Antepartal hemorrhagic Disorders Chapter 28 Learning Objectives Differentiate

Antepartal hemorrhagic Disorders Chapter 28

Learning Objectives Differentiate among causes of early pregnancy bleeding, including miscarriage, ectopic pregnancy, reduced cervical competence, and hydatidiform mole. Discuss signs and symptoms, possible complications, and management of miscarriage, ectopic pregnancy, cervical insufficiency, and hydatidiform mole.
 Compare and contrast placenta previa and placental abruption in relation")
Learning Objectives (Cont. ) Compare and contrast placenta previa and placental abruption in relation to signs and symptoms, complications, and management. Discuss the diagnosis and management of disseminated intravascular coagulation.

Antepartum Hemorrhagic Disorders Bleeding in pregnancy jeopardizes maternal and fetal well-being Maternal blood loss decreases oxygencarrying capacity, increases risk for: n n n Hypovolemia Anemia Infection Preterm labor Adverse oxygen delivery to the fetus
 Fetal risks from maternal hemorrhage n n n Blood")
Antepartal Hemorrhagic Disorders (cont. ) Fetal risks from maternal hemorrhage n n n Blood loss, anemia Hypoxia Anoxia Preterm birth

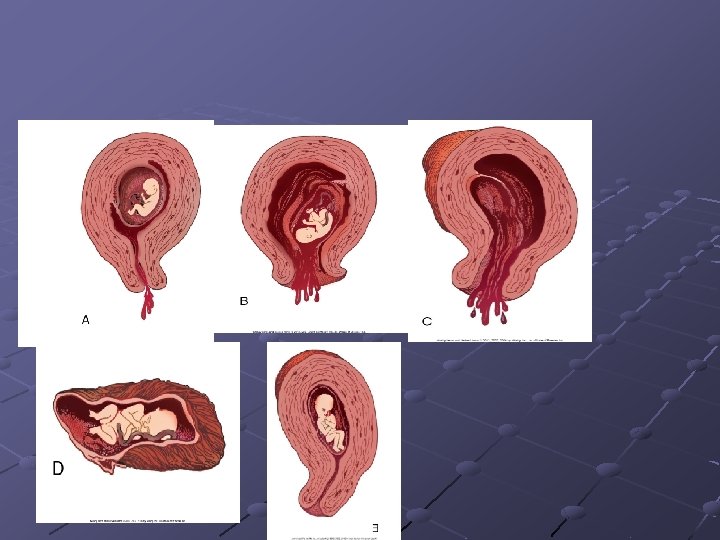
Early Bleeding Ø Miscarriage Ø Ø Spontaneous abortion- a pregnancy that ends before 20 weeks of gestation Types of miscarriages ØThreatened- include spotting of blood but with cervical os closed. ØInevitable and incomplete-miscarriages involve a moderate to heavy amount of bleeding with an open os ØComplete- all fetal tissue is passed, the cervix is closed
 Ø Missed- a pregnancy in which the fetus has died Ø")
Early Bleeding (Cont) Ø Missed- a pregnancy in which the fetus has died Ø Recurrent early (habitual )- is the loss of three or more previable pregnancies Ø Prostaglandin medications-Cytotec Ø Dilatation and Evacuation (D&C)commonly performed to treat inevitable and incomplete miscarriage
 Ø Incompetent Cervix (Recurrent Premature Dilatation of the Cervix) Ø Ø")
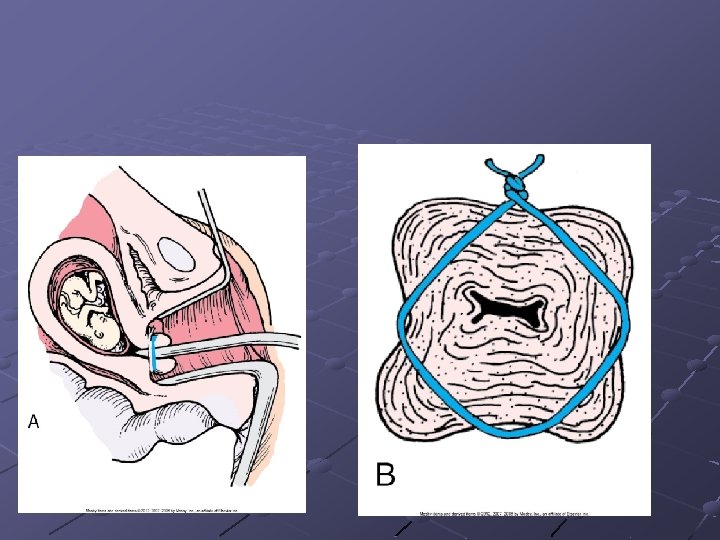
Early Bleeding (cont) Ø Incompetent Cervix (Recurrent Premature Dilatation of the Cervix) Ø Ø Ø Ø Passive and painless dilatation of the cervix during the second trimester Cervical Funneling Bed rest, pessaries, antibiotics an anti-inflammatory, And progesterone supplementation Cervical cerclage Electively removed when the woman reaches 37 weeks of gestation

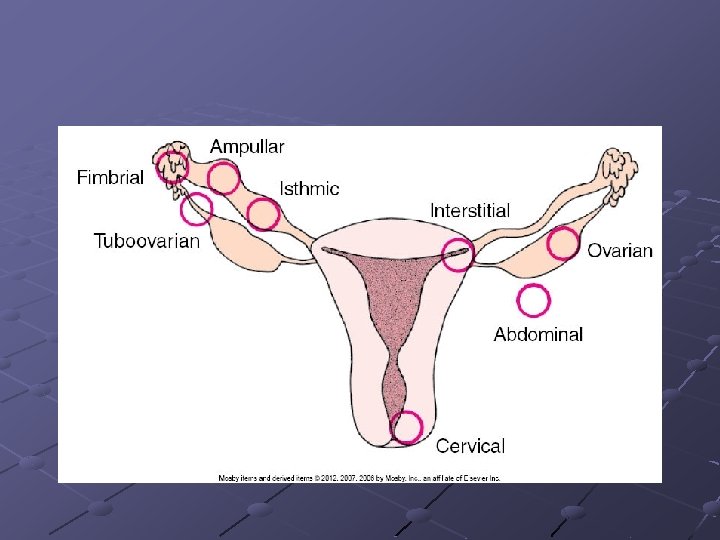
Early Bleeding Ø Ectopic Pregnancy Ø Ø Ø Ø One in which the fertilized ovum is implanted outside the uterine cavity Pain may be unilateral, bilateral, or diffuse over the abdomen Dark red or brown abnormal vaginal bleeding Referred shoulder pain Removal of the ectopic pregnancy by salpingostomy is possible before rupture

ll
 Ø Complete mole results from fertilization of")
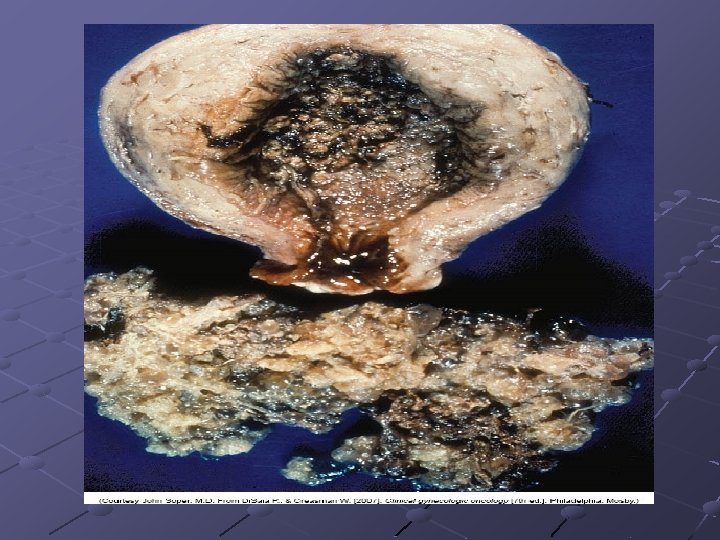
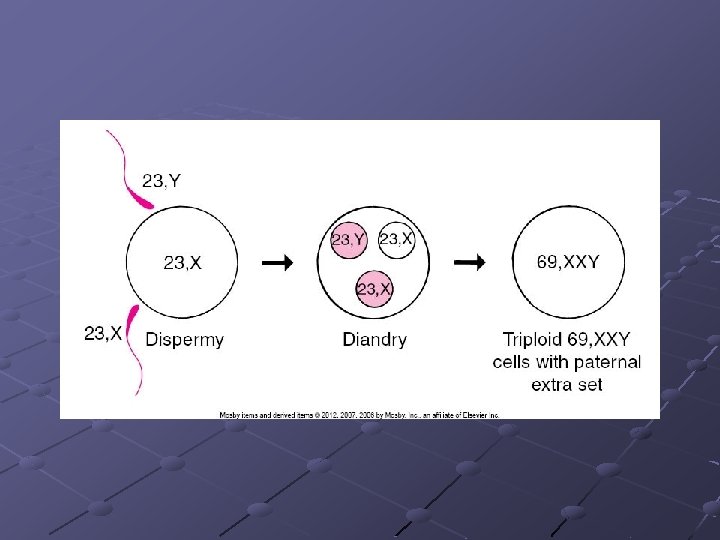
Early Bleeding Ø Hydatidiform Mole (molar pregnancy) Ø Complete mole results from fertilization of an egg with a lost or inactivated nucleus Ø Resembles a bunch of white grapes Ø Contains no fetus, placenta, amniotic membranes or fluid Ø Partial mole often has embryonic or fetal parts and an amniotic sac Ø 20 % of cases of complete mole, progression toward choriocarcinoma occurs
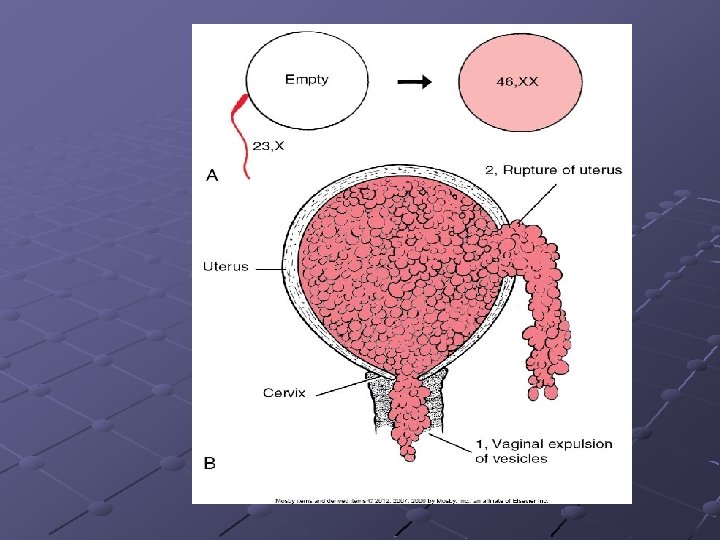

Early Bleeding Hydatidiform mole Vaginal bleeding Early in pregnancy the uterus is significantly larger than expected from menstrual dates Most moles abort spontaneously Woman should reframe from getting pregnant for 6 months to a year

Late Bleeding Ø Placenta Previa Ø Condition in which the placenta is implanted in the lower segment near or over the internal cervical os Ø Three types of placenta previa Ø Ø Incomplete (or partial)- if the internal os is entirely covered by the placenta when the cervix is fully dilated Marginal placenta previaimplies incomplete coverage of the internal os
 Marginal placenta previaindicates that only an edge of the placenta extends")
Late Bleeding (cont) Marginal placenta previaindicates that only an edge of the placenta extends to the internal os Painless vaginal bleeding Previa should be suspected whenever vaginal bleeding occurs during the second or third trimester (after 20 weeks) Vaginal bleeding is bright red
 Placenta Previa Standard diagnosis for previa is a transvaginal ultrasound Lab")
Late Bleeding (cont) Placenta Previa Standard diagnosis for previa is a transvaginal ultrasound Lab studies include: H &H , blood type and RH factor, coagulation profile, and type and crossmatch
 Placenta previa Expectant management consists of rest and close observation for")
Late Bleeding (cont) Placenta previa Expectant management consists of rest and close observation for women less than 36 weeks gestation Ultrasound NST Pad counts H&H and coagulation values monitored closely C/S vs. vaginal delivery
 Ø Maternal hypertension is probably the most consistently identified risk factor")
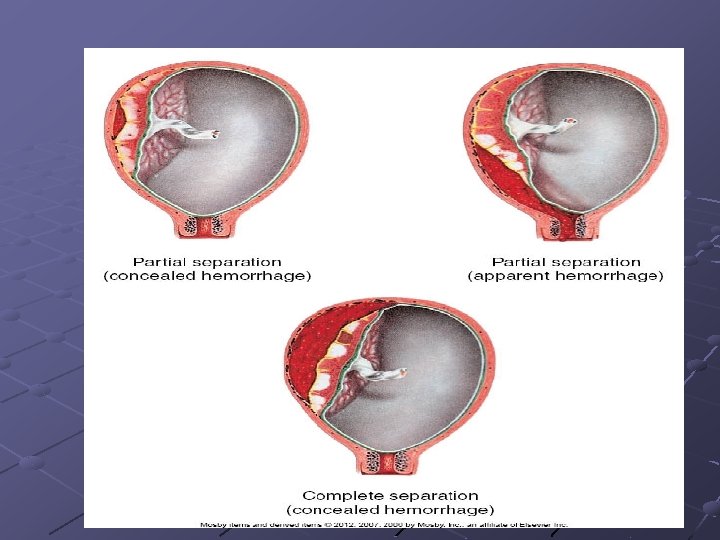
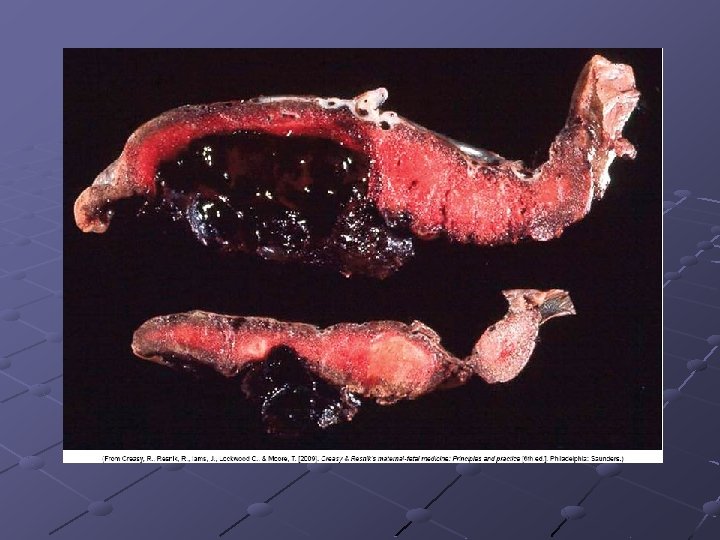
Late Bleeding (cont) Ø Maternal hypertension is probably the most consistently identified risk factor for abruptio Ø Types of abruptio placenta Ø Partial ( concealed hemorrhage)- woman has uterine tenderness and tetany, but neither the mother nor baby is in distress Ø 10 to 20% of the total placental surface is detached Abruptio Placentae- is the detachment of part or all of the placenta from its implantation site.
 Partial separation (apparent hemorrhage)- woman has uterine tenderness, and tetany with")
Late Bleeding (cont) Partial separation (apparent hemorrhage)- woman has uterine tenderness, and tetany with or without external evidence of bleeding Complete separation (concealed hemorrhage)uterine tetany is severe; the woman is in shock; and the fetus is dead Classical symptoms include: vaginal bleeding, uterine tenderness and contractions, and abdominal pain
 Abruptio placentae Treatment depends on the severity of blood loss and")
Late Bleeding (cont) Abruptio placentae Treatment depends on the severity of blood loss and fetal maturity and status Woman is hospitalized and observed closely for signs of bleeding and labor C/S delivery
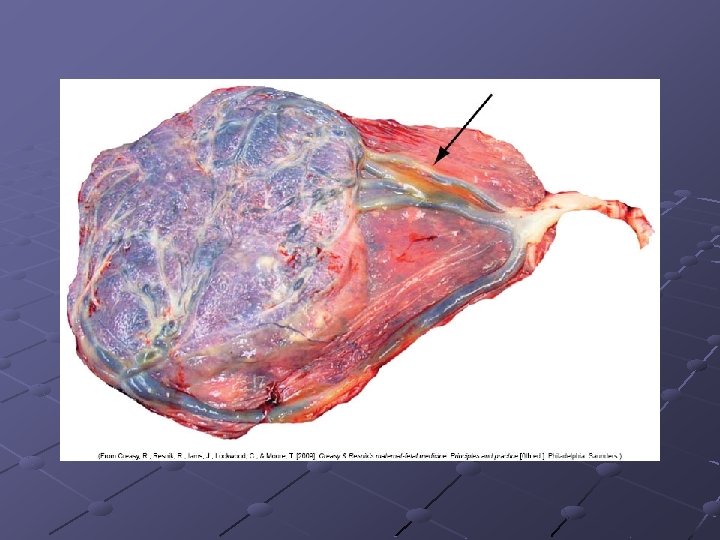
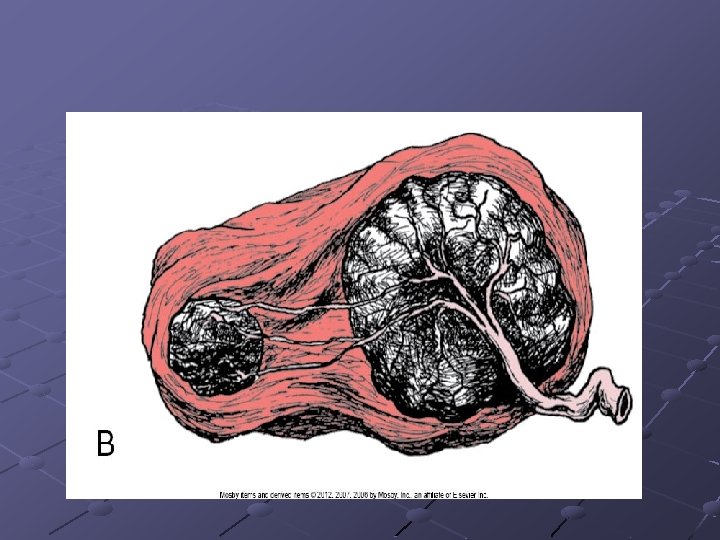
 Velamentous insertion of the cord Rare placental anomaly associated with placenta")
Late Bleeding (cont) Velamentous insertion of the cord Rare placental anomaly associated with placenta previa and multiple gestation Cord vessels begin to branch at the membranes Course onto the placenta Fetus may rapidly bleed to death
- Slides: 30