ANTHRAX Dr Ammar Ibne Anwar Sub Tahaffuzi wa

ANTHRAX ﻣﺮﺽ ﺍﻟﺠﻤﺮﺓ Dr. Ammar Ibne Anwar Sub: Tahaffuzi wa Samaji Tib D/O Tahaffuzi wa Samaji Tib , F/O Unani Medicine Aligarh Muslim University.

Introduction ü Malignant pustule, Malignant oedema, Woolsorter disease, Ragpicker disease. ü From the Greek word anthrakos for coal or black. ü Primarily a disease of domestic & wild animals Herbivores such as sheep, cows, horses and goats. ü Anthrax zones is a soil rich in organic matter (p. H < 6. 0)
, S. E. Asia, China, South America,")
Epidemiology Distribution worldwide Common in Africa ( Zimbabwe), S. E. Asia, China, South America, Turkey, Pakistan, India Human to human or animal to animal transmission is rare (not contagious) Grazing animals become infected through ingestion of spores in the soil (Carcasses become the source)

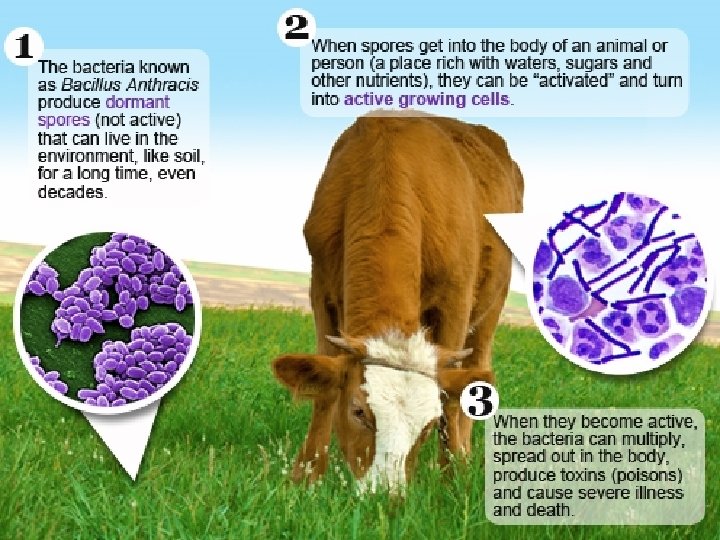
Causative organism Etiological agent: Bacillus anthracis Cohn 1875. Bacillus Anthracis A large, aerobic, spore-forming, gram positive rod-shaped microorganism that is capsulated and non-motile. This microorganism grows in chain. Like many other members of the genus Bacillus, Bacillus anthracis can form dormant endospores often referred to as spores that are able to survive in harsh conditions for decades or even centuries. Such spores can be found on all continents, even Antarctica. When spores are inhaled, ingested, or come into contact with a skin lesion on a host, they may become reactivated and multiply rapidly.
")
Incubation Period üCutaneous anthrax occurs 1 to 7 days (usually 2 to 5 days) after spores enter the body through breaks in the skin. üInhalational anthrax occurs 2 to 7 days (but sometimes up to 2 months) after inhaling large amounts of anthrax spores üGastrointestinal anthrax occurs 2 to 5 days after swallowing spores.

Transmission

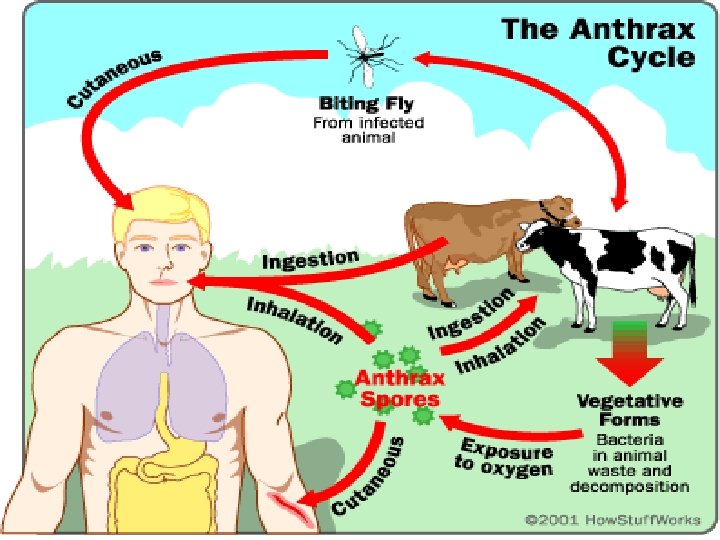
v Direct transmission Through cutaneous contact with infected animals or contaminated animal products. v Indirect transmission Through ingestion of contaminated meat. v Airborne transmission Through inhalation of air contaminated by spores.
 dying")
Transmission Contact with tissues of animals (cattle, sheep, goats, horses, pigs and others) dying of the disease. Biting flies that have partially fed on such animals. Contact with contaminated hair, wool, hides or products made from them (e. g. drums, brushes, rugs). Contact with soil associated with infected animals or with contaminated bone meal used in gardening.

Transmission contd. Inhalation anthrax results from inhalation of spores in risky industrial processes such as tanning hides and processing wool or bone with aerosols of B. anthracis spores in an enclosed, poorlyventilated area. Intestinal and oropharyngeal anthrax may arise from ingestion of contaminated undercooked meat. Accidental infections may occur among laboratory workers. Anthrax is NOT transmitted person to person.

Clinical manifestations

Clinical manifestations Anthrax is an illness with acute onset. Characterised by several distinct clinical forms including: • Skin lesion • Respiratory illness • Abdominal distress Ninety percent of cases are cutaneous anthrax

Cutaneous Anthrax üMainly in professionals (Veterinarian, butcher, Zookeeper. üSpores infect skin a characteristic gelatinous edema develops at the site (Papule- Vesicle. Malignant Pustule- Necrotic ulcer) ü 80 -90% heal spontaneously ( 2 -6 wks) ü 0 -20% progressive disease develop septicemia. ü 95 -99% of all human anthrax occur as cutaneous anthrax.

Cutaneous Anthrax contd. . Cutaneous anthrax is typically caused when Bacillus anthracis spores enter through cuts on the skin. Lesions usually occur on exposed skin and often commence with itchiness. Symptoms include muscle aches and pain, headache, fever, nausea, and vomiting.

They pass through several stages: 1. Papular stage 2. Vesicular stage with a blister that often becomes hemorrhagic 3. Eschar stage that appears two to six days after the haemorrhagic vesicle dries to become a depressed black scab (malignant pustule) which may have surrounding redness and extensive edema (swelling). Anthrax lesions are usually painless but pain may result due to surrounding edema. Untreated lesions can progress to involve regional lymph nodes. An overwhelming septicaemia can occur in severe cases.


Intestinal Anthrax ü ü ü Due to in ingestion of infected carcasses. Mucosal lesion to the lymphatic system. Rare in developed countries. Extremely high mortality rate. Nausea, anorexia, vomiting, fever Progresses to severe abdominal pain and bloody emesis and diarrhoea. ü Ascites may develop on day 2 - 4 ü Death 2 to 5 days after onset of symptoms.
 üPresent with symptoms of")
PULMONARY ANTHRAX üAcquired through inhalation of spores (Bioterrorism - aerosol) üPresent with symptoms of severe respiratory infection( High fever & Chest pain). üProgress to septicemia very rapidly. üMortality rate is very high > 95%. Chest X-ray showing widened chest cavity inhalation anthrax

PULMONARY ANTHRAX Contd. . ØAlso known as Woolsorter’s disease ØResults from breathing anthrax spores into the lungs. ØEarliest symptoms resemble those of a respiratory infection such as mild fever and sore throat. ØAfter one to three days of acute phase, increasing fever, dyspnoea, hypoxia, and hypertension occur usually leading to death within 24 hours.

Anthrax Meningitis Usually a complication of anthrax septicemia. Subarachnoid haemorrhage is a common feature Very often fatal

Diagnosis Clinical sign and symptoms. Laboratory confirmation requires at least one of the following: 1. Isolation of Bacillus anthracis from a clinical specimen. • demonstration of B. anthracis in a clinical specimen by immunofluorescence. 1. Significant antibody titres developing in an appropriate clinical case.

Treatment v Penicillin is the drug of choice for cutaneous anthrax and is given for 5– 7 days. v Tetracyclines, erythromycin and chloramphenicol are also effective. v If the case is associated with a bio-terrorist attack involving aerosolised anthrax where the risk is high, ciprofloxacin or doxycycline are recommended and should be given for at least 60 days

Vaccination Cell-free filtrate At risk groups Veterinarians Lab workers Livestock handlers Military personnel Immunization series Five IM injections over 18 -week period Annual booster

Prevention & Control ü Sterilize hair, wool or hides, bone meal or other feed of animal origin prior to processing. ü Avoid working with raw animal hides, fur or skin, especially those of goats, sheep, or cows. ü Do not eat meat that has not been properly slaughtered and cooked. ü Immunization of high risk individuals usually laboratory workers who are liable to handle B. anthracis.

ü Spores will NOT form inside the carcass, and putrefaction kills the Bacillus. Flies incoagulable blood may be a problem. feeding on ü Protective, impermeable clothing and equipment such as rubber gloves, rubber apron, and rubber boots with no perforations should be used when handling the body. ü If an animal anthrax case is confirmed, the affected property is quarantined, potentially exposed stock vaccinated, dead animals buried and contaminated sites disinfected. ü Control of dusts and proper ventilation in hazardous industries especially those that handle raw animal materials.

Thank you…
- Slides: 27