Anterior ischemic optic neuropathy AION Most common over

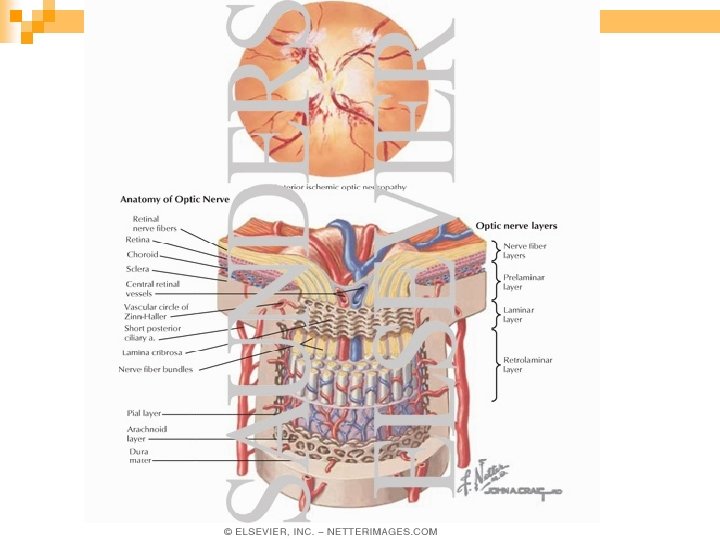








 n Systemic hypertension n")




- Slides: 22
Anterior ischemic optic neuropathy (AION( Most common over 50 years n Painless monocular over hours to days n Visual acuity n Visual field n APD n
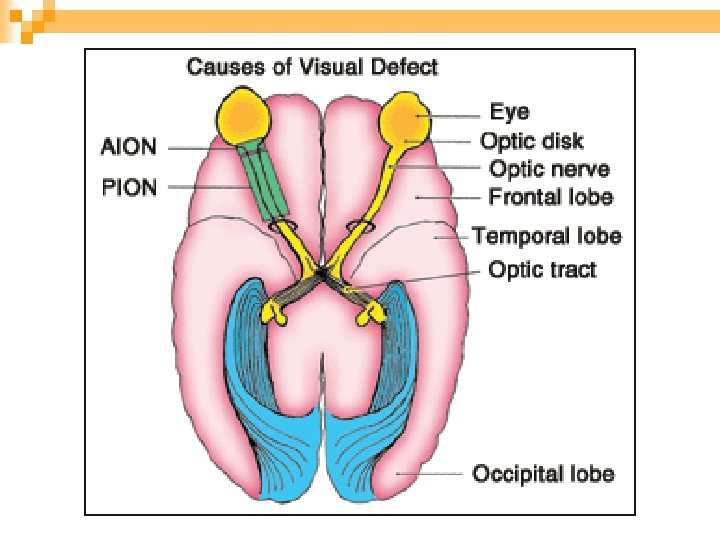
AION Arteritic AION is associated with giant cell arteries (GCA( n Nonarteritic AION n
AAION Is less frequent 5 -10% n Older patients (mean 70 yr( n Inflammatory and thrombotic occlusion post. Cilliary artery n Systemic symptoms n
Systemic Findings of GCA n Are usually present ¨ Headache, temporal and scalp tenderness ¨ Jaw claudication ¨ Malaise, anorexia, weight loss, fever, joint & muscle pain ¨ Ear pain
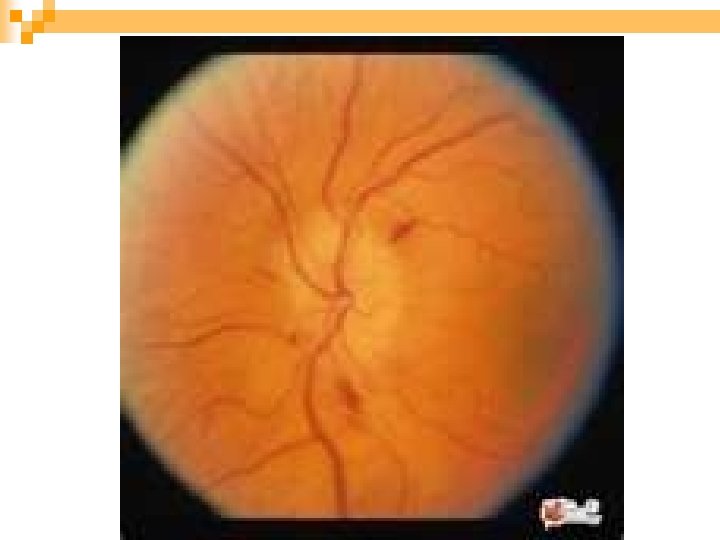
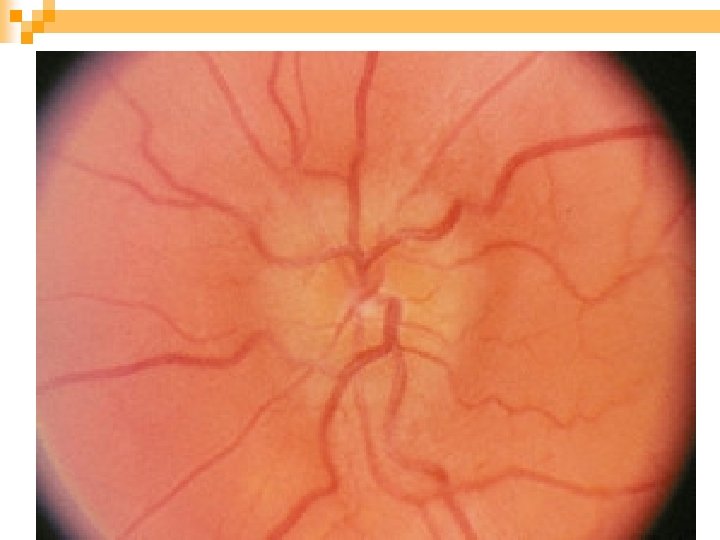
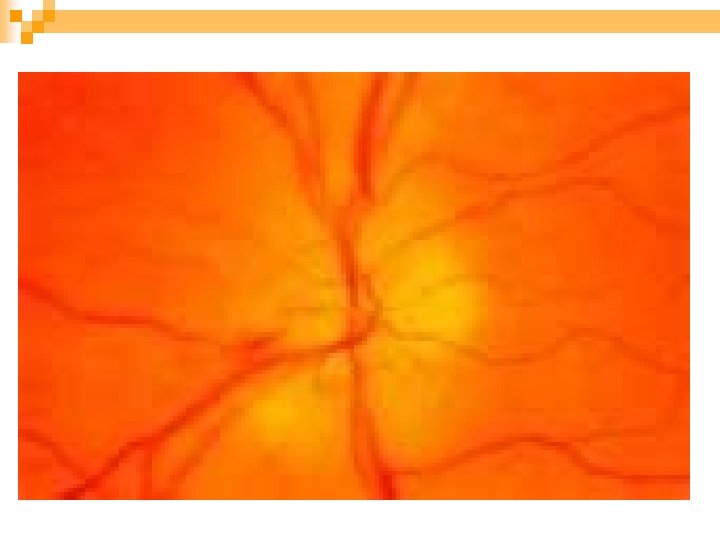
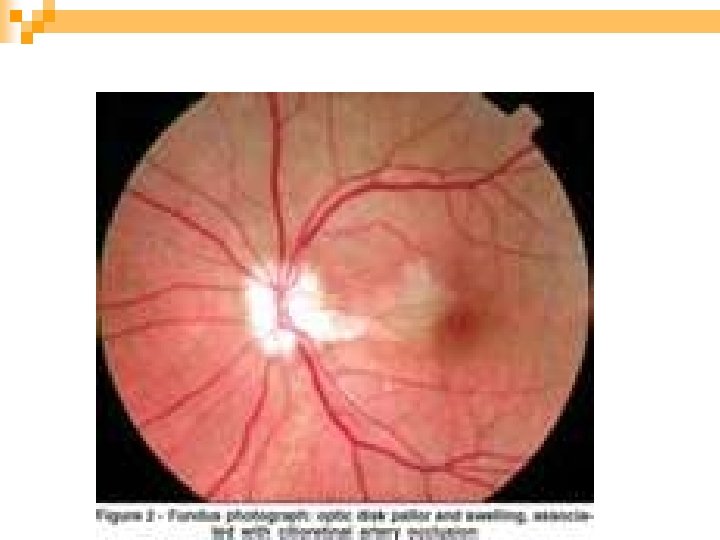
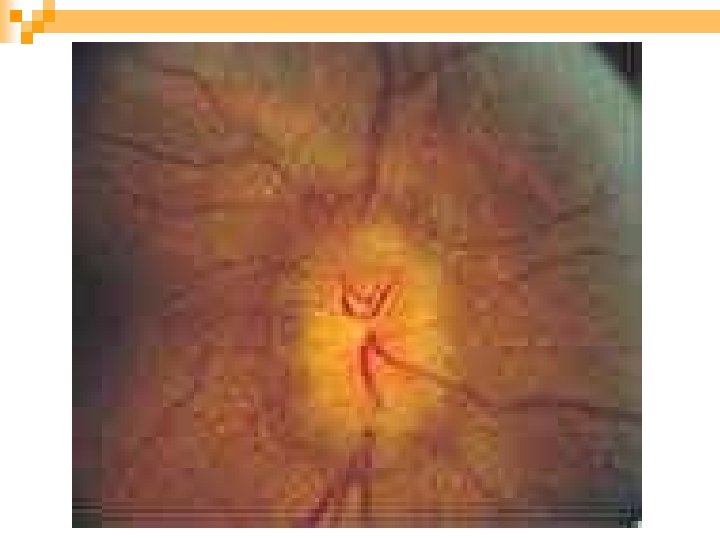
AAION Sever visual loss n Pale edema n Cotton wool spot n F. A. delayed choroidal filling n Normal cup. n
Treating AAION Immediate therapy is critical n Temporal artery biopsy may delayed treat n IV prednisolone 1 g/day for 3 -5 days n Then oral prednisolone 100 mg/day tapered 3 -12 month or more n
Major Goals of Therapy Prevent contralateral visual loss n Fellow eye involved 95% days or weeks n Affected eye improve somewhat n Avoid systemic vascular complication n Risk of recurrence is 7% so tapering must be slow and careful n
Nonarteritic Anterior ISchemic Optic Neuropathy (NAION( More common 90 -95% of AION n In younger age groups (mean age 60 yr( n Related to optic disc microcirculation n On awakening, noctural systemic Hypotension n Systemic symptoms are absent n
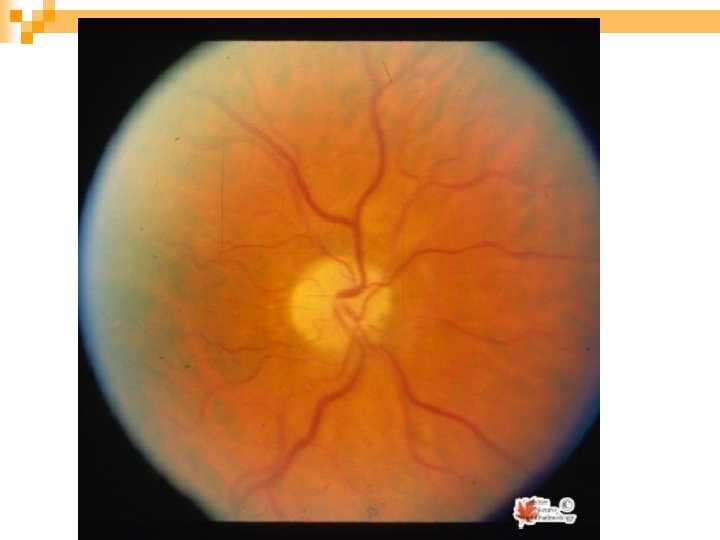
NAION V. A. > 20/200 in over 60% of cases n Palor is less common n Optic disk in other eye is small and small or absent cup. n 5 yr risk of other eye is 14. 7% (psuedfoster kennedy syd( n
Risk Factors of NAION Crowding of disk (disk at risk) n Systemic hypertension n Diabetes (young) n Smoking, hyperlipidemia n Hyperhomocysteinemia, platelet polymorphism, sleep apnea n Phosphodiestrase inhibitors (sildenafil or viagra) ? ? Hypotensive effect n
Differential Diagnosis of NAION Optic neuritis n Infiltrative optic neuropathies n Anterior orbital lesion n Diabetic papillopathy n
NAION Optic neurtis Age >50 <40 pain Unusual 92%+ Pupil APD+ VF Altitudinal Central Optic disk Edema 100% pale Common Edema 33% hyperemic Unusual Retinal hemorrhage F. A. MRI Delayed disk No delayed filling No optic nereve enhancement
Treatment of NAION Untreated case remain stable but recovery of 3 lines 31% after 2 years n Recurrence unusual 6. 4% n No proven therapy surgery no benefit n No proven prophylaxis n Asprin reducing incidence of fellow eye is unclear n
Age summary Mean 70 yr 60 yr Sex F>M F=M Symptoms Headache … None VA <20/200 60% >20/200 60% Fundus Normal cup pale edema ESR Mean 70 mm/hr Small cup Hyperemic edema Mean 20 -40 mm/hr C. R. P. Elevated Normal Natural history Rarely improved 31% improved 54 -95% fellow 12 -19% fellow eye Systemic steroids None proven treatment