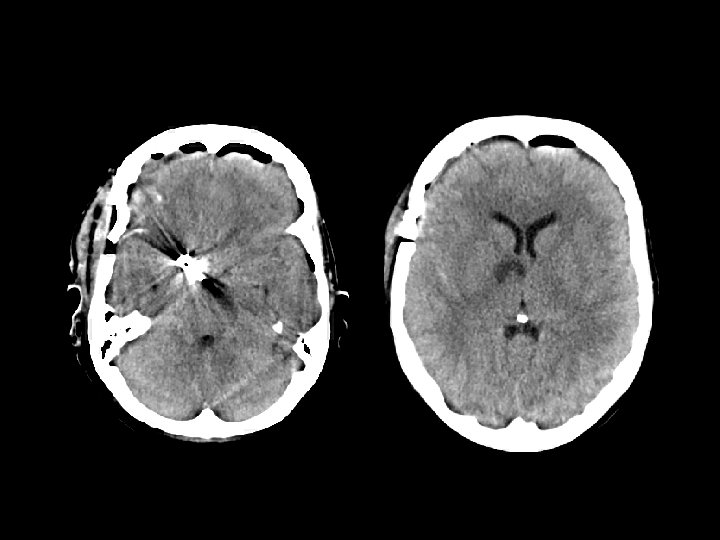
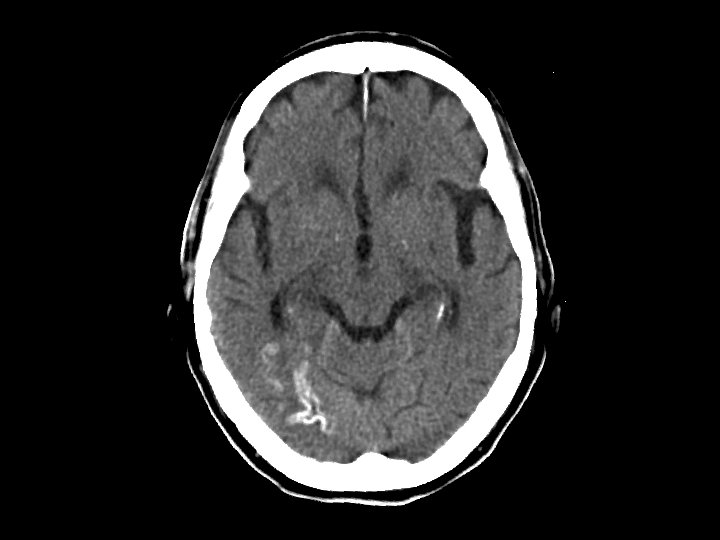
Anoxic Brain Injury Findings Hypodense cerebral hemispheres with
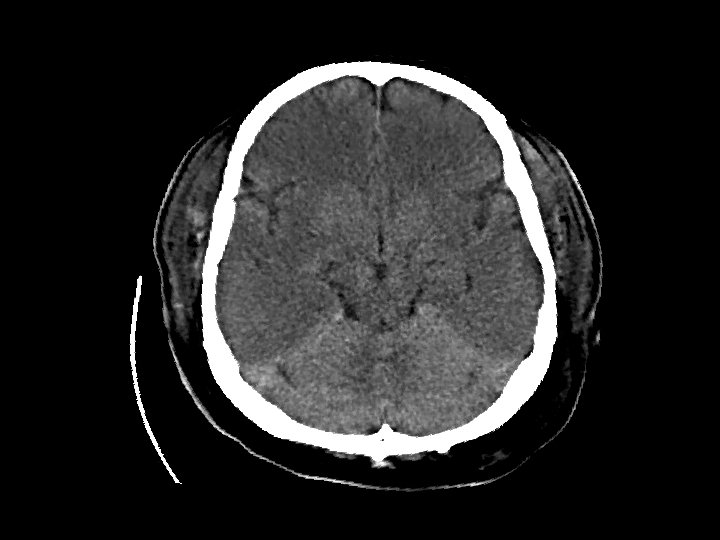

Anoxic Brain Injury • Findings: – Hypodense cerebral hemispheres with effacement of cortical gyri – Relative sparing of cerrebellum • Due to global insult: – Profound hypotension – Carbon monoxide poisoning • MRI findings: – Dense basal ganglia

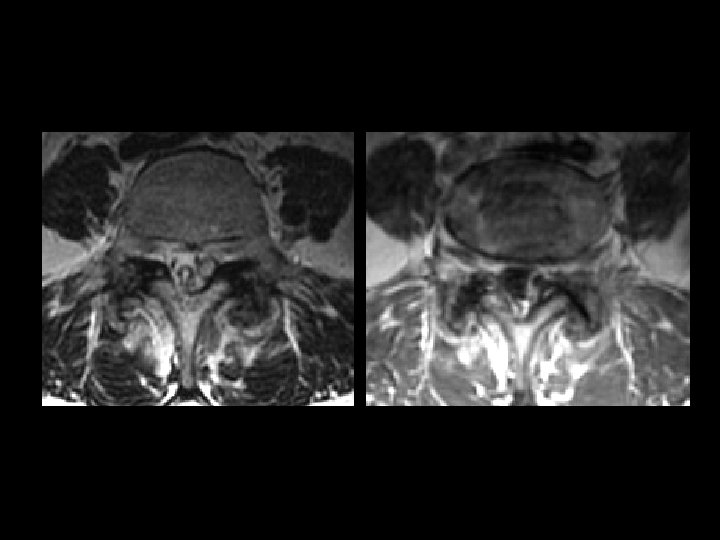

Synovial Cyst of the Lumbar Spine • • • Findings: – Low T 1, high T 2 extradural lesion contiguous with the facet joint – Surrounding enhancement – Mass effect Associated with degenerated joints – 75% at L 4 -5 Typically posterolateral Contents variable – clear fluid, calcium, hemorrhage ddx: – Migrated herniated disc – Perineural cyst (close to nerve root) – Schwannoma (low sig capsule) – Hematoma
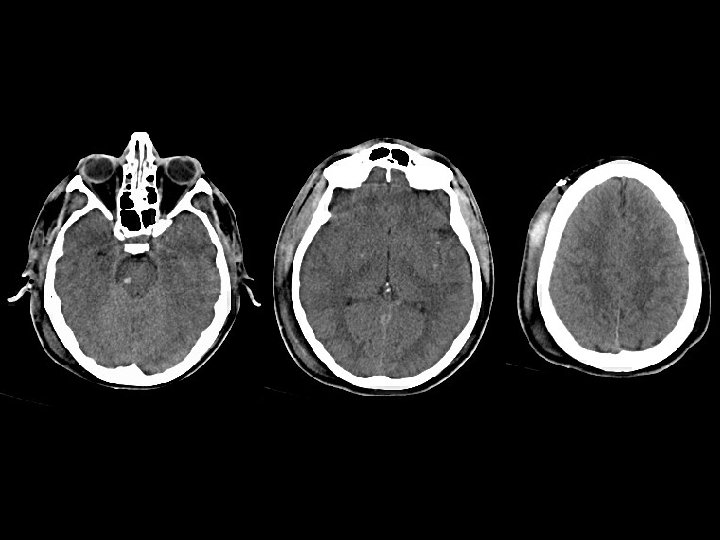

Diffuse Axonal Injury • Findings: – Diffuse brain swelling – Focal punctate hemorrhage scattered in the white matter, corpus callosum, and brain stem – Right subgaleal hematoma • Due to diffuse shearing injury, sudden deceleration (MVA) • MRI findings: – Hemorrhage best seen on GRE sequence

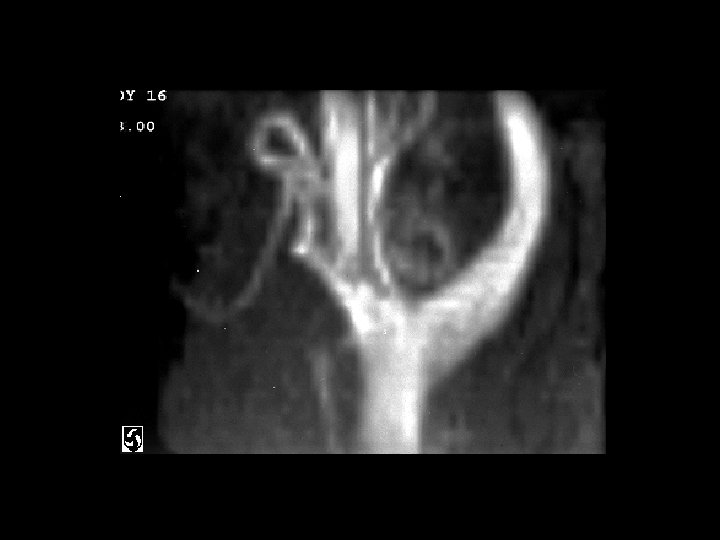
PCOM aneurysm clipping anterior choroidal artery infarct • Findings: – Recent right pterional surgery – Aneurysm clips at PCOM – Low attn at the right genu of internal capsule = infarct • Pt wakes up with hemiparesis • Devastating complication of PCOM aneurysm clipping
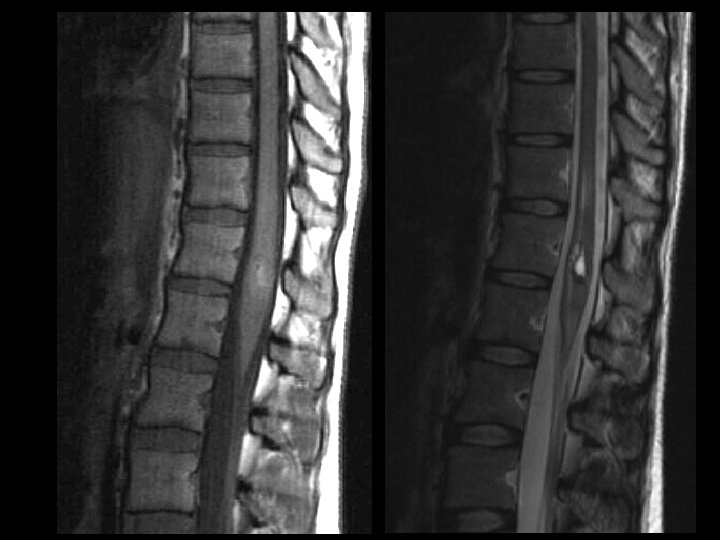

Cavernoma of the Spine • • • Findings: – “popcorn-like” intramedullary lesion in the conus – T 2: faint high signal – T 2: high signal centrally, dark rim, and high signal peripherally a. k. a. Cavernoma, cavernous hemangioma, and capillary hemangioma Congenital abnormal cluster of capillaries and venules that periodically bleed Signal characteristics are that of blood in different stages Angiographically occult Look for multiple lesions on GRE
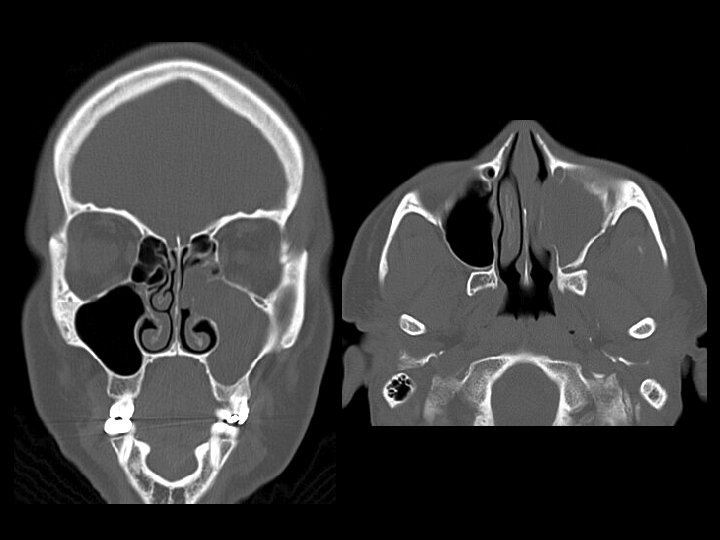

Inverting Papilloma • Findings: – Soft tissue mass involving the maxillary sinus and nasal cavity – Expansion of sinus with bone remodeling, not destruction • Benign tumors of the lateral nasal wall which extend in to the maxillary and/or ethmoid • Can homogeneously enhance • Look for widening of the infundibulum • ddx: – Antrochoanal polyp – Mucocele
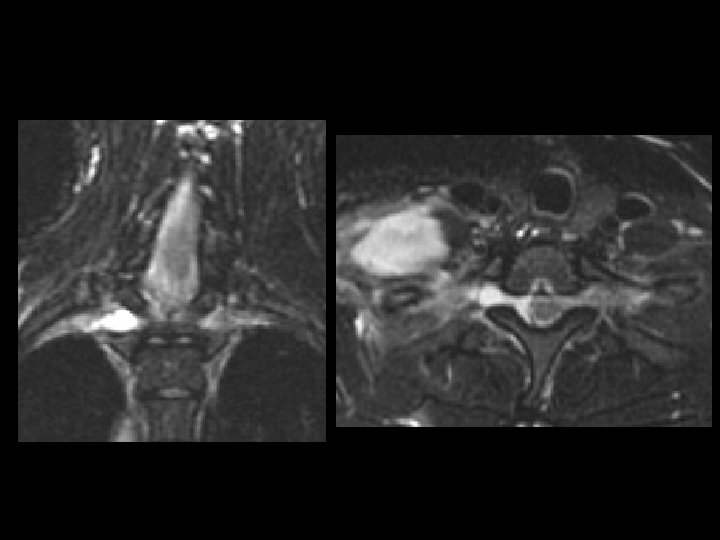

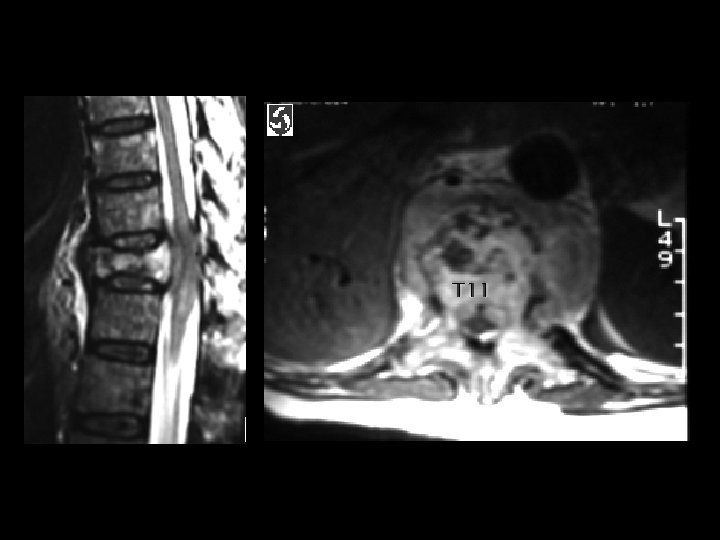
Nerve root avulsion and pseudomeningocele • Findings: – Abnormal high T 2 signal dumbbell-shaped lesion in a high thoracic neural foramen – Mass effect on thecal sac – Large high T 2 collection in the adjacent soft tissues • A result of major trauma • Disruption of the meninges and spill of CSF into surrounding tissues • Focal collection at the nerve root may appear as a discrete mass and displace thecal sac
 • HSV")
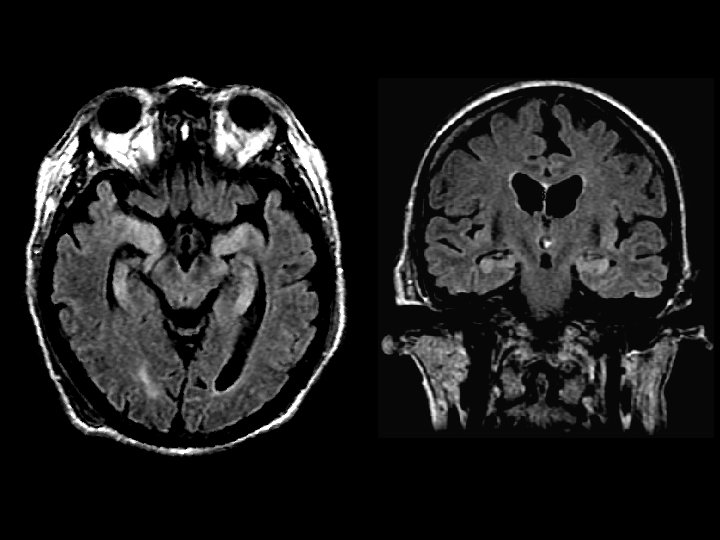
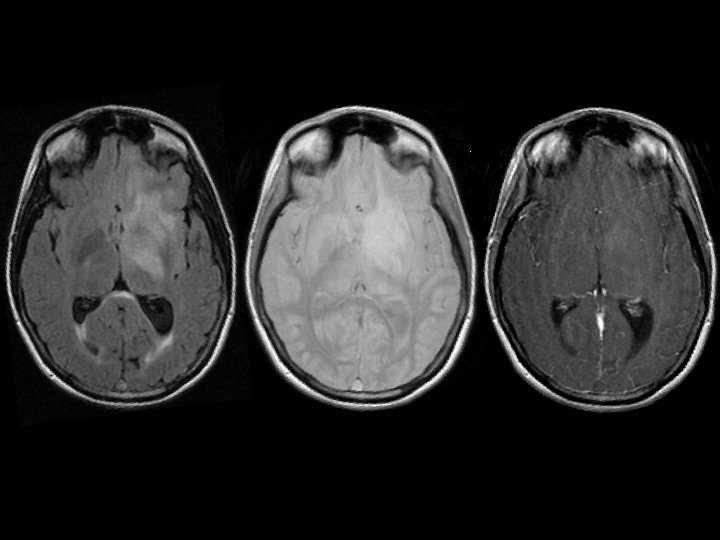
Herpes Encephalitis • Findings – Bilateral temporal lobe FLAIR signal (postseizure edema) • HSV 2 in neonates • HSV 1 in adults – latent infection in the Gasserian ganglion (CN V) – predilection for the limbic syste, cingulate gyrus, and subfrontal region – late stage becomes bilateral, hemorrhage

Cortical Laminar Necrosis • Findings: – Cortical calcification of the posterior right MCA territory • Due to infarction • If global, think of hypoxic injury, hypoglycemia, or encephalitis

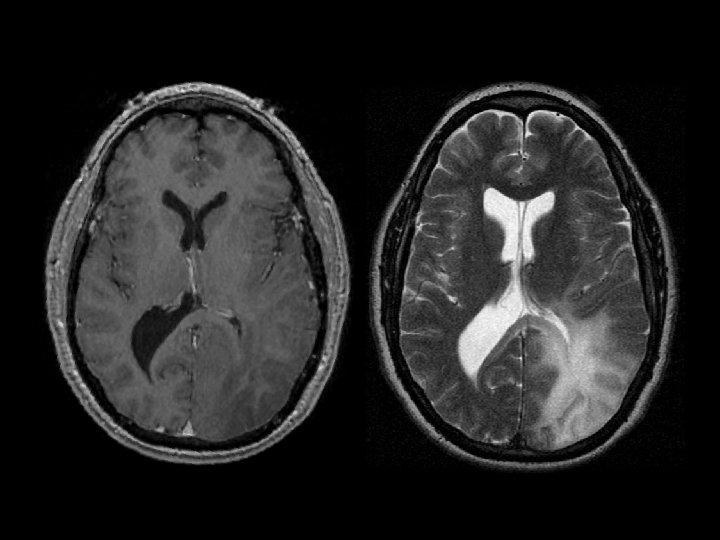
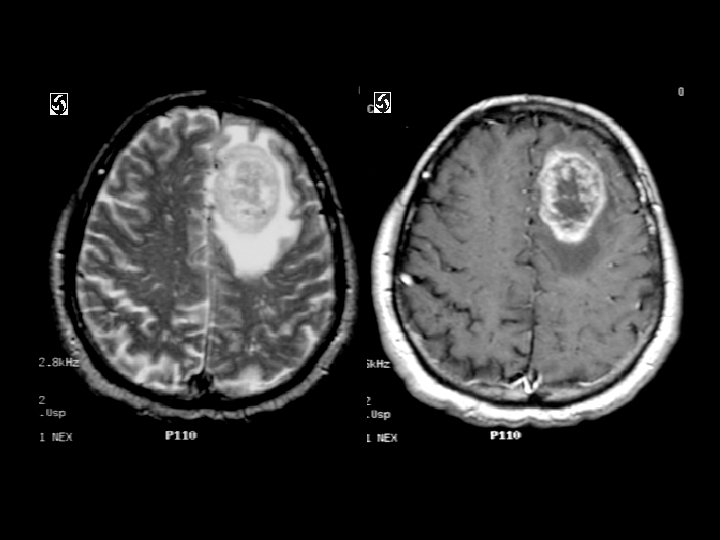
Primary Intracerebral Lymphoma • Findings: – T 2 bright lesion in the left frontal lobe and basal ganglia – Crosses both gray and white matter – Some mass effect – No significant enhancement • An unusual lesion in the non. HIV/immunosuppred population • ddx: – Low –grade glioma

Spinal Sarcoid • Findings: – Iso T 1, hyper T 2, enhancing lesion of cervical spinal cord – No significant cord expansion • Idiopathic system disease characterized by noncaseating granulomas • Young, black women • Image the brain, check CXR • ddx: – Transverse myelitis – Demyelinating dz (MS) – Primary cord tumor (ependymoma, astrocytoma) – Met (uncommon)

Septic Sacroiliitis • • • Findings: – Low T 1, high T 2 abnormality in the right SI joint Uncommon infection usually due to strep ddx: – Unilateral • Gout • Osteoarthritis – Bilateral & symmetric • Ankylosing spondylitis • Inflammatory Bowel Dz – Bilateral & asymmetric • Psoriatic arthritis • Reiter syndrome • Rheumatoid
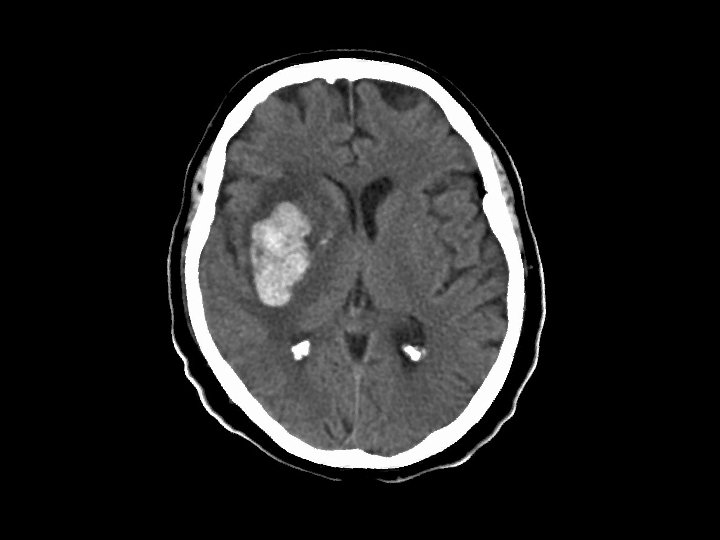

MCA hemorrhagic infarction • Findings: – Large hemorrhage in the right insula – Much surrounding edema – Some mass effect • Due to M 1 segment embolus affecting lateral lenticulostriate arteries • ddx: – Hypertensive hemorrhage (usually little or no edema) – Underlying tumor or AVM (need angio to confirm)


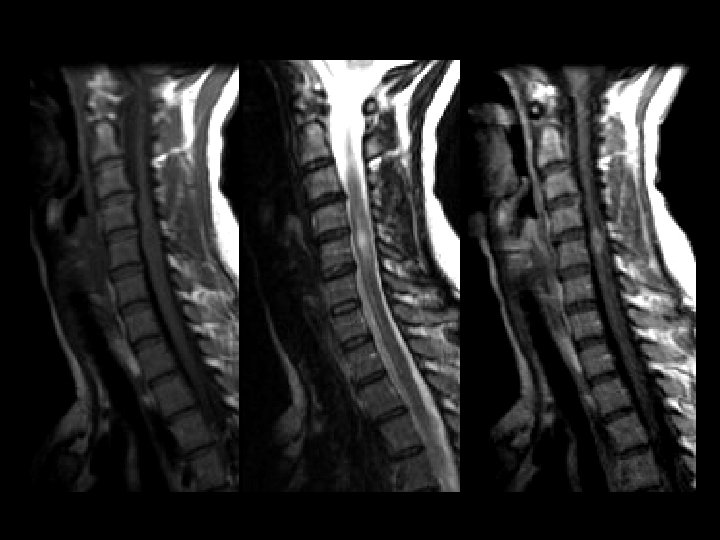
Spinal Multiple Sclerosis • Findings: – Cord edema – Flame-shaped intramedullary enhancement – No significant cord expansion • Image the brain, check the optic nerves • ddx: – Transverse myelitis – Sarcoid – Primary cord tumor – Mets

Sacral Insufficiency Fracture • Findings: – High T 2 signal in the left sacral ala crossing the midline and involving the right side • Normal stress on abnormal bone (usually osteoporosis) • Pts can have non-specific back or hip pain • Plain films show lucency, then sclerosis • Bone scan show classic “Honda sign” • ddx: – acute fractures – metastases
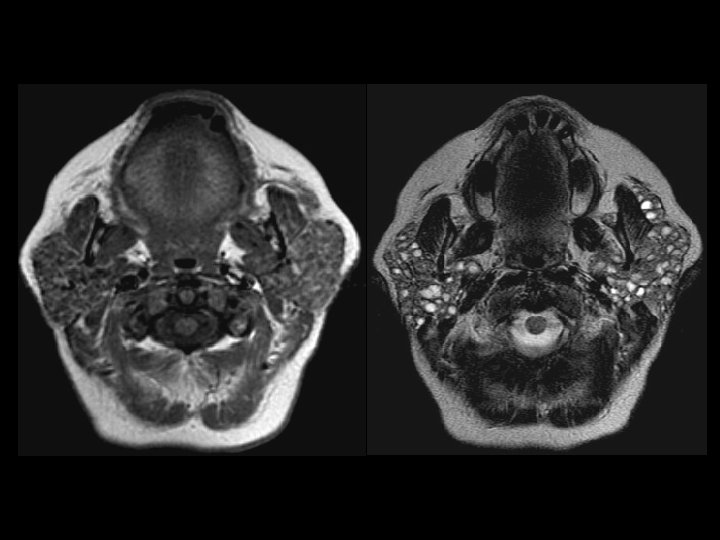

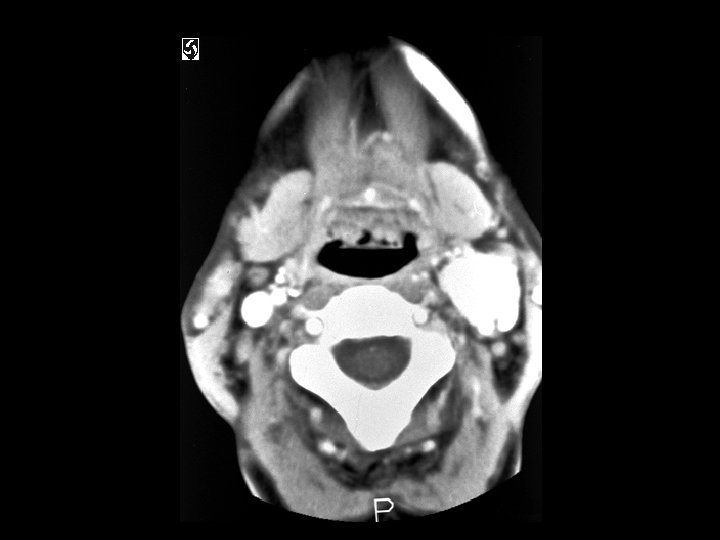
Lymphoepithelial cysts in HIV • Findings: – Enlarged parotid glands containing innumerable small cystic lesions • Manifestation in HIV, unclear etiology • Soft, non-tender enlarged glands • ddx: – Sjogren’s syndrome – Warthin’s tumors


TB meningitis • Findings: – High attenuation of the cerebellar folia • Look for the primary site (lungs); usually a post-primary infection • Long and protracted illness rather an typical sx of acute bacterial meningitis • Look for BASAL involvement • ddx: – Carcinomatous meningitis – Sarcoidosis – Lymphoma – Subarachnoid blood

Anaplastic Astrocytoma • Findings: – Ill-defined T 2 signal abnormality involving both gray and white matter – Crosses vascular territories and into corpus callosum – Mass effect on ventricle • The most common primary brain tumor • Tumor margin likely beyond T 2 boundary • Don’t let lack of enchancement fool you!


Spinal Dural AVF • Findings: – Expanded, edematous cord – Multiple extramedullary high signal foci • Direct AV communication leads to venous hypertension, cord congestion, and infarction • Extramedullary AVFs DO NOT bleed • Intramedullary AVMs have a nidus, present in kids as acute paresis due to spontaneous hemorrhage • ddx: – Leptomeningeal carcinomatosis
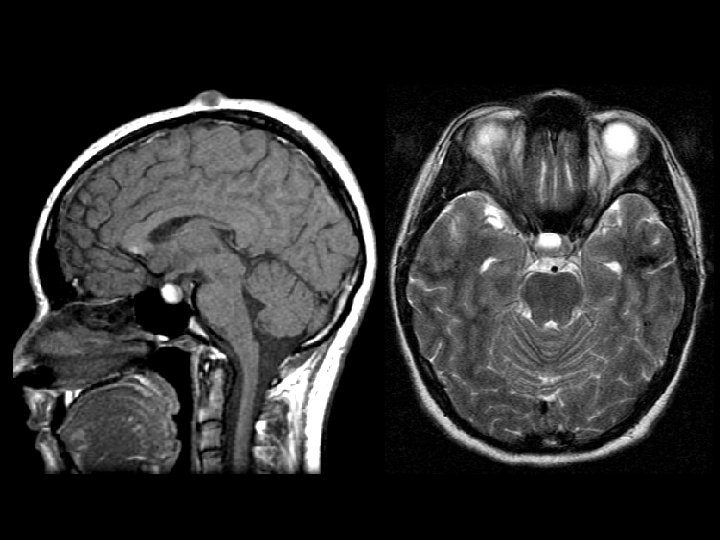
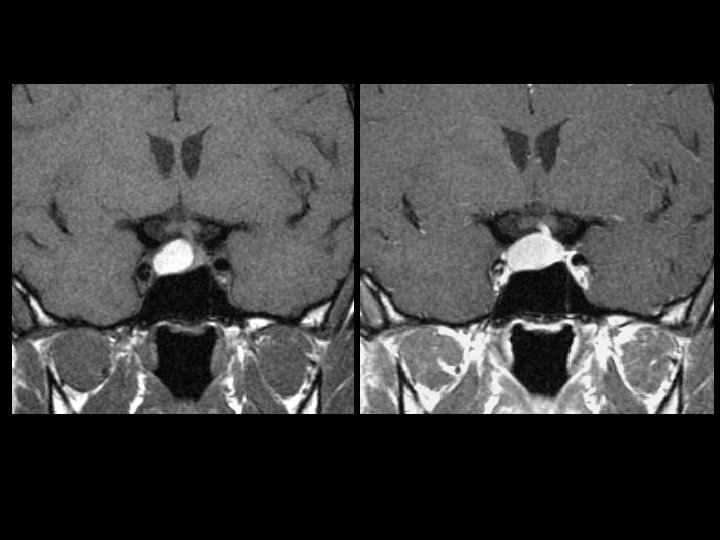

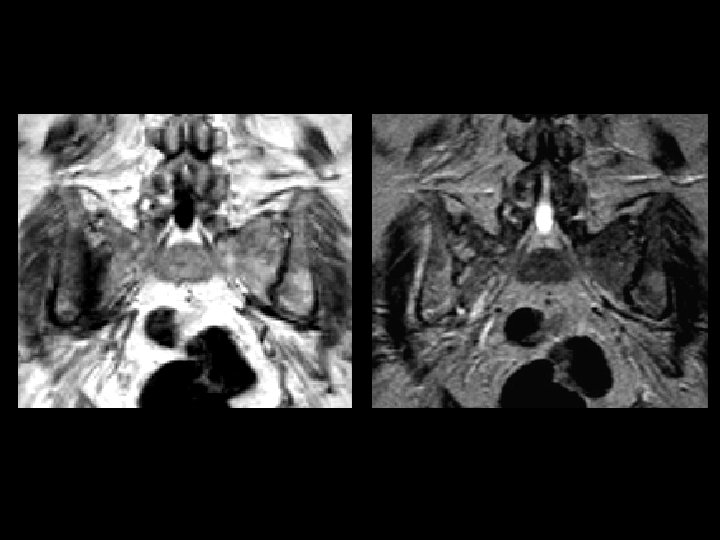
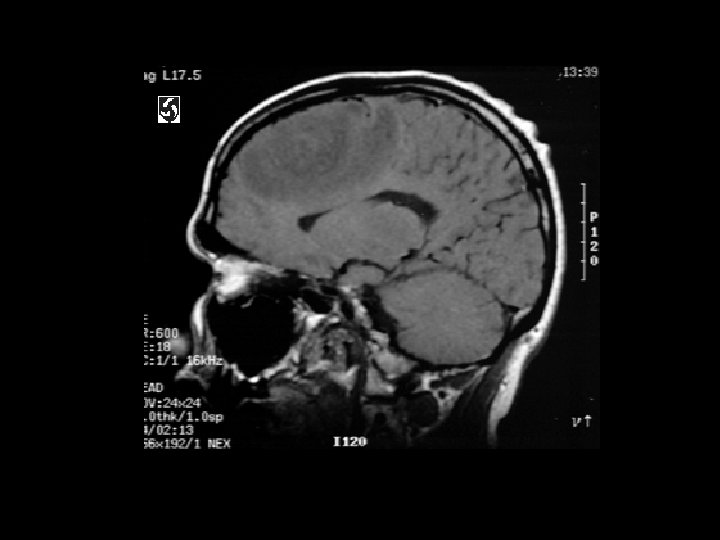
Rathke’s Cleft Cyst • Findings: – High T 1 & T 2 slightly expansile sellar lesion – Displaces normal pituitary tissue • Non-neoplastic remnants of Rathke’s pouch • majority are asymptomatic, symptoms include visual defects, pit insufficiency, headaches • Can be high or low T 1 but always high T 2 • Ddx: – Arachnoid cyst – Epidermoid – Pituitray adenoma – craniopharyngioma

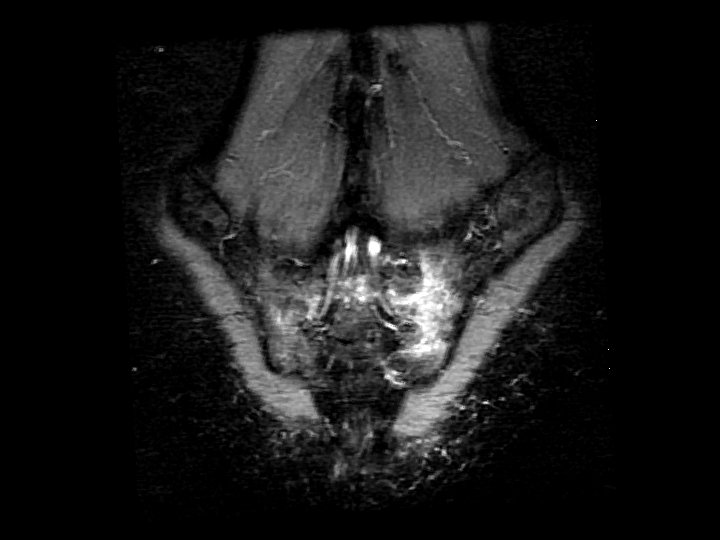
Carotid body paraganglioma • • Findings: – Intensely enhancing mass in the carotid sheath that splays the internal and external carotid arteries ddx: – Glomus vagali – Carotid aneurysm

Glioblastoma multifome • Findings: – Aggressive intra-axial enchancing mass lesion with central necrosis • ddx: – Abscess – Tumafactive MS

Pathologic compression fracture & cord compression • Findings: – Compression of T 11 with retropulsion and cord compression – Diffuse abnormal signal in the visualized vertebrae • Causes: – Metastases – Multiple myeloma

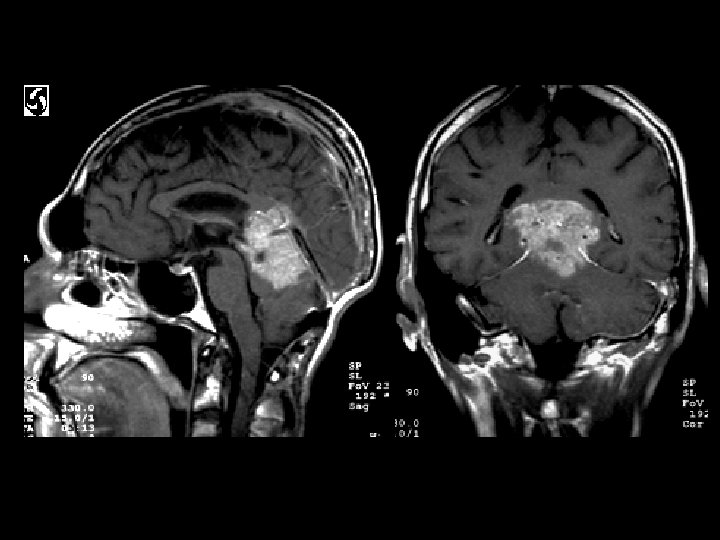

Pinealoblastoma • Findings: – Large, aggressive, enhancing lesion of the pineal region • ddx: – Germinoma – High grade glioma – Metastasis
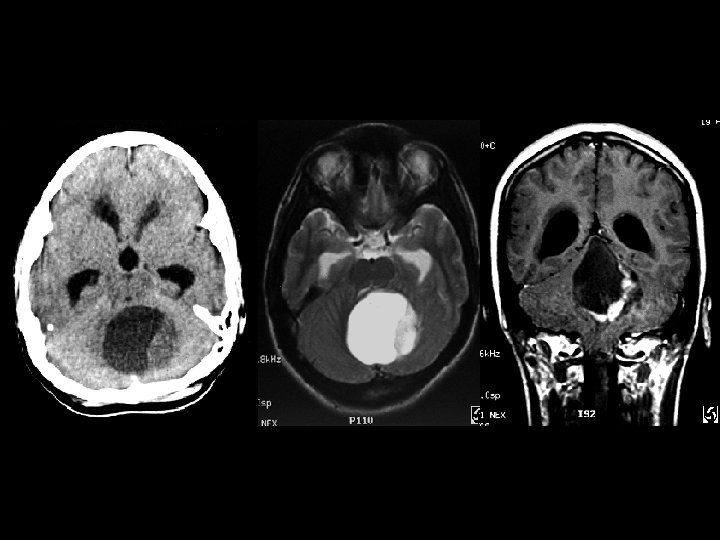

Juvenile Pilocytic Astrocytoma • Findings: – Cystic cerebellar lesion with enhancing mural nodule – Obstructive hydrochephalus • ddx: – Hemangioblastoma (in adults = think VHL)
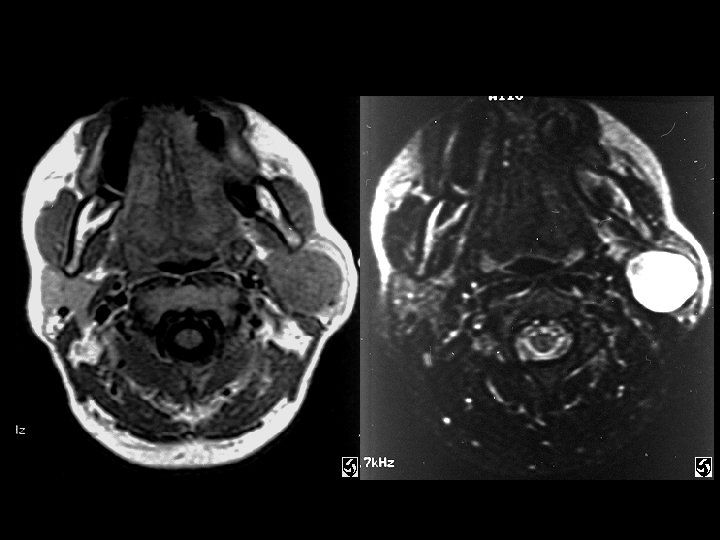

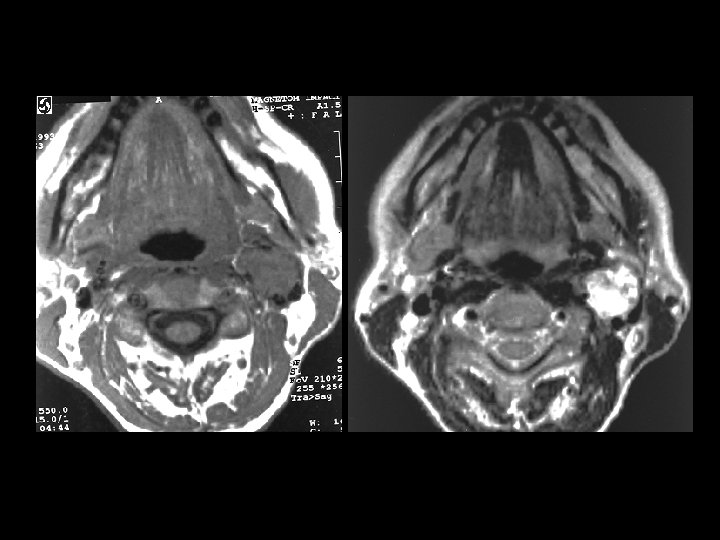
Parotid pleomorphic adenoma • Findings: – Intensely bright T 2 parotid lesion • ddx: – Adenoid cystic tumor – Mucoepidermoid – hemangioma
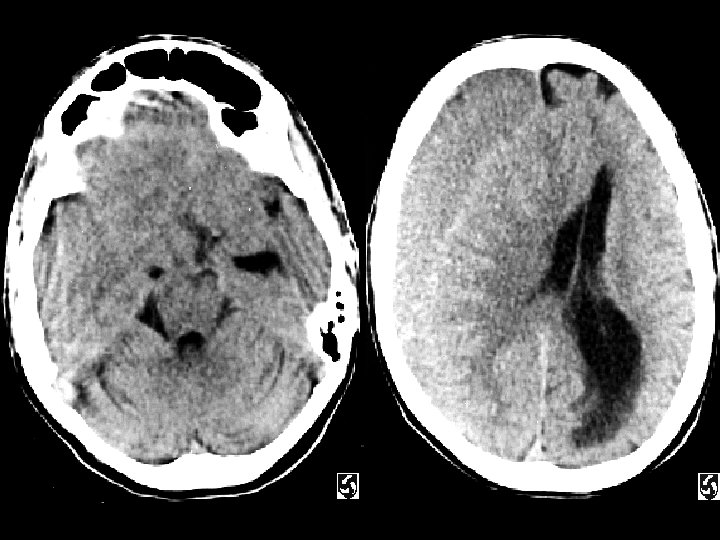

Isodense subacute subdural hematoma • Findings: – Isodense subdural hematoma – Much mass effect • ddx: – Hyperacute hemorrhage
- Slides: 60