Anticoagulants and Thrombolytic Learning objectives At the end

Anticoagulants and Thrombolytic

Learning objectives At the end of session students should be able to: Ø Know the normal hemostatic pathway Ø Know Parenteral anticoagulant drugs Ø Know pharmacokinetics, dynamics of heparin Ø Know the oral anticoagulants Ø Know pharmacokinetics and pharmacodynamics of warfarin

Hemostasis Maintaining fluidity of blood Repairing vascular injury Limiting blood loss Break down of hemostasis lead to Excessive bleeding and thrombosis

Blood Clotting Vascular Phase Platelet Phase Coagulation Phase Fibrinolytic Phase

Vascular Phase Vasoconstriction Exposure to tissues activate Tissue factor and initiate coagulation Tissue Factor
 prevent platelet adhesion and aggregation In vascular")
Platelet phase Blood vessel wall (endothelial cells) prevent platelet adhesion and aggregation In vascular injury, sub endothelial matrix proteins, collagen and von Willebrand factor Platelets contain receptors for fibrinogen and von Willebrand factor After vessel injury Platelets adhere and aggregate Thromboxane A 2 is synthesized from Arachidonic acid ADP released from platelet granules cause platelet aggregation and formation of platelet plug Activation of platelets result in conformational change in the IIb/IIIa receptor, enabling it to bind fibrinogen, which cross link adjacent platelets

Coagulation Phase Two major pathways Intrinsic pathway Extrinsic pathway Both converge at a common point Biosynthesis of these factors are dependent on Vitamin K 1 and K 2 Hereditary lack of clotting factors lead to hemophilia -A

Intrinsic Pathway Extrinsic Pathway Tissue Injury Blood Vessel Injury Tissue Factor XIIa XII Thromboplastin XIa XI IXa IX Xa X Factors affected By Heparin VIIa Prothrombin Vit. K dependent Factors Affected by Oral Anticoagulants Fibrinogen XIII VII X Thrombin Fribrin monomer Fibrin polymer

Classes of Drugs Prevent coagulation Dissolve clots Prevent bleeding and hemorrhage Hemostatic Overcome clotting deficiencies (replacement therapies)

Classification A. Reduce the formation of fibrin clots. 1. INDIRECT THROMBIN INHIBITORS UFH: Heparin LMWH: Enoxaparin, dalteparin, tinzaparin SYNTHETIC: Fondaparinux 2. DIRECT THROMBIN INHIBITORS Parenteral: Hirudin, lepirudin Oral: Ximelagatran, dabigatran 3. ORAL ANTICOAGULANT DRUGS Coumarin anticoagulants ▪ warfarin – dicumarol
 B. Lyse thrombi already formed Streptokinase, Urokinase, Anistreplase Tissue Plasminogen")
ANTICOAGULANT DRUGS (contd. ) B. Lyse thrombi already formed Streptokinase, Urokinase, Anistreplase Tissue Plasminogen Activator: Alteplase, Reteplase, Tenecteplase C. Antiplatelet drugs Aspirin, clopidogrel, ticlopidine Platelet glycoprotein IIa/IIIb Receptor blockers Others: dipyridamole, cilostazol
 It is heterogeneous mixture of sulfated mucopolysaccharides It is glycosaminoglycan found in")
Heparin (Chemistry) It is heterogeneous mixture of sulfated mucopolysaccharides It is glycosaminoglycan found in secretory granules of mast cells, polymer of alternating D-glucronic acid and Nacetyl-D-glucosamine residues These are D-glucosamine-L-iduronic acid and Dglucosamine-D-glucuronic acid
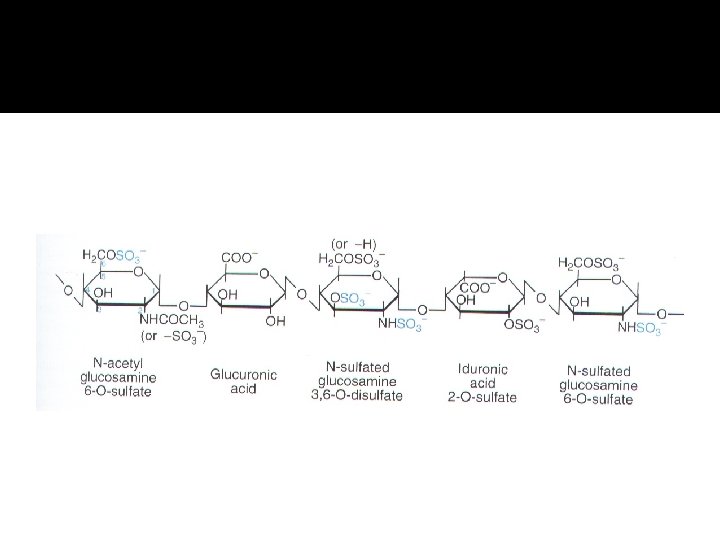

Source: commonly extracted from porcine intestinal mucosa or bovine lung and preparations contain small amount of other glycosaminoglycans.

Pharmacokinetics Not absorbed through GI mucosa Heparin is given as continuous intravenous infusion Immediate onset of action when given intravenously Half life depend on the dose administered Destroyed in liver by heparinase Drug can accumulate in patients with renal impairment I/M can lead to hematoma

Heparin Dose is prescribed in Units Unit of Heparin The USP unit of Heparin is defined as the quantity of Heparin that prevents 1. 0 ml of citrated sheep plasma from clotting for 1 hour after the addition of 0. 2 ml of 1% Calcium chloride (Ca. Cl 2) solution
 MW 5000 -30000 Low MW Forms of Heparin")
Standard Heparin or Unfractioned Heparin (UFH) MW 5000 -30000 Low MW Forms of Heparin preparations (20006000 MW) Enoxaparin Tinzaparin Dalteparin Danaparoid Fondaparinux

Heparin mechanism of action Heparin Antithrombin III Thrombin

Mechanism of Action Heparin binds to endothelial blood surface It activates ant thrombin III It inhibits thrombin IIa , IXa and Xa In the absence of heparin these reactions are slow LMW heparin and fondaparinux have same mechanism of action

Monitoring of Heparin Effect PTT or a PTT Level of UFH determined by protamine titration or anti Xa units Ø Weight based dosing of LMW heparin is important in renal insufficiency, obesity and pregnancy Ø Ø

Clinical uses Initiate treatment of venous thrombosis and pulmonary embolism Inherited and acquired (atrial fibrillation, prolonged bed rest, high risk surgical procedures and cancer) Ø Prevention as well as treatment Ø Oral anticoagulant is started concurrently Ø Heparin is continued for at least 5 days to allow warfarin to achieve full therapeutic effect Ø

LMWHs and Fondaparinux Initial management of unstable angina Acute myocardial infarction Venous thrombosis and pulmonary embolism

Toxicity and adverse effects Bleeding Major bleeding occur in 1 -5% of patients Less bleeding with LMWH Mild bleeding can be controlled without antagonist Protamine sulfate is the antidote (highly basic positively charged peptide, combine with negatively charged heparin 1 mg of protamine neutralize 100 units of heparin Ø

Ø Thrombocytopenia platelet count <150, 000/ml This also occur with LMWH and fondaparinux

Other toxicities Mild elevation of hepatic transaminases Osteoporosis Inhibit the synthesis of aldosterone

Contraindications Hypersensitivity to drug Active bleeding Hemophilia Significant thrombocytopenia Purpura Severe hypertension Intracranial hemorrhage Infective endocarditis Active tuberculosis Ulcerative lesion of GIT

Contraindication --- Threatened abortion Visceral carcinoma Advanced hepatic or renal disease Recent surgery of brain, spinal cord or eye Careful use in pregnancy

Comparison between heparin and LMWH , fondaparinux Features Heparin LMWH Fondaparinux Source Biological Synthetic Molecular weight 15, 000 5000 1500 Target X a and II a Xa Bioavailability % 30 90 100 Half life 1 4 17 Antidote effect Complete Partial None

Features Heparin LMWH Fondaparinux Administration I/V infusion Subcutaneous Monitoring a PTT Adverse effect Thrombocytopenia Osteoporosis Effect on platelet High dose of heparin interfere with platelets aggregation In units Subcutaneous administration Do not require monitoring Less incidence of thrombocytopenia and osteoporosis Little effect on platelets In mg Dose Do not require monitoring Less incidence Little effect on platelets

Direct Thrombin Inhibitor Exert their anticoagulant effect by directly binding to active site of thrombin Hirudin and bivalirudin Agatroban and melagatran
 It inactivate fibrin-bound thrombin in thrombi Monitored")
Parenteral direct thrombin inhibitors Lepirudin (leech saliva) It inactivate fibrin-bound thrombin in thrombi Monitored by a. PTT Clinical use: thrombosis related to heparin induced thrombocytopenia Excreted by kidney Anaphylactic reaction

Oral direct thrombin inhibitor Predictable pharmacokinetics and bioavailability Debigatran etexilate mesylate Debigatran is the active form Clinical use: prevention of stroke and systemic embolism in non valvular atrial fibrillation Prolong PTT and thrombin time

Toxicity Bleeding More in patients >75 No antidote years

Oral anticoagulants WARFARIN Coumarins - warfarin, dicumarol used as rodenticide Administered as sodium salt and has 100% bioavailability Structurally related to vitamin K Delayed onset 8 - 12 hrs

Mechanism of action Block γ-carboxylation of glutamate residues in prothrombin and factor VII, IX and X Proteins C and S Incomplete coagulation factor molecules that are inactive Vitamin k epoxide reductase is inhibited by warfarin

Mechanism of action Descarboxy Prothrombin Reduced Vitamin K Oxidized Vitamin K NADH Warfarin Normally, vitamin K is converted to vitamin K epoxide in the liver. →This epoxide is then reduced by the enzyme epoxide reductase. →The reduced form of vitamin K epoxide is necessary for the synthesis of many coagulation factors (II, VII, IX and X, as well as protein C and protein S). →Warfarin inhibits the enzyme epoxide reductase in the liver, thereby inhibiting coagulation. ( )ﻋﺒﺪﺍﻟﻠﻪ ﺍﻟﻤﻄﻴﺮﻱ

Pharmacokinetics Absorption: complete after oral, I/V or rectal route Distribution: 99 % bound to plasma protein Can reach fetus through placenta Used clinically as racemic mixture S and R warfarin Levorotatory S-warfarin is four times potent

Clinical uses Prevent the progression or recurrence of acute DVT or pulmonary embolism following an initial course of heparin Prevent venous thromboembolism in patients undergoing orthopedic or gyneocological surgery Recurrent coronary ischemia in acute MI patients Systemic embolization in patients with prosthetic heart valves or chronic atrial fibrillation

ADVERSE Effects EFFECTS Bleeding Minor bleeding: withdrawal of the drug and administer vitamin K 1 (PHYTONADIONE) Severe bleeding: fresh frozen plasma or factor IX concentrate Cutaneous necrosis Infarction of fatty tissues, breast, intestine Cross the placenta: Hemorrhagic disorder in the fetus Teratogenic – abnormal bone formation Must not be given to pregnant women.

Monitoring anticoagulant therapy INR Ratio of PT of patient PT of normal person plasma INR = PTpt PT ref

Drug interaction- with Warfarin Category Drugs that Increase Warfarin Activity Mechanism Representative Drugs Decrease binding to Albumin Aspirin, Sulfonamides Inhibit Degradation Cimetidine, Disulfiram Decrease synthesis of Clotting Factors Antibiotics (oral)

Drug interaction with Warfarin Drugs that promote bleeding Inhibition of platelets Aspirin Inhibition of clotting Factors heparin antimetabolites Induction of metabolizing Enzymes Drugs that decrease Promote clotting factor Warfarin activity Synthesis Reduced absorption Hypoproteinemia Barbiturates Phenytoin, rifampin Vitamin K cholestyramine colestipol Nephrotic syndrome

Antiplatelet drugs Example: Aspirin Prevents platelet aggregation /adhesion Clinical use - prevents arterial thrombus Myocardial infarction (MI), stroke, heart valve replacement and shunts Other antiplatelet drugs are - Dipyridamole, sulfinpyrazone and Ticlopidine
 COX is a key enzyme involved in")
Mechanism of action Aspirin inhibits cyclooxygenase (COX) COX is a key enzyme involved in the synthesis of thromboxane 2 (prostaglandins) Inhibits platelet aggregation
 and MI 335")
Prophylactic use of Aspirin Low dose daily. Prevents ischemic attack (ministroke) and MI 335 mg/day reduced the risk of heart attack in patients over 50 More than 1000 mg/day NO EFFECT Contraindication - DO NOT give to patients with glucose 6 -PO 4 dehydrogenase deficiency
 is converted")
Fibrinolysis Enhance degradation of clots Activation of endogenous protease Plasminogen (inactive form) is converted to Plasmin (active form) Plasmin breaks down fibrin clots

Fibrinolysis Exogenously administered drugs Streptokinase - bacterial product ▪ - continuous use - immune reaction Urokinase - human tissue derived – ▪ no immune response Tissue plasminogen activator (t. PA) - genetically cloned ▪ no immune reaction ▪ EXPENSIVE
 Parenteral - 1000 -")
Drug preparations : To reduce clotting Heparin (generic, Liquaemin sodium) Parenteral - 1000 - 40, 000 U/ml Warfarin (generic , Coumadin) Oral : 2 - 20 mg tablets Dipyridamole (Persantine) Oral : 25, 50, 75 mg tablets
 20, 50 mg")
Drug preparations : to lyse clots Alteplase recombinant (t. PA, Activase) 20, 50 mg Lyophilized powder - reconstitute for iv streptokinase (Kabikinase, streptase) Parenteral : 250000 - 1. 5 million units per vial. Lyophilized powder. Reconstitute for iv Urokinase ( Abbokinase) Parenteral : 250000 units per vial. Powder to reconstitute to 5000 u/ml for injection
, Mephyton Oral : 5")
Drug preparations: clotting deficiencies Vitamin K ( Phytonadione (K 1), Mephyton Oral : 5 mg tablets Plasma fractions - for hemophilia Antihemophilic factor ( VIII, AHF) Parenteral Factor IX complex (konyne HT, proplex T) Parenteral : in vials
; Tranexamic acid")
Drug preparations : to stop bleeding Systemic use : aminocaproic acid (Amicar); Tranexamic acid (cyclokapron), Vitamin K Local adsorbable drugs Gelatin sponge (Gelfoam) Gelatin film Oxidized cellulose ( Oxycel) Microfibrillar collagen (Avitene) Thrombin

Anticoagulant drugs to treat thromboembolism Drug Class Anticoagulant Parenteral Prototype Heparin Action Inactivation of clotting Factors Effect Prevent venous Thrombosis Anticoagulant Warfarin Decrease synthesis of Oral Clotting factors Prevent venous Thrombosis Antiplatelet drugs Prevent arterial Thrombosis Aspirin Decrease platelet aggregation Thrombolytic Streptokinase Fibinolysis Drugs Breakdown of thrombi

Intrinsic Pathway All clotting factors are Extrinsic Pathway Initiating factor is outside within the blood vessels - tissue Clotting slower factor Activated partial thromboplastin test (a. PTT) Clotting - faster - in Seconds Prothrombin test (PT)
- Slides: 53