Antenatal Optimisation in Preterm Infants 34 w A













 General It is recommended that")
 Parents • Information for parents")










- Slides: 27
Antenatal Optimisation in Preterm Infants <34 w: A Quality Improvement Toolkit British Association of Perinatal Medicine In collaboration with the National Neonatal Audit Programme September 2020 To be used for staff education in conjunction with the Antenatal Optimisation Toolkit For all references see Antenatal Optimisation Toolkit
The Perinatal Optimisation Care Pathway The Quality Context Key optimisation timepoints Elements of the BAPM Antenatal Optimisation Toolkit Other BAPM Optimisation Toolkits The Perinatal Optimisation Care Pathway Counselling of parents and shared decision-making M bre atern ast a mil l k Nor mo th erm ia Per Op ipartu tim isat m ion Op ma timal nag cor em d ent tics ibio Ant e ste natal roid s Ma gne sium ce o f bi rth Ant opt enata imi l sat ion Pla gth len ical Cer v F one etal ctin fibr Det a hist iled ory Pre dictio term n o Birt f h The Perinatal Team
Purpose of toolkit • To facilitate delivery of key antenatal optimisation measures known to improve preterm outcomes. • To support clinicians leading and participating in QI in maternity units by providing practical resources in the form of a toolkit and supporting materials • This toolkit will: • Provide the evidence base for effective interventions • Facilitate units in interrogating their own data and processes in order to undertake selected quality improvement activities suited to the local context • Assist units in interpreting and monitoring the results of their QI activity • Provide and signpost resources to facilitate QI in the area of improving antenatal optimisation in the preterm infant
Rationale for AO • Reduces cerebral palsy by 30% • Reduce death by 30% • Reduce NEC by 50% • Reduce s. IVH by 45% 1 more baby surviving for every 8 -10 women treated <26 w 1 fewer baby with infection for 9 GBS+ women treated in PTL • The risk of death from GBS in preterm infants is 25% and 10 times that of term infants Steroids Magnesium Antibiotics Place of birth 1 fewer baby with CP for every 37 women treated <30 w 1 more baby surviving for every 20 women transferred • If not born in a tertiary unit: • 2 -3 x higher risk s. IVH/PVH • 1. 3 x higher risk of death For all references see Antenatal Optimisation Toolkit
Evidence and professional recommendations
Prediction of preterm birth • Preterm birth history alone: 10 -57% of pregnant women with a PTB history will give birth preterm. Most women who give birth preterm do not have a history of preterm birth. • QUi. PP App: Using a 5% chance of birth, predicts PTB in next 7 d in women <37 w and avoids 90% of admissions • qf. FN: Predicts PTB <30 w in singleton/multiple pregnancy • Combination of Cervical Length and qf. FN: Addition of cervical length refines predictive ability of qf. FN and may save € 480 per patient • Placental growth factor and s. Flt-1/PGF ratio: Rules out pre-eclampsia within the next 7 d in women with suspected pre-eclampsia <35 w For all references see Antenatal Optimisation Toolkit
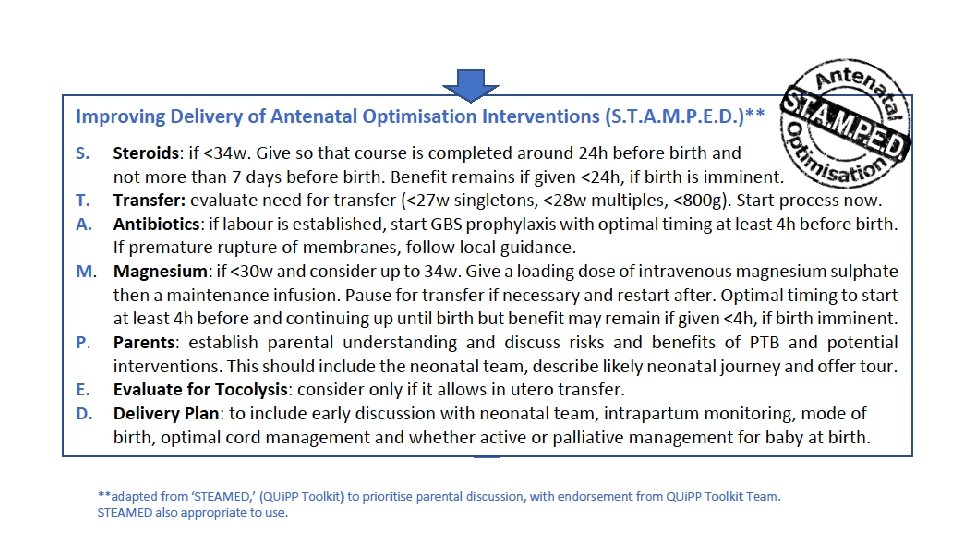
Steroids • A complete course of steroids reduce death by 30% in infants less than 34 w, including those <25 w where mortality effect is greater • Steroids also reduce RDS, IVH and NEC including in extreme preterm gestations • Optimum timing is within 7 d of birth with course completed 24 h before birth (only 22% of women who give birth <34 w receive steroids in this timeframe) • Benefits of steroids do not exceed 7 d • Mortality benefit remains for steroids given 6 -12 h before birth • Repeat courses reduce respiratory morbidity but do not reduce mortality and may impact fetal growth Focus should be on more accurate prediction of birth to inform more precise timing of antenatal steroids rather than a repeat dosing strategy For all references see Antenatal Optimisation Toolkit
Magnesium • Given within 24 h before birth at <32 w reduces the risk of cerebral palsy and death without risk to mother or fetus • Similar effects across a range of gestations including extreme preterm infants • Optimum level is at least 4 h after loading dose • Benefit remains if given <4 h where birth is imminent Antibiotics • Preterm prelabour rupture of the membranes and preterm labour are associated with early onset neonatal infection with GBS • Antibiotics given at least 4 h before birth reduces the risk of GBS sepsis tenfold For all references see Antenatal Optimisation Toolkit
Place of birth • If birth of an extreme preterm infant occurs in a high volume, neonatal intensive care setting, • Mortality is reduced by around 50% • There are reductions in NEC, IVH and PVL For all references see Antenatal Optimisation Toolkit
Overall Aim Accurate Prediction of Preterm Labour/ Need for Preterm Birth What Interventions? Who? -Detailed history QUi. PP app: symptoms, quantitative fetal fibronectin and cervical length, placental growth factor Steroids <34 weeks Magnesium <30 weeks *Consider 30+0 -33+6 w Antibiotics Optimising Place of Birth In utero transfer to NICU setting if: <27 weeks singleton Preterm labour or PPROM <28 weeks multiple <800 g When? >24 h and <7 d >4 h and <24 h *<24 h is still beneficial *<4 h is still beneficial Immediately • If these maternal interventions are not achieved before birth, the opportunity for benefit is lost •
Scottish Maternity and Neonatal Services Review The drivers for preterm Antenatal Optimisation within the UK Saving Babies Lives Version 2 British Association of Perinatal Medicine Maternity and Children Quality Improvement Collaborative PRETERM ANTENATAL OPTIMISATION European Standards of Care for Newborn Health National Neonatal Audit Programme World Health Organisation Maternal and Neonatal Safety Improvement Programme
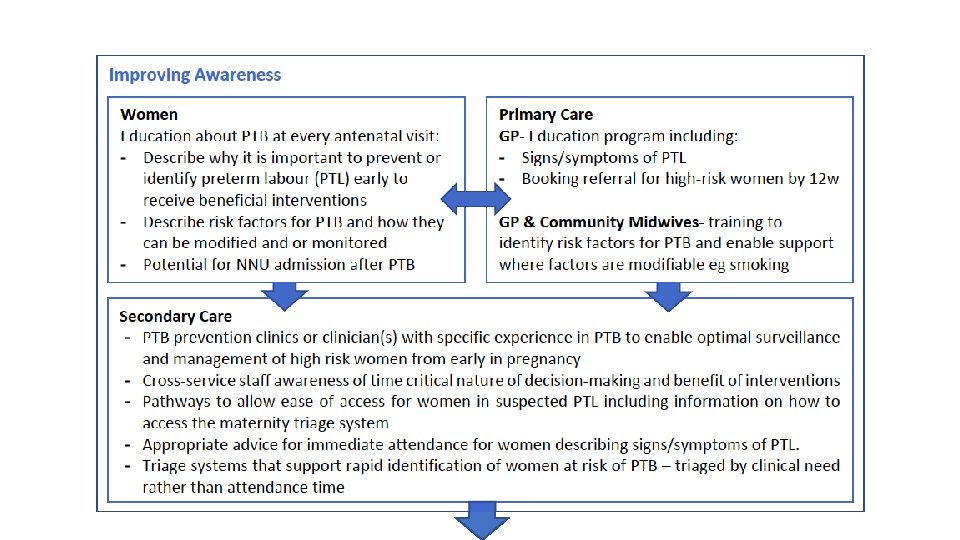
What does best practice in Antenatal Optimisation look like?
*in some situations, such as remote distance from a NICU at extreme preterm gestation, a lower QUi. PP threshold may be appropriate in prompting transfer. These decisions should be clinician-led.
Best Practice in Delivery of Antenatal Optimisation Interventions (1) General It is recommended that each unit should establish: • Obstetric, Neonatal and Midwifery leads for Antenatal Optimisation • A ‘Perinatal Team’ culture with shared goals and responsibilities • A maternity triage system such as the Birmingham Symptom-specific Obstetric Triage System to expedite assessment of women presenting acutely with symptoms of PTL • A preterm birth guideline to support the delivery of the key elements of Antenatal Optimisation • A rolling training package including simulation to ensure staff awareness of both the benefits and the need for timeliness in delivering the elements of Antenatal Optimisation. Situational awareness training using the Situational Awareness Programme for Everyone (SAFE) Toolkit may be valuable • Auditable standards and a system of exception reporting where interventions are not achieved Pharmacological interventions To ensure prompt administration of medication, consider the value of prescription templates, pre-made administration packs, stickers and checklists. Where available, practice should align with PRe. Ce. PT.
Best Practice in Delivery of Antenatal Optimisation Interventions (2) Parents • Information for parents about the risks of PTB, NNU admission and the benefit of interventions. PRe. Ce. PT, Bliss and the BAPM Extreme Preterm Framework: Helping parents to understand extreme preterm birth have useful resources • Where a woman is expected to give birth before 27 w, parental discussions should be led by senior members of the paediatric and neonatal teams and should be based on the BAPM Extreme Preterm Framework for Practice: Communication Guidance for professionals consulting with families at risk of extreme preterm delivery • Parent-held passports may aid information-sharing about interventions between different units In utero transfer To ensure efficient and effective referral and transfer processes, networks should work to establish: • A network-wide combined maternity and in utero transfer policy including reciprocal transfer • A central referral hub with defined turnaround time (auditable) for requests • Decisions about appropriateness of transfer being made by senior clinicians and supported by risk assessment tools using details of maternal and fetal wellbeing and progression of labour • Remote support for clinicians in LNU/SCUs by those in NICU settings • NICU and associated Maternity Unit policy of ‘auto-acceptance’ of in utero transfers • Guidance about staff resource and experience required to accompany in utero transfer • Guidance for Ambulance Service Partners about time critical nature of transfer
The Improvement Journey
• Understand your local data, both now and in recent past • Consider data in context of national standards/benchmarking Phase One: Define the Problem • Use one or two of the following tools to understand your data: • Forcefield analysis • Fishbone diagram • Case review • Process mapping • Pareto chart • Develop an improvement plan using a driver diagram • Learn what works by talking to high performing units • Listen to parents
Phase Two: Develop a Shared Purpose 1. Engage your team • Obstetric, Midwifery and Neonatal project leads • Parent representation • Multidisciplinary representation including • Obstetricians • Labour Ward and Theatre representatives • Midwives • Neonatologists/paediatricians • Neonatal nurses • People with QI expertise +/- a data analyst
Phase Two: Develop a Shared Purpose 2. Engage your stakeholders: Which teams need to be reached to make your project successful? • • • Parents Senior and junior obstetricians Midwives Neonatal nurses Obstetricians Theatre staff Transport team Pharmacists Sonographers Prioritise us Understand us Inform us
Phase Three: Plan and Implement Changes • Construct a Project Charter: Detail your proposed improvement, including the resources required and the potential benefits to patients Control Define Improve Measure Analyse • Formulate, prioritise and test solutions using established QI methodology, e. g: • Model for Improvement and PDSA cycles • LEAN • Six Sigma
Phase Four: Test and Measure Improvement 1. Collect the best data for your needs • Outcome measures: reflect the impact on the patient e. g. mortality, CP, IVH • Process measures: the way systems and processes work to deliver the desired outcome e. g. number of women receiving steroids or Mg; number of extreme preterm infants born in a NICU; measures of parental satisfaction • Balancing measures: this is what may be happening elsewhere in the system as a result of the change e. g. • Place of birth: number of women transferred but who do not give birth; number of women who give birth during transfer; number of low risk women who are transferred out from their primary choice of place of birth for capacity reasons; measures of labour ward and neonatal unit capacity • Antenatal steroids: number of women who receive steroids but do not give birth within a week; number of women who receive steroids but deliver at term • Antenatal magnesium: number of women who receive Mg but who deliver at term; number of delayed inductions or low risk women transferred out due to lack of labour ward capacity.
% 100 90 90 80 80 70 70 60 60 50 50 40 40 30 30 20 20 10 10 0 Average 12. 31. 21 450 Upper Confidence Limit 400 11. 3. 20 100 8. 27. 20 150 6. 10. 20 Antenatal steroids within 7 days of birth: infants <34 w 3. 12. 20 Statistical Process Control Chart 1. 13. 20 1. 1. 20 Antenatal steroids within 7 days of birth: infants <34 w окт-17 ноя-17 дек-17 янв-18 фев-18 мар-18 апр-18 май-18 июн-18 июл-18 авг-18 сен-18 окт-18 ноя-18 дек-18 янв-19 фев-19 мар-19 апр-19 май-19 июн-19 июл-19 авг-19 сен-19 окт-19 ноя-19 дек-19 янв-20 фев-20 мар-20 апр-20 май-20 Run chart Days between event of interest 100 окт-17 ноя-17 дек-17 янв-18 фев-18 мар-18 апр-18 май-18 июн-18 июл-18 авг-18 сен-18 окт-18 ноя-18 дек-18 янв-19 фев-19 мар-19 апр-19 май-19 июн-19 июл-19 авг-19 сен-19 окт-19 ноя-19 дек-19 янв-20 фев-20 мар-20 апр-20 май-20 Phase Four: Test and Measure Improvement 2. Use well-described methods to analyse and display your data: Days between chart Infant <27 w born outside an NICU 421 350 300 250 200 105 50
• Spread: • Dissemination: formal eg presentations • Diffusion: informal eg word of mouth • Exception reporting: • Case review for noncompliant cases Phase Five: Implement, Embed and Sustain • Barriers and loss of motivation: • Understand • Talk to key individuals • Observe clinical practice in action • Use a questionnaire to survey staff • Brainstorm with a focus group • Find solutions • Re-examine your change idea • Use impactful parent stories • Use lessons from high performers • Re-market your message • Use incentivisation to engage
BAPM Quality Webpages QI tools and templates Specific BAPM resources at https: //www. bapm. org/qimadeeasy • Planning your QI project • Investigating your current practice • Planning your change idea • Interpreting your data Other QI resources at BAPM QI Signpost: https: //www. bapm. org/signpost-qi-resources
NNAP Online. National Neonatal Audit Programme: Royal College for Paediatrics and Child Health Maternity and Neonatal Safety Improvement Programme: NHS Improvement Organisational standards, guidelines and initiatives Maternity and Children’s Quality Improvement Collaborative- Scottish Patient Safety Programme Saving Babies Lives’ Version 2. A care bundle for reducing perinatal mortality: NHS England; 2019 Neonatal Service Quality Indicators: Standards relating to structures and processes: British Association of Perinatal Medicine; 2017 PERIPrem Care Bundle: West of England Academic Health Sciences Network 2020 Preterm Perinatal Wellbeing Package: Maternity and Children Quality Improvement Collaborative, Scottish Patient Safety Programme. Health Improvement Scotland; Implementing the Recommendations of the Neonatal Critical Care Transformation Review: NHS England; 2019 [updated 2019. PRe. Ce. PT Resources: PRe. Ce. PT Programme. The AHSN Network Preterm Labour and Birth: National Institute for Clinical Excellence; 2019 Care of Women Presenting with Suspected Preterm Prelabour Rupture of Membranes from 24+0 Weeks of Gestation (Green-top Guideline No. 73): Royal College of Obstetricians & Gynaecologists; 2019 [Available from: