Anti diabetic Drugs BY MD ANAMUL HAQUE M

Anti diabetic Drugs BY MD ANAMUL HAQUE M. Pharm Clinical Pharmacy & Pharmacology

Chapter OUTLINE v INTRODUCTION v BACKGROUND v PREVALENCE v TYPES OF DIABETES v DIAGNOSIS v PATHOPHYSIOLOGY v CAUSES AND MANIFESTATIONS v MAJOR COMPLICATIONS v MANAGEMENT PLAN v PHARMACOTHERAPY ORAL ANTIDIABETIC DRUGS INSULIN

Role of insulin: https: //www. youtube. com/watch? v=OYH 1 deu 7 -4 E Diabetes type 1& 2: https: //www. youtube. com/watch? v=Xfy. Gvxwjl. I&t=105 s Understanding diabetes: https: //www. youtube. com/watch? v=jxbb. Bmbvu 7 I&t=41 s Diabetes: https: //www. youtube. com/watch? v=OXAe 3 e. Ojq. Ck&t=206 s GLUT TYPES: https: //www. youtube. com/watch? v=LW_3 Ji 0 ml. Ec GLUL 4 function: https: //www. youtube. com/watch? v=r 69 MPM 0_5 b. Q Role of exercise: https: //www. youtube. com/watch? v=9 UVl 4 HQ 2 V 1 Q Insulin secretion: https: //www. youtube. com/watch? v=VXQ 0 a. QHe 9 VQ

Diabetes Mellitus Diabetes mellitus is a chronic metabolic disorder caused by inherited or acquired deficiency in production of insulin by the pancreas, or by the ineffectiveness/ underutilization of the produced insulin. Such a deficiency results in increased concentrations of glucose in the blood called hyperglycemia which in turn damage many of the body's systems.

History Diabetes mellitus was recognized as early as 1500 B. C. by Egyptian physicians who described a disease associated with “the passage of much urine” Indian physicians around the same time identified the disease and classified it as madhumeha or "honey urine", noting the urine would attract ants. The term diabetes (the Greek word for siphon) was coined by the Greek physician Aretus. He described patients who were passing too much water (polyuria) – like a siphon. Although it is commonly referred to simply as diabetes, In 1675 Thomas Willis added mellitus to the term. Mel in Latin means honey. The urine and blood of people with diabetes has excess glucose, and glucose is sweet like honey. Diabetes mellitus could literally mean “siphoning off sweet water”.

Worldwide prevalence of diabetes mellitus

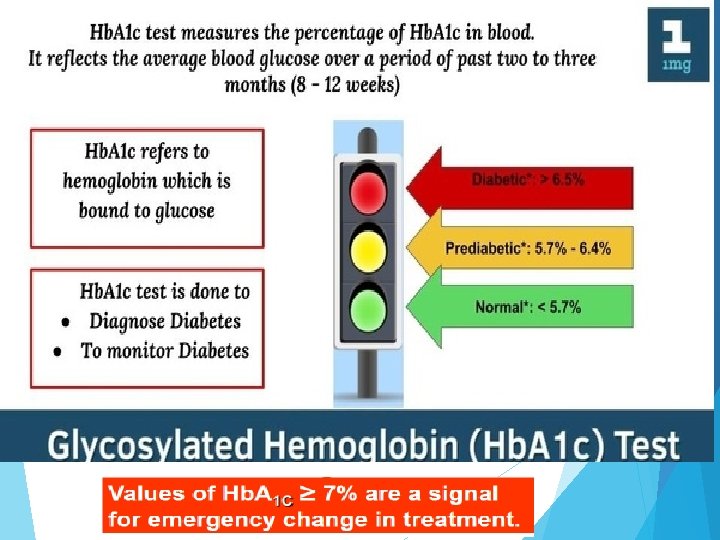
Glucose occupies a central position in metabolism as the predominant substrate for energy production NORMOGLYCEMIA (WHO) Fasting glucose: 3. 8 -6. 1 mmol/L Hb. A 1 C: 4. 7– 6. 0%

Suspected diabetes mellitus Random 2 hours after a meal blood glucose <7. 8 mmol/l Normal 7. 8– 11. 1 mmol/l Impaired Glucose Tolerance (IGT) ≥ 11. 1 mmol/l Diabetes mellitus

Pancreas

Approximately 3 million cell clusters called pancreatic islets are present in the pancreas. Within these islets are four main types of cells which are involved in the regulation of blood glucose levels. Each type of cell secretes a different type of hormone 1. α alpha cells secrete glucagon which increase glucose in blood 2. β beta cells secrete insulin which decrease glucose in blood. 3. δ delta cells secrete somatostatin that regulates α and β cells. 4. γ (gamma) cells, secrete pancreatic polypeptide. As an exocrine gland, it secretes pancreatic juice into the duodenum through the pancreatic duct. digestive enzymes, which break down carbohydrates, proteins, and lipids in ingested food entering the duodenum from the stomach.

Functions of insulin
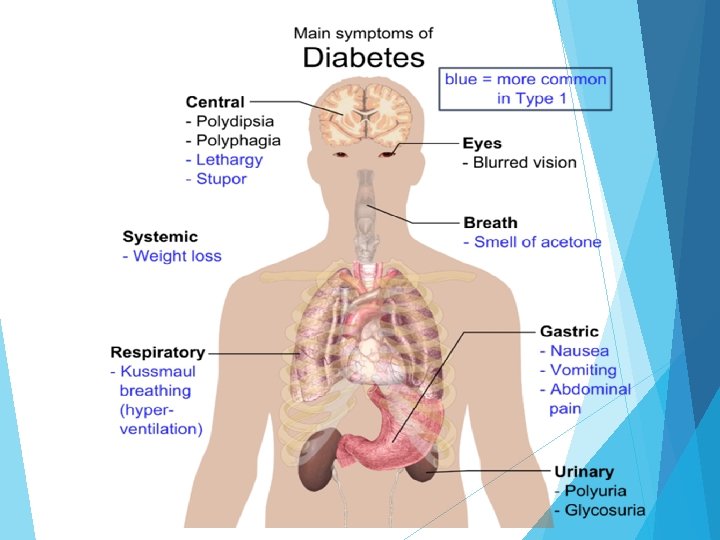

3 main symptoms of diabetes mellitus 1. Polyuria Frequent urination 2. Polydipsia Excessive thirst 3. Polyphagia Excessive eating / hunger
 In this case, there is")
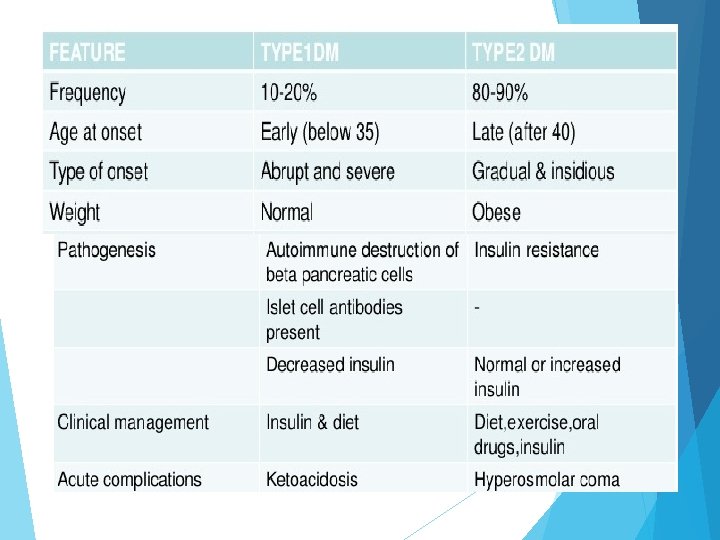
CLASSIFICATION Type I Diabetes mellitus (Insulin Dependent Diabetes Mellitus-IDDM) In this case, there is lack of insulin production which is responsible for metabolism of glucose. β-cell of pancreas is destroyed by an auto immuno process, usually leading to absolute insulin deficiency. It is also called juvenile onset Diabetes mellitus. Over 95% of persons with type 1 diabetes mellitus develop the disease before the age of 25 with an equal incidence in both sexes. Usually, this consists of 10 -15% of all diabetes mellitus patients.
 Type 1 DM (beta-cell destruction) – about 10% of all patients.")
Diabetes mellitus (DM) Type 1 DM (beta-cell destruction) – about 10% of all patients. a) Autoimmune DM ( IDDM or juvenile-onset diabetes). It results from autoimmune mediated destruction of the beta cells of the pancreas. The rate of destructions quite variable (and may reach 80% of the beta- cells of the Langerhans islets), being rapid in some individuals and slow in others. The rapidly progressive form is commonly observed in children, but also may occur in adults. The slowly progressive form generally occurs in adults and is sometimes referred to as latent autoimmune DM in adults (LADA). b) Idiopathic type 1 DM, which has no known etiology of autoimmunity. This form is more common among individuals of African and Asian origin. Patients periodically develop ketoacidosis.
 In this case, insulin concentration")
CLASSIFICATION Type II Diabetes mellitus (Non-Insulin Dependent Diabetes Mellitus-NIDDM) In this case, insulin concentration in blood is sometimes normal or more than normal or less than normal. Insulin is produced in β-cell but not secreted sufficiently or not working due to tissue resistance to insulin. There may be decrease in insulin receptors. Glucose is not utilized properly. This is also called maturity onset Diabetes mellitus or old age Diabetes mellitus. Usually, it consists of 85% of all patients.

CLASSIFICATION Type III Diabetes mellitus It is called secondary Diabetes mellitus. It is a non-pancreatic Diabetes mellitus characterized by elevation of blood glucose level by some drugs such as corticosteroids, phenytoin, thiazides etc. Type IV Diabetes mellitus (Gestational Diabetes mellitus) It is usually found in pregnant woman. In case of pregnancy, some hormones of placenta are responsible for insulin resistance In case of diabetes insipidus, there is no increase of blood sugar (hyperglycemia). It is the feeling of extreme thirst and excessive urine is produced due to less ADH (Anti-diuretic hormone) secretion. Decreased secretion of ADH (Anti-diuretic hormone) vasopressin causes extreme production of urine.
. It")
Diabetes insipidus, in this case there is no increase of blood sugar (hyperglycemia). It is the feeling of extreme thirst and excessive urine is produced due to Decreased secretion of ADH (Anti-diuretic hormone) vasopressin. A hormone called anti-diuretic hormone (ADH), or vasopressin, helps control how fast or slow fluids are excreted. ADH is made in a part of the brain called the hypothalamus and stored in the pituitary gland, a small gland found in the base of the brain. Causes: neurogenic diabetes medlineplus. gov/ency/article/000704. htm in insipidus or near : the pituitary gland/Hypothalamus, autoimmune disorder. nephrogenic diabetes insipidus: Hpercalcemia, Polycystic kidney diseases.

Causes / Etiology of Diabetes mellitus: Causes of Type I Diabetes mellitus Production of autoimmune response causing destruction of β-cell. Infection with virus causing destruction of β-cell. [Encephalomyocarditis virus, Mengovirus, Coxsackie B virus, Reovirus ] Exposure to diabetogenic chemicals (streptozotocin, chlorozotocin, cyproheptadine, alloxan) Drug induced damage of β-cell [Pentamidine, SSRI] Certain disease [Cystic fibrosis, Chronic Pancreatitis] Exposure of young infants to cow’s milk. Causes of Type II Diabetes mellitus Physical inactivity Obesity Heredity Insulin receptor defects Reduction of sensitivity of peripheral tissue.

Causes / Etiology of Diabetes mellitus: Causes of Type III Diabetes mellitus It is called secondary Diabetes mellitus. It is a non-pancreatic Diabetes mellitus characterized by elevation of blood glucose level by some drugs such as corticosteroids, phenytoin, thiazides etc. Some endocrine disorder. Causes of Type IV Diabetes mellitus Increased insulin resistance due to placental hormone in pregnancy. Typically women’s insulin demand may be 2 -3 times higher during pregnancy than normal. A number of hormones needed to promote the growth of fetus (specially human placental lactogen and progesterone), have an opposite action to insulin. During pregnancy, the placenta, which connects your baby to your blood supply, produces high levels of various other hormones. Almost all of them impair the action of insulin in your cells, raising your blood sugar. Modest elevation of blood sugar after meals is normal during pregnancy.

Glucose cannot enter our cells without insulin being present – insulin makes it possible for our cells to take in the glucose. Why does a patient with diabetes lose weight? Diabetes and sudden weight loss. In people with diabetes, insufficient insulin prevents the body from getting glucose from the blood into the body's cells to use as energy. When this occurs, the body starts burning fat and muscle for energy, causing a reduction in overall body weight. Slow healing in Diabetic patient? Diabetes and slow healing wounds. High levels of blood glucose caused by diabetes can, over time, affect the nerves (neuropathy) and lead to poor blood circulation, making it hard for blood - needed for skin repair - to reach areas of the body affected by sores or wounds. An elevated blood sugar level decreases the function of red blood cells that carry nutrients to the tissue. Without sufficient nutrients and oxygen, a wound heals slowly. Diabetic Neuropathy. When blood glucose levels are uncontrolled, nerves in the body are affected and patients can develop a loss of sensation.
 Micro-vascular")
The chronic complications of diabetes include- Macro-vascular disease (peripheral, cerebral, cardiovascular disease) Micro-vascular disease (retinopathy and nephropathy) Neuropathy (peripheral and autonomic) Foot problems

Description Body location Eyes Retinopathy, Glaucoma, cataract formation and visual disturbance Mouth Gingivitis (inflammation & swelling of the gum), increased incidence of dental cavity Reproductive Increased incidence of large babies, system Miscarriages (Pregnancy) Neonatal death and congenital defects Still birth, Nervous system Motor, sensory and autonomic neuropathy leading to impotence (inability to take effective action), gangrene Vascular system Large vessel disease and microangiopathy Skin Numerous infections and specific lesions due to small vessel disease Kidney Diabetic glomerulosclerosis causing nephropathy Others Tuberculosis, stroke and cardiovascular diseases

Causes of Complications of Diabetes mellitus Most salient in this list of deleterious biochemical pathways is the production of high conc. Of advanced glycation end products (AGE’s) and sorbitol. 1. AGE’s: Glycated proteins Advanced Glycated End products (AGEs) Thickening of membranes Reduction of EDRF (Endothelial Derived Relaxing factor) Vasoconstriction Atherosclerosis Hypertension Stroke and Heart diseases

Ø Proteins throughout the body are non-enzymatically glycosylated at a rate that is proportional to the ambient glucose concentration. Ø These glycosylated proteins are highly reactive, forming bonds with other glycosylated proteins, collagen and other molecules eventually forming AGE’s. Ø AGE’s are very stable and are incorporated into the basement membrane matrix of capillaries. Ø This process causes the thickening of the basement membranes and reduction of active endothelial derived relaxing factor (EDRF). Ø The net result is leakage across the basement membranes, which appears as hard exudates in the patient with diabetic retinopathy and as proteinuria in the patient with diabetic nephropathy. Ø This process is thought to be one of the major pathways leading to the development of macro vascular disease.

2. Sorbitol/polyol Pathway: Another important biochemical pathway leading to the development of chronic complications in patients with diabetes is the sorbitol pathway.

Many cell lines, such as the Schwann cell in the CNS, do not require insulin for uptake of glucose. These cell types will be subject to intracellular hyperglycemia during times of ambient hyperglycemia. As a result a high fraction of glucose is shunted into the sorbitol pathway leading to the formation of high concentrations of sorbitol via the enzyme aldose reductase. High concentrations of sorbitol cause a reduction in the uptake of myoinositol results in the down regulation of Na+/K+ ATPase system with a reduction in energy production. Additionally, sorbitol cause an intracellular osmotic gradient resulting in hypervolemia of the cell. This pathway is thought to be important in the development of neuropathy in diabetic patients.
 are proteins or lipids that become glycated as a")
Advanced glycation end products (AGEs) are proteins or lipids that become glycated as a result of exposure to sugars. They can be a factor in aging and in the development or worsening of many degenerative diseases, such as diabetes, atherosclerosis, chronic kidney disease. Glycation is the result of the covalent bonding of a sugar molecule, such as glucose or fructose, to a protein or lipid molecule, without the controlling action of an enzyme.
 – a condition brought on by inadequate insulin –")
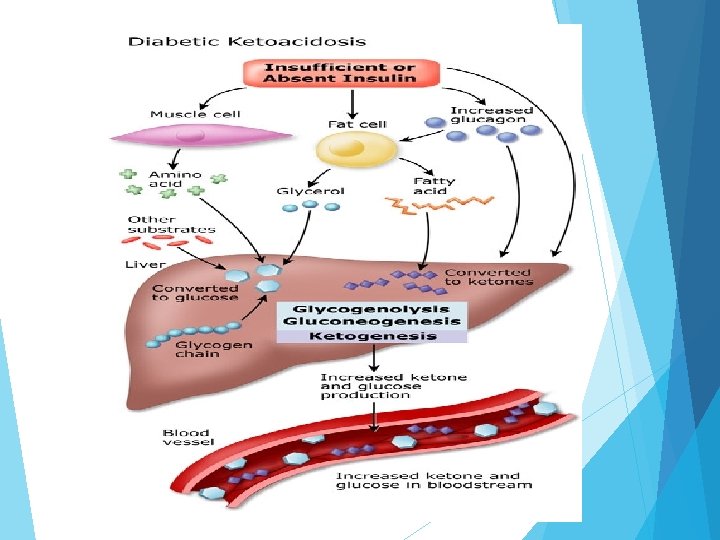
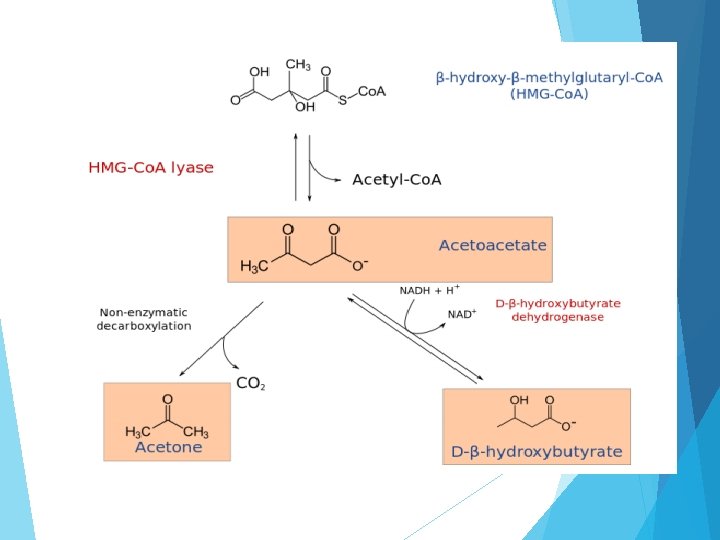
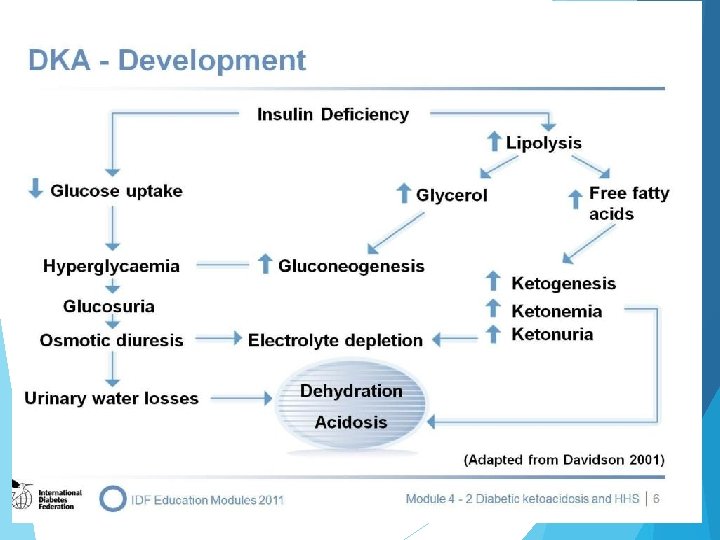
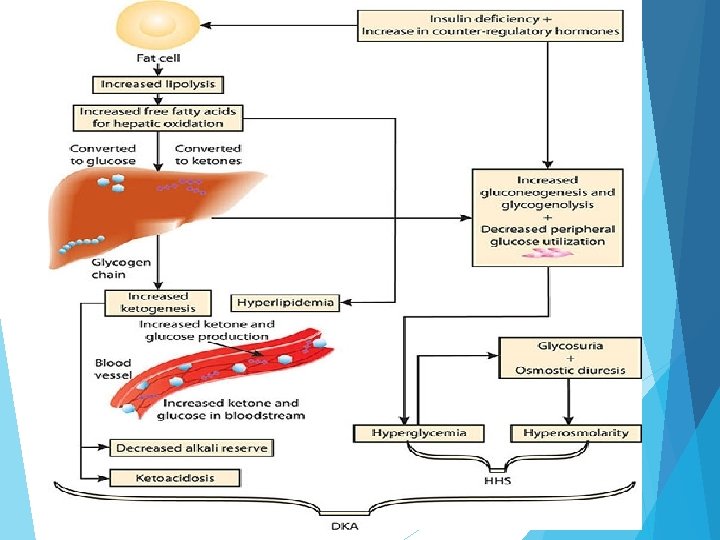
Diabetic ketoacidosis Diabetic Ketoacidosis (DKA) – a condition brought on by inadequate insulin – is a life-threatening emergency usually affecting people with type 1 diabetes. Although less common, it also can happen when you have type 2 diabetes. The important fact to remember is that without enough insulin, the body cannot burn glucose properly and fat comes out of fat cells. As a consequence the excess fat goes to the liver and glucose builds up in the bloodstream. The liver makes ketoacids (also known as ketones) out of the fat. Before long, the body is literally poisoning itself with excess glucose and ketoacids. Life-threatening complication occurs with insulin deficiency Glucose cannot be used by body cells for energy so fat is mobilized for this purpose Mobilized fat is then extracted by liver and broken down into glycerol and fatty acids Fatty acids further broken down into ketones
 Nausea and vomiting Thirst Polydipsia,")
Clinical S/S of DKA Kussmaul breathing ( Laboured Breathing) Nausea and vomiting Thirst Polydipsia, polyphagia and polyuria Hypotension Tachycardia shock DKA/HHS Management IV fluids to rehydrate No use of hypotonic solutions at this time Potassium supplementation IV insulin drip with gradual lowering of blood sugars Judicious administration of sodium bicarbonate
")
Hyperglycemic Hyperosmolar Syndrome(HHS)

Management goals • Normoglycemia - avoiding hypoglycemia or ketosis - Hb. A 1 C < 6. 5% (glycosylated hemoglobin) glycosylated hemoglobin • Reduce - nephropathy - neuropathy - retinopathy - infections (mycoses, etc)
 • Diet – weight control BMI –")
• Control blood pressure (120/80 mm) • Diet – weight control BMI – low fat intake 18. 5– 24. 9 – normal protein intake – carbohydrates ~ 50% of total energy • Motor activity and compliance! !

Management of Diabetes Mellitus Education Diabetic patients should be monitored under the guideline of a good professional health team including a physician, a pharmacist, and a nurse and so on). Patients should be continually educated and participate with other patients with diabetes. Exercise produces insulin sensitivity which will be effective for glucose utilization. It helps in uptake of glucose by muscle. It also increases blood circulation which will increase glucose utilization.

Management of Diabetes Mellitus Diet Diabetic patients should follow dietary requirement. Prolong fasting should be avoided. Quick acting sugar should be avoided. Animal fat should be avoided Alcohol and smoking should be prohibited. Medications The medications that are used for the treatment of diabetes can be catergorized into two broad areas Insulin Oral antidiabetic agents.

Hypoglycemic Drugs Insulin: it lowers glucose levels by increasing glucose uptake by cells Indicated for Type 1 DM, often in Type 2 DM, in those with chronic pancreatitis. Oral Anti diabetic Drugs


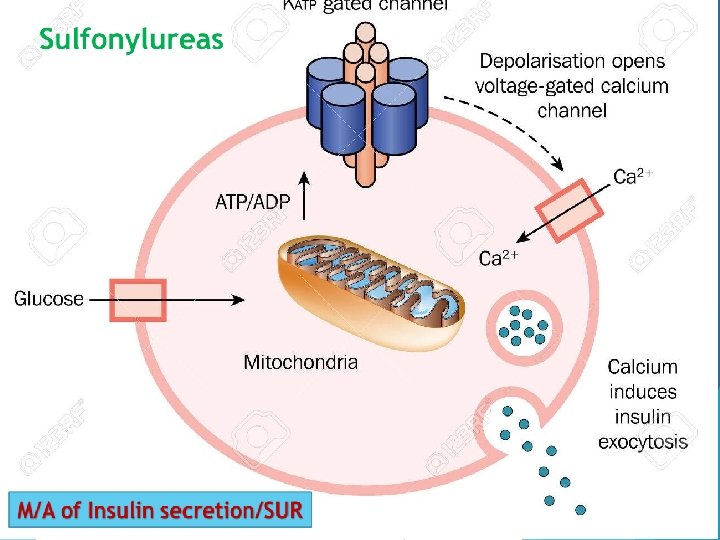
M/A of Insulin secretion

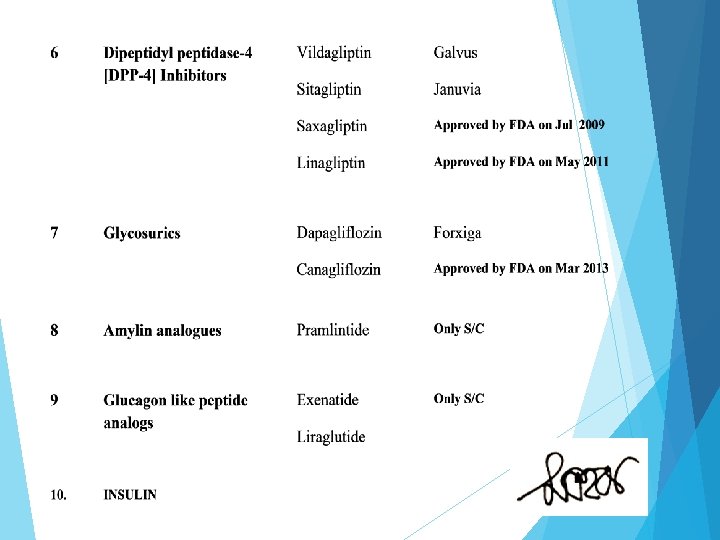
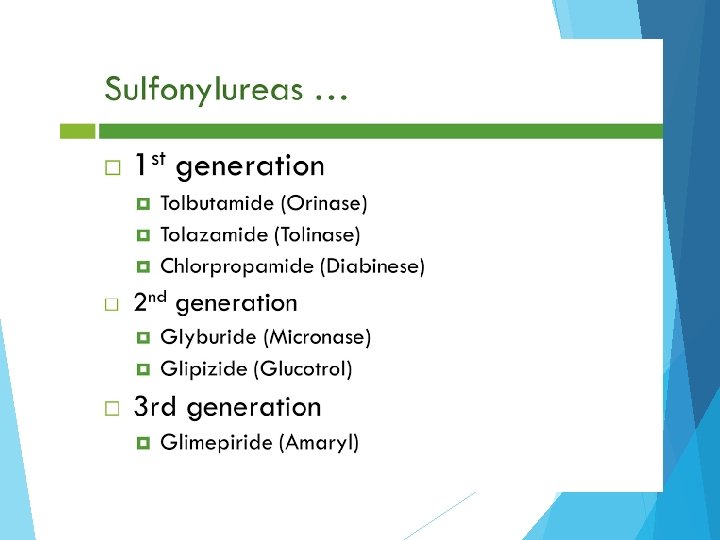
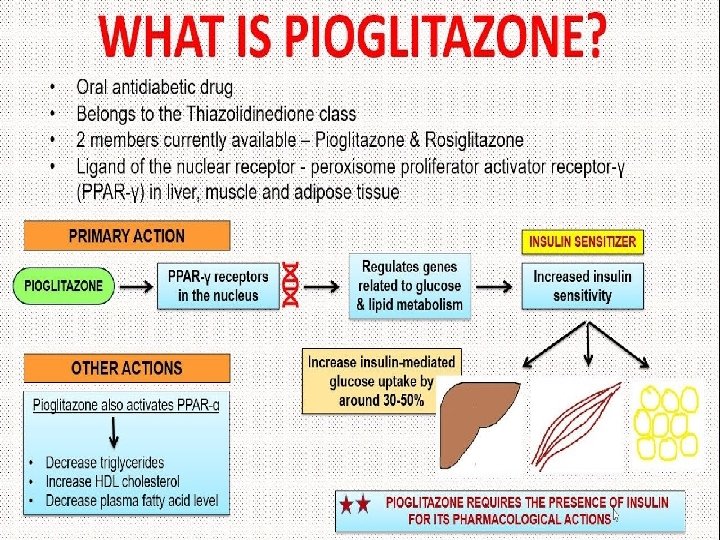
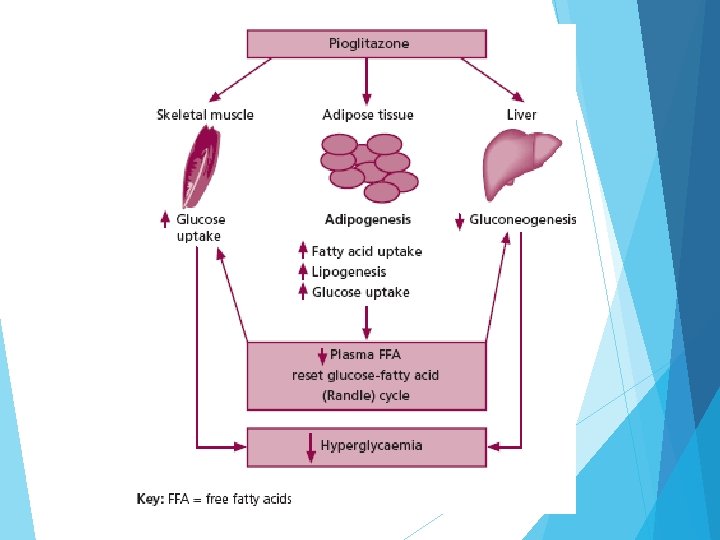
Oral Antidiabetic Drugs Classification of Oral Antidiabetic Drugs A. Insulin secretagogues (agents that increase insulin secretion from pancreas) 1. Sulfonylureas: First generation: Tolazamide, Tolbutamide, Chlorpropamide; Second generation: Glyburide, Glipizide, Glimepiride, Gliclazide 2. Meglitinides: Repaglinide 3. D-Phenylalanine derivatives: Nateglinide B. Biguanides: Phenformin, Metformin. C. Thiazolidinediones: Pioglitazone, Rosiglitazone. D. α- glucosidase inhibitors: Acarbose, miglitol. E. Dipeptidyl peptidase-4 [DPP-4] Inhibitors: Vildagliptin, Sitagliptin, Saxagliptin, Linagliptin F. Glycosurics: Dapagliflozin, Canagliflozin G. (GLP-1) agonists : Liraglutid, Liraglutid Exenatide

Meglitinide derivatives They are insulin secretagogues. They enhance insulin secretion from β-cells of pancreas. M/A is similar to that of sulfonylureas. Repaglinide Newer class of drug used clinically in 1998. Use: Action of Repaglinide is quick. It can be used in post-prandial (meal time) hyperglycemia. So the drug is taken before meal. Advantage: It will not cause sulfur toxicity (Sulfonylureas contain sulfur in their structure. So, they cause sulfur toxicity). Adverse effects: Headache, dyspepsia, weight gain, arthralgia.

D-Phenylalanine derivatives They are also insulin secretagogues. M/A: M/A is similar to that of sulfonylureas. Nateglinide It is a newer drug developed after rapeglinide. It is the meglitinide and phenylalanine derivative. It is absorbed quickly within 20 minutes and peak plasma concentration reaches less than 1 hour. Use: It is used for post-prandial hyperglycemia. It is also used in combination with other drugs which have effects on overnight hyperglycemia. Adverse effects: Nausea, dizziness, vomiting, joint pain, flu-like symptom.

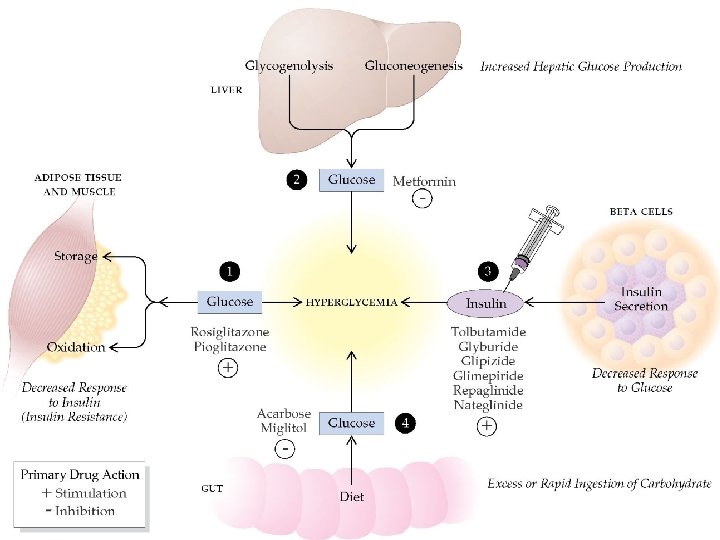
Biguanides Phenformin: It is a toxic drug and also an older drug. It causes lactic acidosis. So, it discontinued and replaced by metformin. Metformin M/A: It has no effect on β-cells of pancreas. It enhances the utilization of glucose. No action on receptors. It acts in the following ways: It suppresses the hepatic gluconeogenesis and glucose output from liver. It enhances disposal of glucose in muscle and fat. Usually, it enhances GLUT-4 concentration from intracellular region to plasma membrane. It reduces the absorption of glucose from intestine and decreases the blood sugar level. It increases the utilization of glucose in peripheral tissue by anaerobic glycolysis. Adverse effects: Diarrhea, drowsiness, weakness, dizziness, malaise and headache.
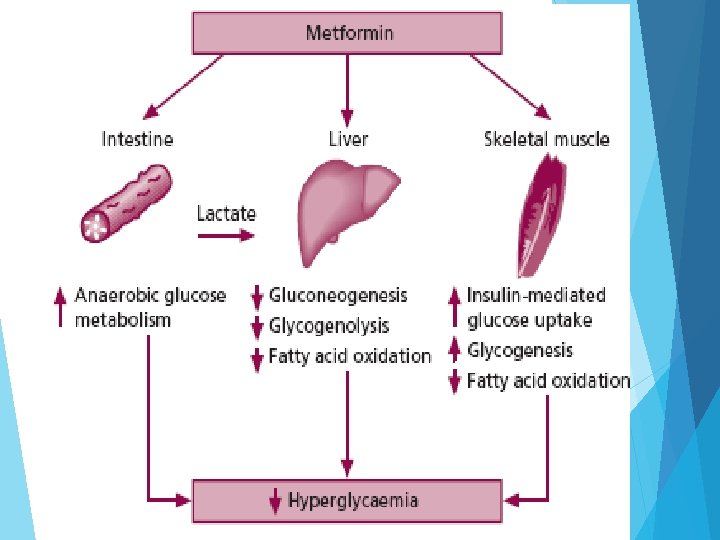

Main Use: 1. Metformin Treats and Prevents Type 2 Diabetes 2. Metformin Improves Insulin Resistance Other Recent uses: 1) Metformin Treats Symptoms of PCOS (Polycystic ovarian syndrome) 2) Metformin Causes Weight Loss Adverse effects: Diarrhea, drowsiness, weakness, dizziness, malaise and headache. Caution: Acute renal failure, CHF, Age >80 yrs due to lactic acidosis. GFR less than 45 ml/min.

Alpha-glucosidase inhibitors Acarbose, Miglitol They work by preventing the digestion of carbohydrates that are normally converted into simple sugars (monosaccharides) by alpha-glucosidase enzymes present on cells lining the intestine. Hence, alpha-glucosidase inhibitors reduce the impact of dietary carbohydrates on blood sugar. Inhibition of these enzyme systems reduces the rate of digestion of carbohydrates. Less glucose is absorbed because the carbohydrates are not broken down into glucose molecules. Acarbose (Precose) and miglitol (Glyset) inhibit alpha-glucosidase enzymes (maltase, amylase, sucrase) in GI tract. Delays absorption of complex CHO and simple sugars

Alpha-glucosidase inhibitors: e. g: Acarbose, Voglibose and Miglitol Acarbose…

https: //www. youtube. com/watch? v=3 -z 3 Gf 8 Sua. E

Dipeptidyl peptidase-4 inhibitors Vildagliptin, Sitagliptin, Saxagliptin, Linagliptin

https: //www. youtube. com/watch? v=e. YYw. Op. G 15 IE https: //www. youtube. com/watch? v=Fe. Pj. KBo. FICA
 and glucose-dependent gastric inhibitory polypeptide(GIP)")
During a meal, the incretins glucagon-like peptide 1 (GLP-1) and glucose-dependent gastric inhibitory polypeptide(GIP) are released by the small intestine into the blood stream. It stimulates insulin biosynthesis, inhibits glucagon secretion, slows gastric emptying, reduces appetite and stimulates regeneration of islet β-cells. ) GLP-1 and GIP have extremely short plasma half-lives due to very rapid inactivation, catalyzed by the enzyme DPP-4. Inhibition of DPP-4 slows their inactivation, thereby potentiating their action, leading to lower plasma glucose levels, hence its utility in the treatment of type 2 diabetes.
 agonists Liraglutid, Liraglutid Exenatide Binds to the same receptors as does")
Glucagon-like peptide-1 (GLP-1) agonists Liraglutid, Liraglutid Exenatide Binds to the same receptors as does the endogenous metabolic hormone GLP-1 that stimulates insulin secretion. It acts in a glucose-dependent manner, meaning it will stimulate insulin secretion only when blood glucose levels are higher than normal, preventing "overshoot". Consequently, it shows negligible risk of hypoglycemia.
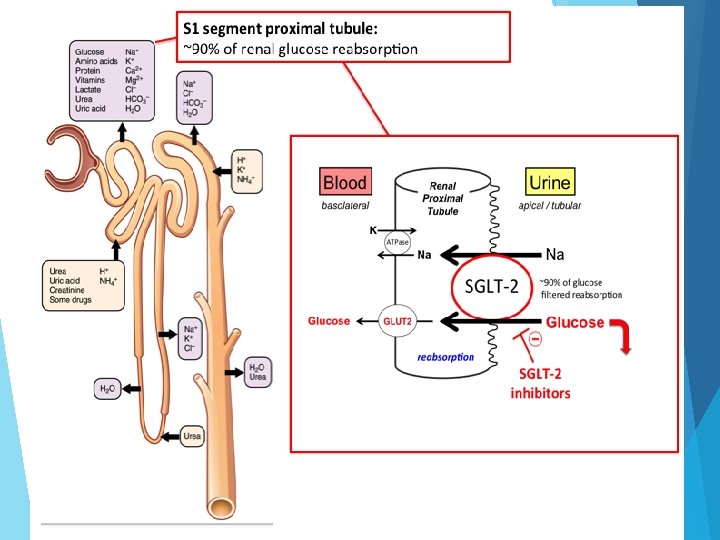
/Glycosurics: Dapagliflozin, Canagliflozin • Canagliflozin blocks in")
Inhibitors of reabsorption of glucose (SGLT 2 inhibitors)/Glycosurics: Dapagliflozin, Canagliflozin • Canagliflozin blocks in renal proximal tubule sodium / glucose co-transporter protein 2 (SGLT 2), which re-absorbed 90% of the filtrated glucose. The result is increased glucosuria and plasma glucose levels are lowered.

Thiazolidinedione derivatives Side effects: Edema, cardiovascular disease. weight gain, hepatic dysfunction, anemia,
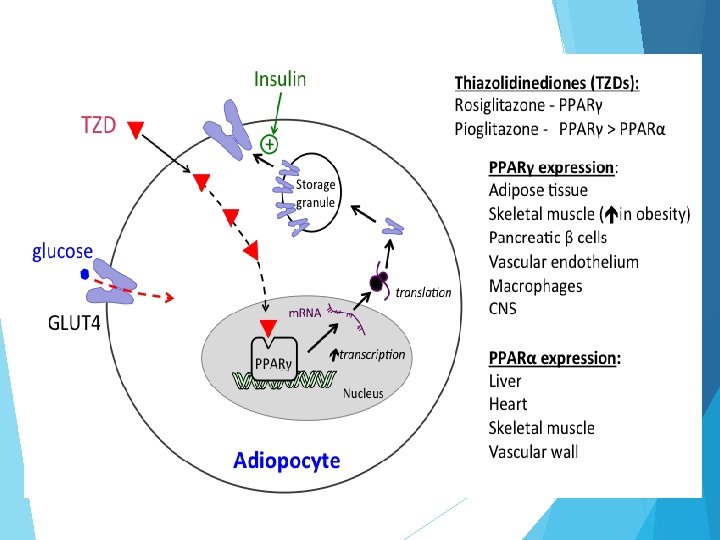
 increase tissue insulin sensitivity but have serious ADRs and suspended from the")
Thiazolidinediones (TZDs) increase tissue insulin sensitivity but have serious ADRs and suspended from the EU market: market - Rosiglitazone (Avandia ) has high cardiovascular risks - Pioglitazone causes bladder tumors Troglitazone causes hepatitis

AMYLIN ANALOGUE

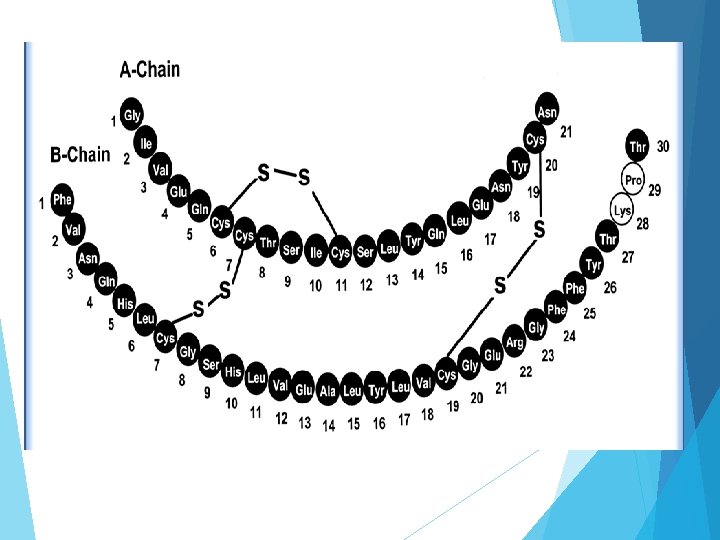
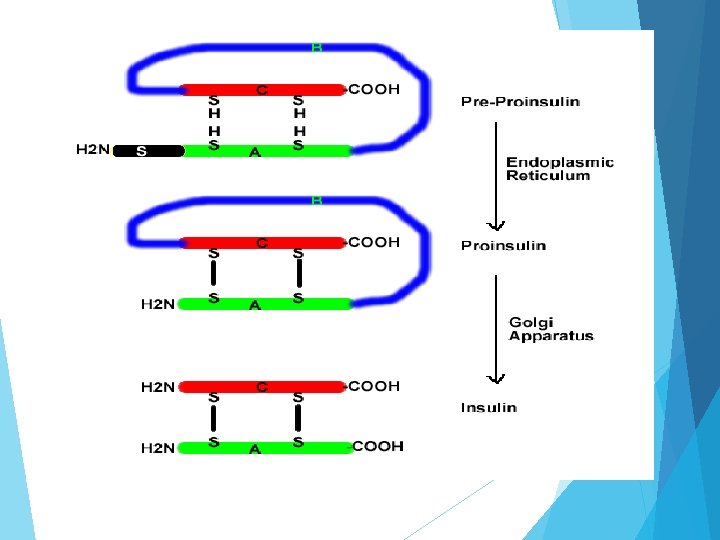
Insulin It is a dimer of an A-chain and a B-chain. Insulin's structure varies slightly between species of animals. It is composed of 51 amino acids arranged in two chains (A and B) linked by two disulfide bridges. Chain A consists of 21 amino acids whereas chain B consists of 30 amino acids. These two chains are connected by disulfide linkage. First bridge occurs between cysteine of position 7 th in both chain. Second chain between cysteine at 20 th position of chain A and cysteine at 19 th position of chain B. Chain A contains one intra subunit disulfide bridge between cysteine molecule at position 6 th and 11 th. Insulin cannot be given orally because it is a peptide hormone. If it is given orally, it will be hydrolyzed by proteolytic enzymes present in stomach. Thus it is administered subcutaneously. Type II diabetic patients sometimes require insulin.

Hypoglycemia It is a clinical condition associated with low blood sugar level. If blood sugar falls around 50 mg/dl then hypoglycemia occurs. Symptoms: Normal symptoms include • Nausea • Weakness • Palpitation • Sweating • Nervousness • Intense hunger Hypoglycemic episode: If blood sugar falls below 45 mg/dl, then acute symptoms are shown and this is called hypoglycemic episode. In that case nervous system is affected and symptoms include. Diminished cerebral function (confusion, agitation, lethargy or personality changes) Drowsiness Unconsciousness Convulsion Coma Speaking problem

Causes of hypoglycemia: �Insufficient food intake due to skipping meals, vomiting or diarrhea �Excessive exercise �Inaccurate measurement of insulin �Concomitant intake of hypoglycemic drugs (Sulfonyl urea) �Termination of diabetogenic conditions �Strict glycemic control �Liver diseases �Hypopituitarism, adrenocortical insufficiency Treatment: All manifestations of hypoglycemia are relieved rapidly by glucose administration. Patients should instantly take quick acting sugars [such as table sugar (pure sucrose derived from sugar beet or sugar cane), soda, juice]. 3 tea spoon (1 tea spoon = 4. 92892 ml), 10 -15 mg of sugar is given at a time and may repeat for 3 times if condition does not improve.
- Slides: 80