAO – A n -Peripheral adrenergic nerve endings -Intestinal mucosa -Human placenta -Liver -Serotonin , Noradrenalin and dopamine -Inhibited by MAO-B A-B moclobemide and clorgyline -brain ( basal ganglia) -Platelets -Liver -Deaminates dopamine -Inhibeted by selegiline (deprenyl) C-D Isoniazide, iproniazide, phenelzine, isocarboxazide, tranylcypromine were non selective and irreversible inhibitors (Hit and run drugs) used previously but not used now due to drug and drug food interactions. Linezolide (new drug against MRSA) Cheese and serotonin syndrome
Nonselective MAOIs not favorable Cheese Reaction Cheese, beer, wine, meat, fish, yeast, (contain large amount of tyrammine and other indirectly acting amines) n Hypertensive crises, n CVA Medical Emergency Due to irreversible block of MAO These escape degradation in intestinal wall and liver Reach to circulation Displace large amount of noradrenalin from loaded nerves Tt. I. V. Phentolamine, Prazosin
Nonselective MAOIs not favorable n Cold and Cough medicines contain Ephedrine (Same result as cheese reaction) Levodopa- excitement and hypertension n Tricyclic antidepressants- excitement, rise in BP, temperature n
Reversible inhibitor of MAO-A (RIMAs) n Moclobemiden Reversible and selective MAO-A inhibitor n Short duration of action n Competitive enzyme inhibition n Tyramine is able to displace it n Cheese reaction is less likely n Devoid of anticholenergic, sedative, cognitive, cardiovascular effects
Tricyclic Antidepressants (TCAs) n Imipramine represents the class (Prototype) n Inhibit monoamine reuptake (serotonin and noradrenalin) n Increase the concentration of n Other receptors acted (Adverse effects) n Muscarinic- Anticholinergic side effects (dryness etc. ) # n Alpha- alpha blocking actions (postural hypotension etc. ) # n Histamine-Antihistaminic (sedation) # n Dopamine- antipsychotic (amoxapine, maprotiline) Serotonin and NA at synapse and potentiate the action (therapeutic effects)
TCAs actions (CNS) n In Normal person n - Tiredness Light-headedness Sleepiness Difficulty in thinking Difficulty in concentration, Gait disturbances Provoke anxiety Unpleasant -Sedation immediately -Elevation of mood (24 Weeks) -Suppresses REM prolongs total sleep duration - In Depressed Lower seizure threshold and produce convulsions in overdose Don’t carry abuse potential, Development of dependence is less
TCAs uptake blockade is not directly responsible for antidepressant action? n Uptake blockade occurs quickly but antidepressant action occurs after months n Initially Pre synaptic alpha 2 and 5 -HT 1 auto receptors are activated by increased amount of NA and Serotonin in synaptic cleft resulting in decreased firing n But on long term desensitize and down regulation of these receptors and induce adaptive changes in the number and sensitivity of receptors and amine turnover leading to enhanced NA and Serotonin transmission required for antidepressant action.
TCAs on other systems n ANS Potent anticholinergic (dry mouth, blurring of vision, , constipation, urinary hesitancy) n Weak alpha 1 blocking (postural hypotension, impairment of ejaculation, ) n H 1 antihistaminic (sedation) n n CVS n n n Tachycardia Postural hypotension Cardiac arrhythmias (T wave suppression or inversion) due to intra ventricular conduction interference due to NA and Anti cholinergic actions Tolerance to Anticholinergic and hypotensive actions develop latter on
TCAs (Pharmacokinetics) Good oral absorption n Highly bound to Proteins (plasma and tissue) n Metabolized in liver (oxidation, glucuronide conjugation and CYP 2 D 6, CYP 3 A 4, CYP 1 A 2 n Many active metabolites may be produced n Mostly can be given once a day (at bed) n Have Therapeutic Window phenomenon (50 -200 ng/ml of imipramin) n
TCAs Adverse effects n n n n Anticholinergic- dry moth, bad taste, constipation, epigastric fullness, urinary retention (more common in elderly male), blurred vision, palpitation Sedation, mental confusion, weakness Increased appetite and weight Sweating, fine tremors Precipitation of seizures Postural hypotension Cardiac arrhythmias Rashes and jaundice
TCAs (Acute Poisoning) n n Usually suicidal attempt Presents as n Excitement n delirium, n Anticholinergic symptoms like atropine poisoning n Muscle spasm n Convulsions n Respiratory depression n Coma n Treatment n n n Gastric lavage I. V. line Oxygen Maintenance of BP and Temperature Diazepam iv Propranolol / lignocain
TCAs (Interactions) n n n n n Potentiation of sympathomimetics (direct acting) Reduce action of sympathomimetics (indirect acting) Reduce antihypertensive action of guanethidine and clonidine ( by preventing their transport in to neurons) Potentiate other CNS sedatives SSRIs inhibit metabolism of TCAs With MAO inhibitors dangerous hypertensive crisis with excitement and hallucinations Retard the absorption of other drugs Phenytoin, phenylbutazone, chlorpromazine, aspirin, displace TCAs and produce toxicity Phenobarbitone induce metabolism and inhibit the effect of the drug
Miscellaneous n Amoxapine n Tetra cyclic compound n Blocks D 2 reuptake also n Has mixed antidepressant and neuroleptic effects n Good for psychotic depression n Reboxetine n Selective NA reuptake blocker n Weak action on 5 -HT mechanism n Anticholinergic effects are minimal
Selective Serotonin Reuptake Inhibitors (SSRIs) n Limitations of TCAs n Anticholinergic effects n Alpha blocking action n Cardio toxicity n Sedation, seizures ppt n Low safety margin n Weight gain n Therapeutic window n Overdose poisoning common n Lag of 1 month period n Incomplete response to Tt n Answers may be given by SSRIs n n n n Selectively inhibit membrane associated SERT (serotonin transporter) More tolerability and better acceptability Used in depression as well as in OCD, phobias No sedation, No seizure ppt No alpha blocking action Less chances of arrhythmia No weight gain Now 1 st choice for OCD, Panic disorders, Social Phobia, Eating disorders, Premenstrual syndrome, Post traumatic stress
Important points ØTCAs have slightly more efficacy ØSome patients not responding to TCAs may respond to SSRIs, ØSSRIs preferred in prophylaxis of recurrent depression ØIn severe depression TCAs appear to be more efficacious
Individual compounds n Fluoxetine n n Prototype of SSRIs Longest acting Paroxetine n Short acting n More GI side effects Fluvoxamine n n n Short acting Commonly used in indoor patients Sertraline n Less chances of drug interactions due to low potency to cause cytochrome enzyme depression q. Citalopram q. Escitalopram • Similar to sertraline but should be avoided in patients attempting suicide • Active enantiomer of citalopram side effects are less
SSRIs n Side effects Gastric upset n Nausea n Interfere with ejaculation n Nervousness n Restlessness n Insomnia n Anorexia n Headache n Diarrhea n Epistaxis n Ecchymosis n n Others n n Inhibit cytochrome enzymes and elevate the plasma level of other drugs Other serotonergic drug ( MAOIs) is taken may precipitate Serotonin Syndrome manifesting as agitation, restlessness, sweating, twitching, convulsions
Atypical Antidepressants n Trazodone Blocks 5 -HT uptake n Has prominenent alpha blocking n Weak 5 -HT 2 antagonistic n No anticholinergic effect n Bradycardia n Has anxiolytic action also n Prolonged and painful penile erection n n Mianserin n Unique not inhibit NA and 5 -HT uptake n n Blocks pre-synaptic alpha 2 receptors increases release and turnover of NA Antagonist at serotonin 2, 1 c, and H 1 receptors Has sedative effect Damages liver and bone marrow (Reserve drug)
Atypical Antidepressants n Tianeptine / and Amineptine n Increases rather n n n inhibiting 5 -HT uptake Neither sedative nor stimulant Effective in anxiodepressive states n Venlafaxine / Duloxetine n n Mirtazapine (Na. SSA) n n Noradrenergic and specific serotonergic antidepressant Blocks alpha 2 auto receptor (on NA neuron) and hetero(on 5 -HT neuron) receptors increasing both NA and serotonin release. n SNRI selective in action Faster onset of action Increases BP Duloxetine increases uretheral tone used in urinary incontinence ( over active bladder) Bupropion n n Inhibits DA and NA uptake has excitant effect Used to reduce smoking
Antidepressant uses Depression (ECT may be needed in severely depressed and patients having suicidal tendency) n Bipolar affective disorders TCAs and lithium or SSRIs with lithium or valporate/ lamotrigine n SSRIs with atypical antipsychotic in psychotic depression n Obsessive compulsive disorders (SSRI and Clomipramine) n Eating disorders n
Anxiety disorders n Neuropathic pain n Attention deficit hyperactivity disorder in children n Enuresis- (Imipramine 25 mg at night) n Overactive bladder (stress incontinence) n Migraine prophylaxis n Pruritus (Topical doxepin) n
Antianxiety Drugs n Anxiety - emotional state Unpleasant Associated with uneasiness Discomfort Fear Undefined threat Fear about future Some amount of anxiety is must for progress When it becomes excessive, disproportionate, hampers performance then only needs treatment
Antianxiety Drugs n n n Drugs producing restful state of mind without interfering with normal mental or physical functions. Have no effect on thought control Don’t produce extra pyramidal side effects Can Produce physical dependence May Have abuse potential Don’t selectively block conditioned avoidance response in animals n Have anticonvulsant activity
Antianxiety Drugs n Benzodiazepine n n n Diazepam Chlordiazepoxide Oxazepam Lorazepam Alprazolam n Azapirones n n Others n n PHO/BIG/DOCLA Buspirone Gepirone Ispapirone n Beta blocker- Propranolol Antihistaminics. Hydroxyzine SSRIs and other antidepressant drugs
Benzodiazepines n n n Relieve anxiety at low dose ( higher dose induce sleep and impair performance ) Selective taming effect More selective to limbic system Have low side effects in Antianxiety dose Lorazapam and clonazepam IM for psychotic and manic patients Act by facilitating GABAergic transmission
Benzodiazepine MOA Cl Diazepam + DMCM – Flumazenil- 0 α subunit Extra-tracellular Others δεθπ or t ita cil a F γ subunit tic e m Mi or t a t cili a F Intracellular Barbiturates GABA β subunit GABA- A Receptor Cl More Clintracellular more polarized more
Benzodiazepines n Adverse effects n Sedation n Light headedness n Psychomotor impairment n Cognitive impairment n Vertigo n Confusional state n Increased weight n Impaired sexual functions n Potential to produce dependence n All are almost similar selection is empirical
Benzodiazepines (Individual drugs) n Chlordiazepoxide n n First BZD Long lasting effect Chronic anxiety Diazepam n n Oxazepam n n n Has two phase of metabolism Broken in to active metabolites Long duration of action Lorazepam Polar compound n Less lipid soluble Penetration In brain is slow n Slow entry in brain No active metabolite Used in short lasting anxiety n IM state Alprazolam- high potency, mood elevating in depressed pt. less drowsiness
Buspirone Does not produce sedation, cognitive impairment, n Does not interact with BZD receptor or modify GABAergic transmission n No tolerance n No physical dependence n No muscle relaxant n No anticonvulsant property n
Buspirone Relieves mild to moderate generalized anxiety n Effects develop slowly (not used for acute) n Partial agonist on 5 HT 1 A (pre-synaptic) and antagonist on 5 HT postsynaptic receptors n Presynaptic auto-receptors stimulated leading to reduced activity of dorsal raphe serotonergic neurones n Also has weak D 2 blocking effect n
n Hydroxazine n n n H 1 antihistaminic Sedative, anti -emetic and spasmolytic Anti - Pruritus n Propranolol Reduces sympathetic symptoms like rise in BP, Tremors, sweating etc. n Performance or situational anxiety (like examination fear, social phobia, public lecture) n
Questions Classify antipsychotic drugs n Classify antidepressant drugs n Pharmacological actions of chlorpromazine n Pharmacological actions of amitriptyline n Drug indued parkinsonism n MOA of antipsychotic n MOA of antidepressants n Lithium n
Questions n n n n Drug of choice of cheese reaction-Phentolamine Moclobemide is reversible and selective MAO-A inhibitor All antidepressants don’t inhibit DA uptake except amoxapine, maprotiline, Bupropion Antidepressants don’t carry abuse potential SSRIs are inhibitor of CYP enzymes Serotonin syndrome Trazodone – may produce priaprism due to high α 1 blocking property Mianserin unique not inhibiting NA or 5 HT but blocks Pre-synaptic α 2 receptors Tianeptine, Amineptine - unique increase 5 -HT uptake Venlafaxine, Duloxetine – SNRI Mirtazapine- Na. SSA- blocks α 2 auto and hetro receptors and enhance NA and 5 HT release Nocturnal enuresis- Imipramine Benzodiazepines- GABA facilitatory Buspirone- partial agonist at 5 HT 1 A autoreceptors, antagonist at 5 HT 1 A postsynaptic DOC of performance or situational anxiety- B-blockers
Thanks