Anterior ischemic optic neuropathy AION Nahid Rezaei Pour
 Nahid Rezaei Pour MS of critical car nursing")







 n Most common over 50 years n Painless monocular")
 n AION is due to acute ischemia of the")



 n Older patients (mean")


")



")
 More common 90 -95% of AION n In")

 n Systemic")






- Slides: 38
Anterior ischemic optic neuropathy (AION) Nahid Rezaei Pour MS of critical car nursing
The Eye n n n The eye is often compared to a camera. Light comes in through the cornea, pupil, and lens in front of the eye just as the lens of the camera lets light in the film. This light is then focused on the inside wall of the eye called the retina (as on the film in a camera). This picture is then sent to the brain along the optic nerve, which connects the eye to the brain. We see properly when all of these parts of the eye and brain are working together
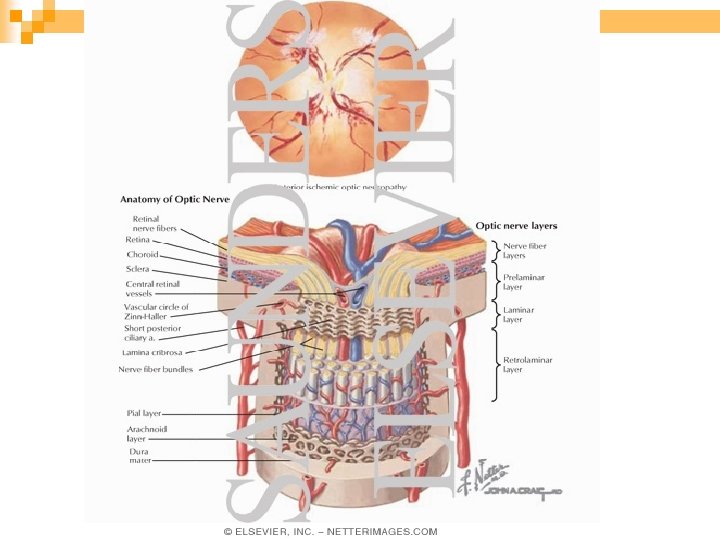
The Optic Nerve n n The optic nerve is unique because it is the only nerve in the body that a physician is able to see directly. The optic nerve is made up of a million tiny, delicate nerve fibers that are like wires. Many blood vessels nourish the optic nerve with blood rich in oxygen and nutrition. Vision actually takes place in the brain when the messages from the eye travel to the brain along the optic nerve; however, the nerve has to be healthy to transmit these messages.
n n While explaining this disease, a doctor may say that there has been a "stroke at the back of the eye", "blocked blood vessel", or "broken blood vessel at the back of the eye". A "stroke" is an interruption of the blood supply to the brain or a nerve in the body. With a "stroke at the back of the eye" a loss of vision develops because the retina or the optic nerve may have its circulation interrupted. How much vision is lost depends on how much the retina or the optic nerve is affected
Ischemia n n Ischemia of the optic nerve results in ischemic optic neuropathy Ischemia is a decrease in the blood supply to a tissue in the body which in turn decreases oxygen and nutrition. n Without sufficient oxygen and nutrition, nerves cannot function properly and will eventually die n The blood supply of the anterior of the optic nerve (also called the optic nerve head) is mainly by the posterior ciliary arteries, while the blood supply to the posterior part is from several quite different sources but not the posterior ciliary arteries.
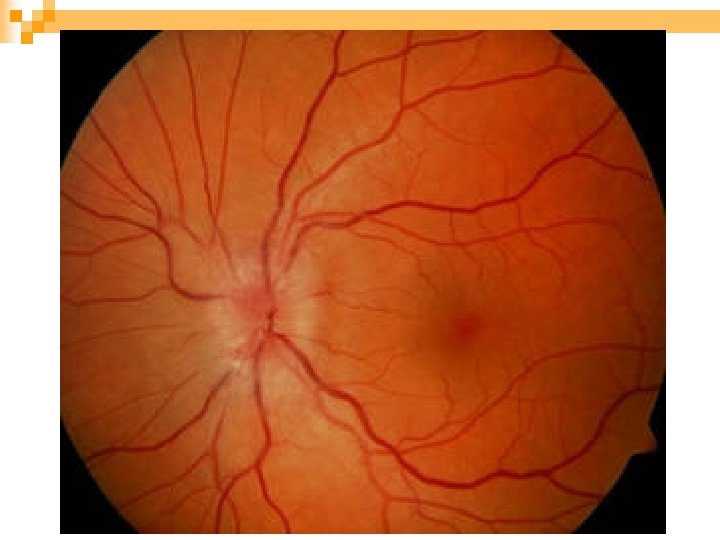
Normal eye
The blood supply of the anterior of the optic nerve (also called the optic nerve head) is mainly by the posterior ciliary arteries, while the blood supply to the posterior part is from several quite different sources but not the posterior ciliary arteries.
Types of Ischemic Optic Neuropathy n Ischemic optic neuropathy is of two types depending upon the part of the optic nerve involved: 1. Anterior ischemic optic neuropathy (commonly abbreviated to "AION“ 2. Posterior ischemic optic neuropathy (commonly abbreviated to "PION"
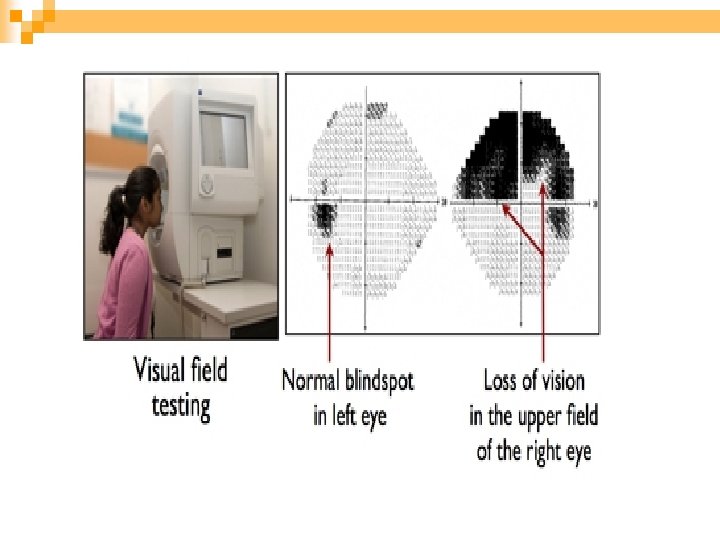
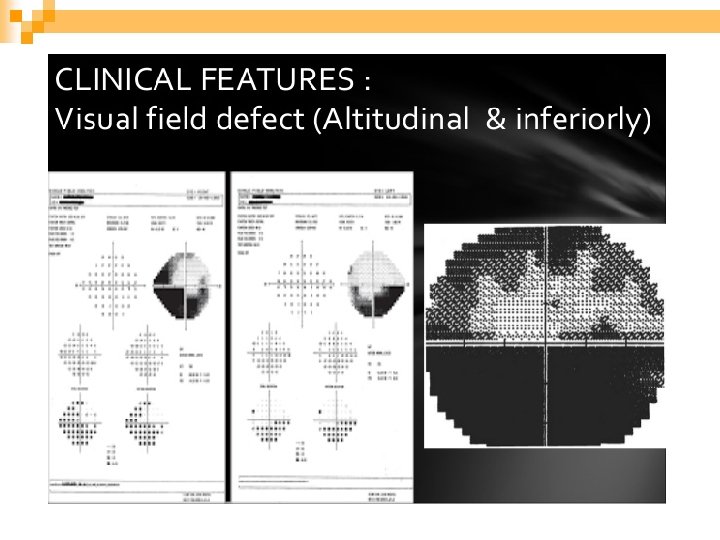
Anterior ischemic optic neuropathy (AION) n Most common over 50 years n Painless monocular vision loss that develops over hours to days n Visual acuity may be diminished n Visual field loss always occur(Altitudinal) n RAPD(Relative Afferent Pupillary Defect)or APD/Marcus. Gunn pupil is peresent unless the optic neuropahty is bilatral.
Anterior ischemic optic neuropathy (AION) n AION is due to acute ischemia of the front (anterior) part of the optic nerve AION is of two types depending on what causes it: n Arteritic AION: This is the most serious type and is due to (vasculitis) a disease called giant cell arteritis or temporal arteritis. n Non-arteritic AION: This is the usual, most common type, with many different causes but not associated with thrombosis or embolism
Arteritic AION AAION
Arteritic AION n Giant cell arteritis is one medical emergency in ophthalmology. n This is a disease of persons aged 50 years or older. n more common among women than men. n About 80% of patients with AION due to giant cell arteritis will have felt generally unwell for some time n However, 20% have no such general symptoms and are perfectly healthy.
AAION
AAION n AAION is less frequent than NAION (5 -10%) n Older patients (mean age 70 year) n It is coused by inflammatory and thrombotic occlusion of the short posterior cilliary arteries. n Systemic symptoms of GCA are usually present
Systemic Findings of GCA n Are usually present ¨Headache, temporal and scalp tenderness ¨Jaw claudication ¨Malaise, anorexia, weight loss, fever, joint & muscle pain ¨Ear pain
To help determine if giant cell arteritis is present, a physician will want to know about the following problems: n n n n n Pain while chewing food Pain in the temples and/or neck Scalp tenderness Loss of appetite Loss of weight Headaches Unusual fatigue or sleepiness Muscular aches and pains Regarding the loss of vision
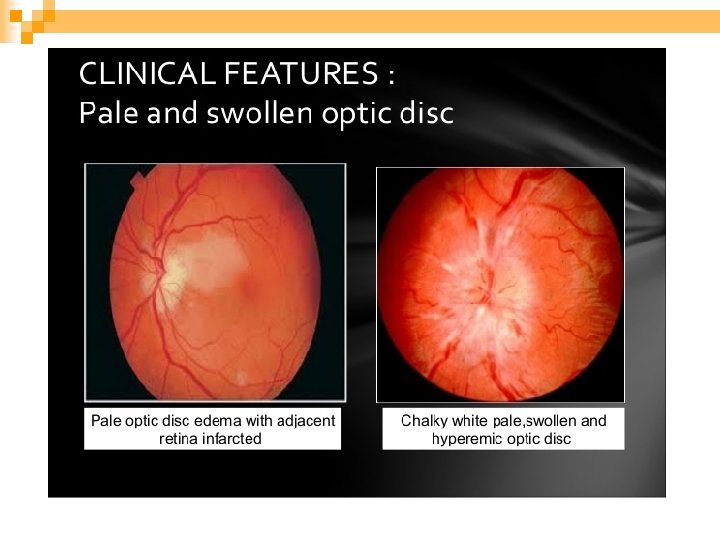
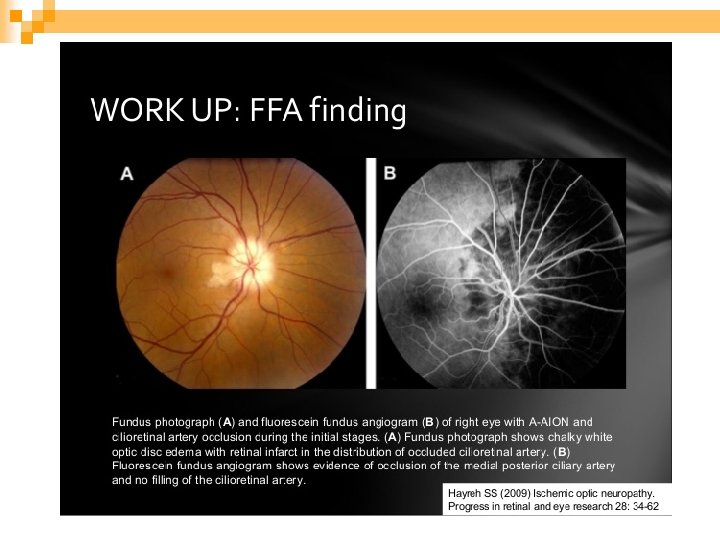
AAION n n n n Sever visual loss(VA is <20/200 in 60% of patients) Pale edema Cotton wool spot Delayed choroidal filling on fluorscein angiogeraphic stdies Normal cup. ESR CRP
Treating AAION n Immediate therapy is critical n IV methylprednisolone 1 g/day for 3 -5 days n Then oral prednisolone 1 mg/kg/d may be use up to 100 mg/day. n tapered slowly over 3 -12 month or more, depending on response. n Temporal artery biopsy
AAION n Major Goals of AAION Therapy is prevent contralateral visual loss. n untreated, fellow eye involved 95% of cases, whithin days to weeks n Risk of recurrence is 7% so tapering must be done slowly and carefully.
Nursing points n Effective communication with patients n Patient Education n Medication Ø Osteoporosis Peptic ulcer Considering the administration of methylprednisolone Ø Ø
Nonarteritic Anterior ISchemic Optic Neuropathy (NAION)
Nonarteritic Anterior ISchemic Optic Neuropathy (NAION) More common 90 -95% of AION n In younger age groups than arteritic form (mean age 60 yr) n The annual incidence is approximately 80/100, 000. n Systemic symptoms are absent n
NAION n V. A > 20/200 in over 60% of cases n Palor is less common n Optic disk in other eye is small and small or absent cup (disk at risk) n The 5 year risk of other eye is 15%
Risk Factors of NAION Structural crowding of the disk (disk at risk) n Systemic hypertension n Diabetes mellitus (young) n Smoking, hyperlipidemia n Hyperhomocysteinemia, platelet polymorphism, sleep apnea n Atherosclerosis n
Differential Diagnosis of NAION Optic neuritis n Infiltrative optic neuropathies n Anterior orbital lesion n Diabetic papillopathy n
NAION Optic neurtis Age >50 <40 pain Unusual 92%+ Pupil APD+ VF Altitudinal Central Optic disk Edema 100% pale Edema 33% hyperemic Unusual Retinal hemorrhage Common F. A. Delayed disk filling No delayed MRI No optic nereve enhancement
Treatment of NAION Untreated case remain stable n Recurrence unusual 6. 4% n No proven therapy surgery no benefit n No proven prophylaxis n Asprin reducing incidence of fellow eye is unclear n
Emperical Treatment of NAION n Hydration Drop: Brimodine n Tab: Memantine n Tab: Vitamin B 1 n Amp: Erythropoietin iv n Amp: Triamcinolon intravitreal n
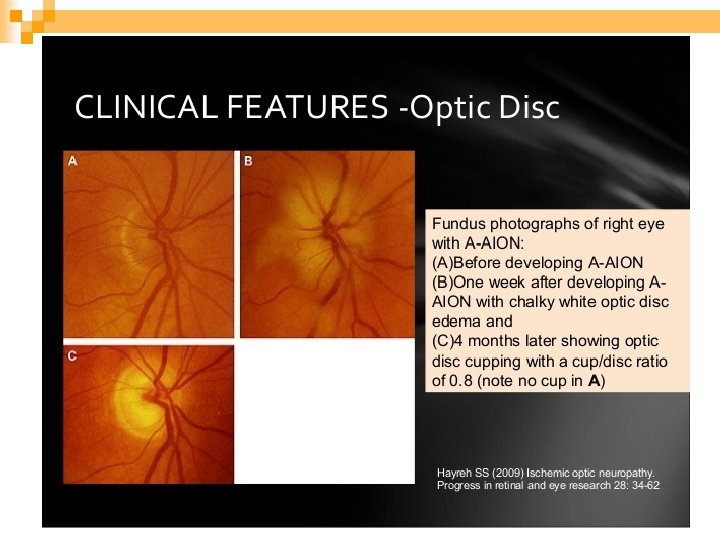
Characteristic Arteritic Features Non arteritic Features Age Mean 70 years 60 years Sex F>M F=M Symptoms Headache, scalp tender ness, … Usually none VA <20/200 60% >20/200 60% Disc/Fundus Pallid disc edema common cup normal Cotton-wool spots Cup small Hyperemic disc edema ESR Mean 70 mm/hr Mean 20 -40 mm/hr C. R. P. Elevated Normal Platelet count Elevated or normal Normal Fluorscein angiogeraphy finding Disc delay and choroid delay Disc delay Natural history Rarely improved 54 -95% fellow eye 31% improved 12 -19% fellow eye treatment Systemic steroids None proven
THANK YOU FOR YOUR ATTENTIO