Anterior pituitary cells and hormones Cell type Pituitary


")






 Øsynthesized in the adenohypophysis, the concentration in the pituitary is 5")







 In children and adults • GH is secreted")







- Slides: 32
Anterior pituitary cells and hormones Cell type Pituitary Product population Target Corticotroph 15 -20% Thyrotroph Gonadotroph 3 -5% 10 -15% Adrenal gland ACTH b-lipotropin Adipocytes Melanocytes TSH Thyroid gland LH, FSH Gonads Somatotroph 40 -50% GH Lactotroph 10 -15% PRL All tissues, liver Breasts gonads
Anterior pituitary hormones
Where does it come from? • Synthesized and secreted by somatotroph cells (anterior pituitary) in response to growth-hormone releasing hormone (GHRH) from the hypothalamus • Activates gene transcription by cyclic adenosine monophosphate (c. AMP) mechanisms
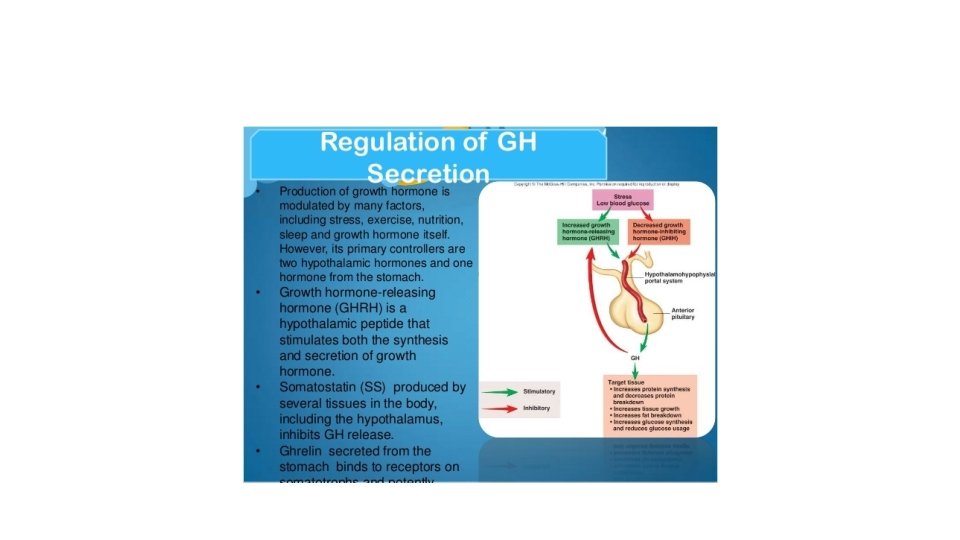
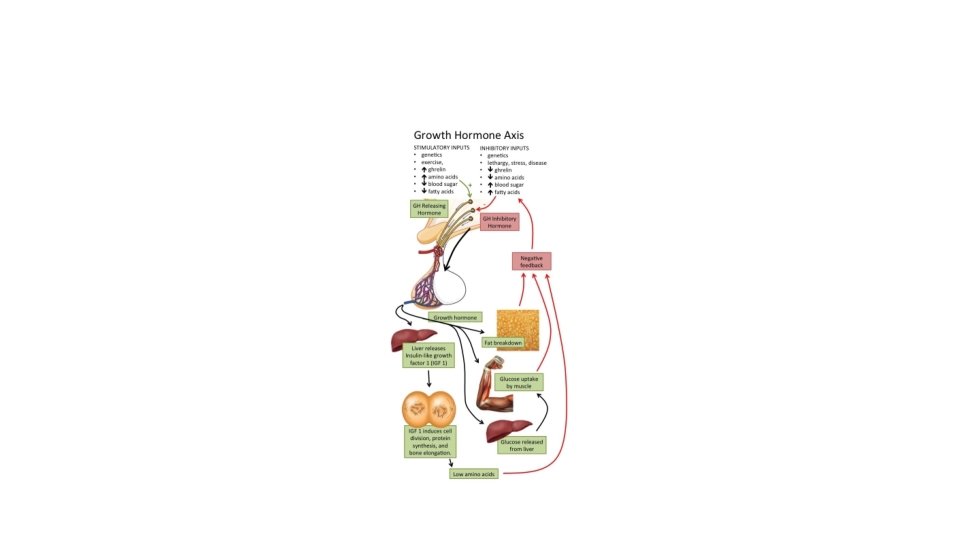
Regulation of Growth Hormone Secretion • GH secretion controlled primarily by hypothalamic GHRH stimulation and somatostatin inhibition • Neurotransmitters involved in control of GH secretion– via regulation of GHRH and somatostatin
Regulation of Growth Hormone Secretion • Neurotransmitter systems that stimulate GHRH and/or inhibit somatostatin • Catecholamines acting via a 2 -adrenergic receptors • Dopamine acting via D 1 or D 2 receptors • Excitatory amino acids acting via both NMDA and non-NMDA receptors
Regulation of Growth Hormone Secretion § b-adrenergic receptors stimulate somatostatin release and inhibit GH § b-adrenergic receptors inhibit hypothalamic release of GHRH
Regulation of Growth Hormone Secretion • Additional central mechanisms that control GH secretion include an ultra-short feedback loop exerted by both somatostatin and GHRH on their own secretion
Growth hormone vs. metabolic state • When protein and energy intake are adequate, it is appropriate to convert amino acids to protein and stimulate growth. hence GH and insulin promote anabolic reactions during protein intake • During carbohydrate intake, GH antagonizes insulin effects-- blocks glucose uptake to prevent hypoglycemia. (if there is too much insulin, all the glucose would be taken up). • When there is adequate glucose as during absorptive phase, and glucose uptake is required, then GH secretion is inhibited so it won't counter act insulin action.
Growth hormone vs. metabolic state • During fasting, GH antagonizes insulin action and helps mediate glucose sparing, ie stimulates gluconeogenesis • In general, during anabolic or absorptive phase, GH facilitates insulin action, to promote growth. • during fasting or post-absorptive phase, GH opposes insulin action, to promote catabolism or glucose sparing
Growth hormone (GH) Øsynthesized in the adenohypophysis, the concentration in the pituitary is 5 -15 mg/g Øsingle polypeptide, two disulfide bridges Øis essential for postnatal growth
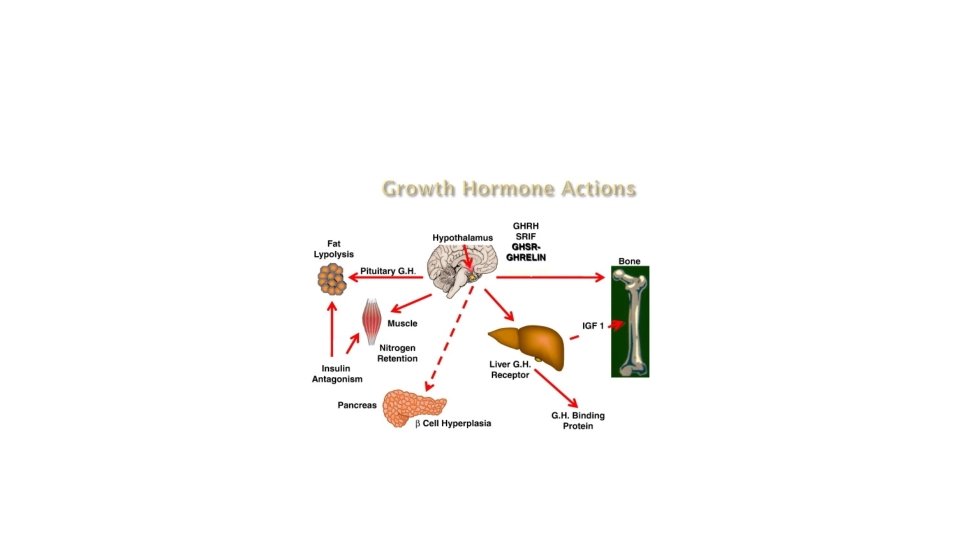
Biochemical actions 1. GH increases protein synthesis 2. Carbohydrate metabolism: GH antagonizes the effects of insulin (hyperglycemia); decreased peripheral utilization of glucose, increased hepatic production via gluconeogenesis 3. Lipid metabolism: GH promotes the release of free fatty acids and glycerol from adipose tissue, increases circulating free fatty acids, causes increased oxidation of free fatty acids in the liver 4. Mineral metabolism: GH promotes a positive calcium, magnesium, and phosphate balance (promotes growth of long bones) 5. Prolactin-like effects Pathophysiology: dwarfism, gigantism, acromegaly
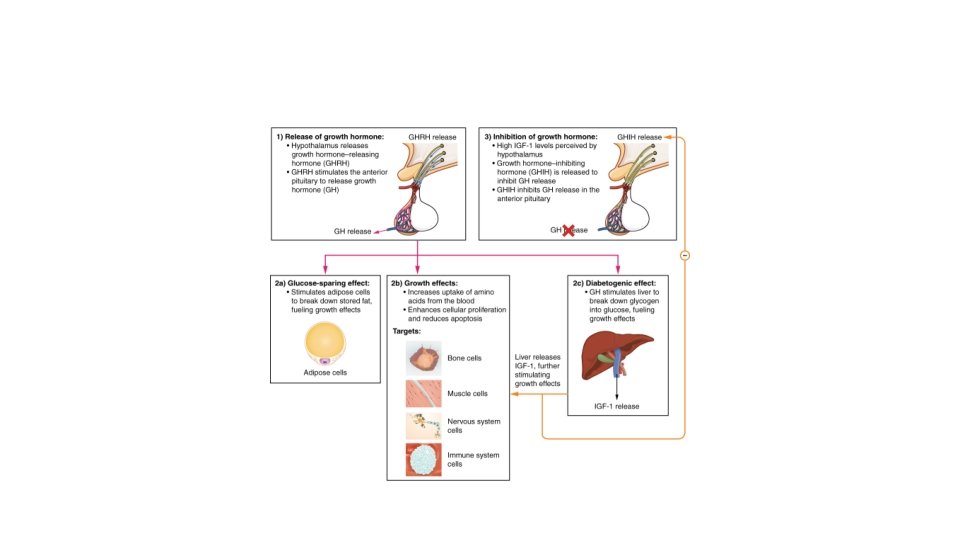
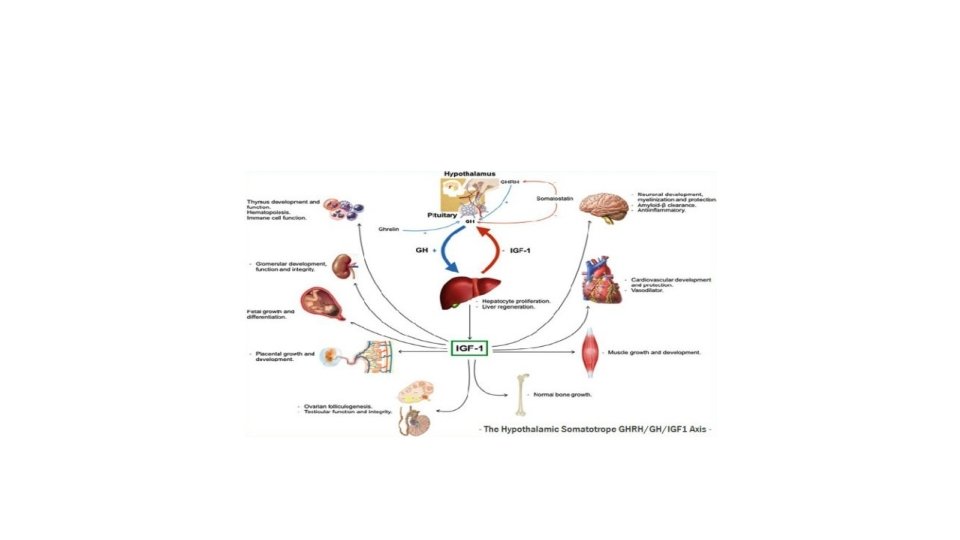
Role in growth Growth hormone travels through the blood and stimulates the liver to produce a protein called insulinlike growth factor (IGF-1) In children, IGF-1 stimulates chondrocytes to multiply in the cartilage at the ends of long bones (epiphyseal plate) �This leads to growth in the length of the bones and increases the child's height �In adults, growth hormone plays an important role in repair and maintenance of the body’s tissues IGF-1 also acts on immature muscle cells to increase muscle mass
Role in metabolism Protein metabolism: �Increased amino acid uptake �Increased protein synthesis Fat metabolism: �Triglyceride breakdown in adipocytes (lipolysis) Carbohydrate metabolism: �Helps maintain blood glucose levels �Suppresses insulin to prevent uptake of glucose in peripheral tissues �Glucose synthesis in the liver (gluconeogenesis)
Primary Target tissues • Bone • Muscle • Fat
Negative Feedback • IGF-I • Directly suppresses the somatotroph cells • Stimulates the release of somatostatin from the hypothalamus • Growth hormone • Directly suppresses the somatotroph cells • Inhibits GHRH secretion
Feedback control of growth hormone
Acromegaly and Gigantism • Caused by eosinophilic adenomas of somatotrophs • Excess GH leads to development of gigantism if hypersecretion is present during early life– a rare condition • Symmetrical enlargement of body resulting in true giant with overgrowth of long bones, connective tissue and visceral organs. • Excess GH leads to acromegaly if hypersecretion occurs after body growth has stopped. • Elongation of long bones not possible so there is over growth of cancellous bones– protruding jaw, thickening of phalanges, and over growth of visceral organs
GH excess – Types. 2. (age) In children and adults • GH is secreted more than body requirements • The effects of GH excess depend on the age of onset, both in children and adults – 2 conditions • Giantism or Gigantism : This condition occurs in children when epiphysis are not Fused • Acromegaly: when epiphysis are fused in adults
GH excess in adults – Acromegaly excess of GH/IGF-1 • Acromegaly results from excessive secretion of growth hormone in adults with fused epiphysis • It is usually the result of benign pituitary adenoma in middle aged individuals • Excessive secretion of GH leads to excessive generation of IGF 1 - the mediator for the effects of GH
Acromegaly – No ↑in height ↑in soft tissue /viscera • • • There is no ↑ in height but soft tissue proliferation. There is Enlargement of bones of hands and feet with swelling Over growth of the Skull, lower jaw and bulging of forehead Prominent nose, thick lips and tongue ↑ in the size of the viscera like Liver and heart
Acromegaly –↑ in bone thickness and soft tissues
Acromegaly - Wide sole of foot
Acromegaly – Large skull, lower jaw, prominent nose and bulging forehead
GH excess in Children- Giantism when epiphysis are not fused • Giantism in children and adolescents occurs when epiphysis are not fused • Chronic GH secretion leads to linear growth of long bones usually to 7 - 9 feet • Hyper secretion of GH is commonly associated with hypogonadism and cause of non fusion of epiphysis
Gigantism 7 feet 8 inches Pituitary gland tumor