Anomalies in the Development of the Dentition Natal







")













 • • • An aberration in the")
 • When ankylosis is minor or questionable,")







")
")




 Mild Fluorosis: Found in ± 6% of children Moderate Fluorosis: Found")


")
 • Inherited in an autosomal dominant pattern. • A")

- Slides: 46
Anomalies in the Development of the Dentition
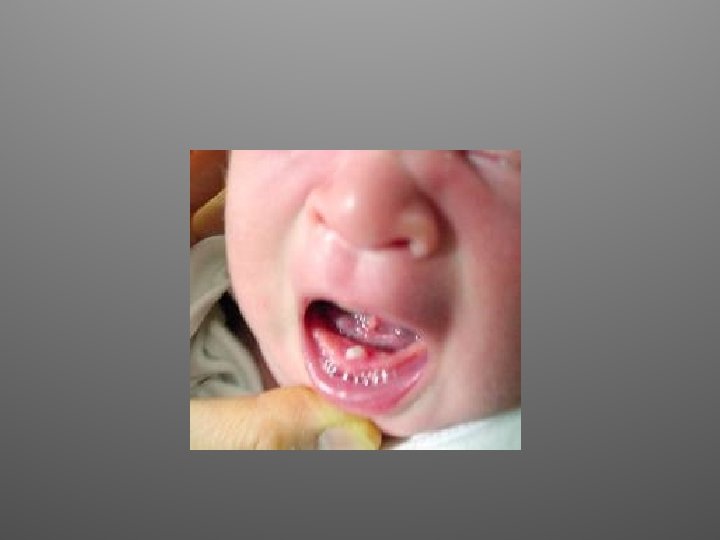
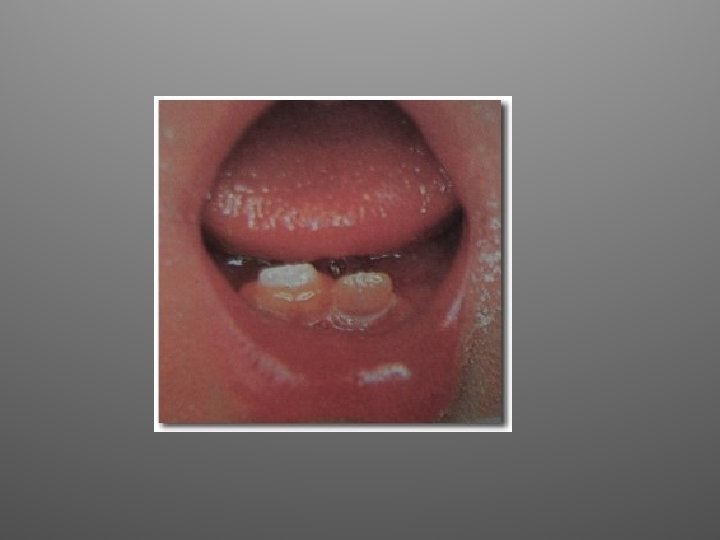
Natal and Neonatal Teeth
Definitions and Prevalence • Natal Teeth: Teeth that are erupted at birth. • Teeth Neonatal: Teeth that erupt during the period of early infancy shortly after birth; typically characterized as within 30 days. • Natal/Neonatal Teeth occur in approximately 1 in 3, 000 births. • Typically they are mandibular incisors. • In 90% of the cases they are prematurely erupted primary teeth, not supernumeraries.
Treatment • Due to the overwhelming prevalence of the teeth being prematurely erupted teeth, they should be preserved. • If it can be determined (by radiograph) that they are supernumerary, then should be extracted. Supernumerary natal and neonatal ‘teeth’ appear to be calcific nodules that do not have the morphological appearance of a primary tooth. • Typically are somewhat mobile due to immature root formation. • Physicians and nurses will frequently ask that they be extracted due to concern about become dislodged with swallowing or aspiration. Also concern regarding interfering with nursing. • Unless it is determined that the natal/neo-natal teeth are supernumerary, pressure to extract should be resisted, as the teeth are more resistant to dislodging than thought. Teeth are typically not an impediment to nursing as mothers’ nurse their infants for a considerable period subsequent to the eruption of all of the incisor teeth.
Eruption Hematoma • Eruption hematoma’s are sometimes referred to as an “eruption cyst. ” • Essentially a dilatation of the normal follicular space around the crown of the erupting tooth caused by the accumulation of tissue fluid or blood. • Most commonly occur with eruption of primary teeth, although also noted with eruption of first permanent molars. • No therapy is required.
Cysts Inclusions of the Newborn • Inclusion cysts of the newborn infant are of two types. • Bohn’s nodules are smooth whitish cysts of 1 -3 mm in size filled with keratin. They are found on the buccal and lingual of the dental ridges and are the result of cystic degeneration of epithelial rests of the dental lamina. They are benign and usually disappear within the first three months of life. • Epstein’s pearls are small cystic vesicles of 1 -3 mm in size seen in the medial palatal raphe of newborn infants—they are commonly present. They are caused by the entrapment of epithelium during the development of the palate. They resolve spontaneously and do not require treatment.
Bohn’s Nodules Epstein Pearls
Fusion and Gemination (“Double Teeth”)
Definitions • Fusion is defined as a the conjoining of two teeth. When the teeth are counted and the anomalous tooth is counted as one, a tooth is missing. • Gemination is defined as ‘two teeth’ developing from one tooth bud, and when the teeth are counted the individual is not missing a tooth. • Counting the teeth is critical to determining whether the anomalous tooth is fused or geminated.
Fusion of Primary Teeth Prevalence of fusion is estimated to be between 0. 5% and 2. 5% in the primary dentitions. It is seen much less frequently in the permanent dentition.
Gemination Geminated and fused primary teeth are essentially phenomenon related to primary anterior teeth. Generally no treatment is required, though decay may occur if a crevice exists in the “double tooth. ” Additionally, if the root is involved, thus larger than normal, and is delaying the eruption of the succedaneous tooth, the primary tooth may have to be extracted. Anomalies exist in permanent incisors approximately 50% of the time when there anomalies of the primary incisors. (Gellin)
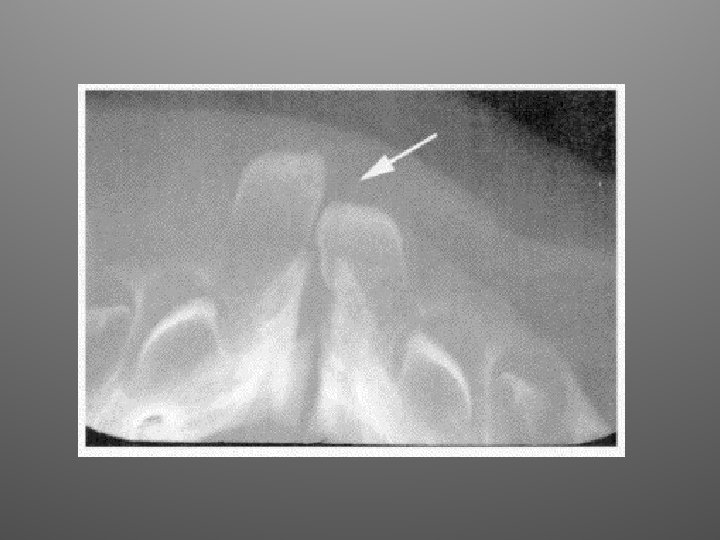
Ectopic Eruption of First Permanent Molars
Definition and Significance • A condition in which the permanent first molar assumes a path of eruption that intercepts the distal root of the second primary molar causing its resorption with the potential to cause premature of the second primary molar. • Problematic that in doing so there is a loss of arch circumference ultimately compromising the eruption of the second premolar.
Characteristics and Prevalence • Ectopic eruption of the first permanent molar occurs in 2 -4% of the population. • Most common in the maxillary; relatively infrequent in the mandibular arch. • Associated with inadequate arch circumference—typically the lower incisors will be “crowded. ” • Self-correction occurs in approximately 66% of the cases. • Generally requires appliance intervention if not self-corrected by age 7.
Ectopic Eruption
Halterman Appliance Correction
Halterman Appliance • Primary molar band is fitted on second primary molar. • If a primary molar band is not maintained in the office, the occlusal surface can be cut of a stainless steel crown that fits the tooth and used as alternative. • A compound impression with the band in place is then sent to a laboratory such as “Space Maintainers Laboratory (information for submission on the internet) with instructions to fabricate a Halterman Appliance. • On return an orthodontic button is attaced to the occlusal of the partially erupted first permanent molar through acid etching and adhesion with a resin; the Halterman appliance is cemented to the second primary molar; and a orthodontic elastic chain is stretched over the button engaging the loop in the Halterman Appliance. • Child should be seen in one week with elastic changed, and every 2 -3 weeks until correction has occurred; varying from 4 -12 weeks,
Subsequent to Correction While the pulp typically is involved, rarely does pulpal necrosis occur and the second primary molar remains in place until eruption of the second premolar.
If Not Corrected, Arch Circumference Lost with Molar Shifting Forward
If Not Treated and Arch Circumference is Lost, Head Gear Necessary to Regain Lost Space
NO Space Maintainer • Do not place a space maintainer after the first permanent molar has already migrated forward and space has been lost! • Space maintainers are only to be used for maintaining adequate space. • Once space is lost a space regainer is required.
Infra-occlusion of Primary Posterior Teeth (Submersion, Ankylosis) • • • An aberration in the eruption of teeth in which the continuity of the periodontal ligament becomes compromised during bone remodeling during growth of the alveolus, with fusion of the cementum and bone at one or more locations/teeth do not move with the continuing vertical growth of the alveolar arch. Results in the tooth being in infraocclusion or “submerged” relative to the occlusal plane. Prevalence 3 -4%, with mandibular first primary molar most commonly ankylosd, and typically between 7 -11 years of age.
Infra-occlusion of Primary Posterior Teeth (Submersion, Ankylosis) • When ankylosis is minor or questionable, can be diagnosed by a dull sound on percussion of the tooth. • One study found that only 3 -4% of ankylosed primary molars did not exfoliate normally and required extraction. • However, due to adjacent posterior tooth tipping into the space, a full arch space maintainer (lingual arch or Nance arch) must be placed to preserve arch circumference. Do not permit the infraocclusion to go past the point of proximal contact.
Mesiodens • Most common supernumerary tooth; defined as supernumerary existing in the maxillary midline. • Prevalence is up to 2% of population. • Can interfere with eruption of permanent central incisor(s).
Mesiodens • Only approximately 25% of mesiodens erupt. • Majority are conical in shape, vertically aligned and positioned to the palatally. • Timing of surgical removal is critical with tension between not adversely affecting permanent incisor tooth bud, and not interfering with the normal eruption of the incisor.
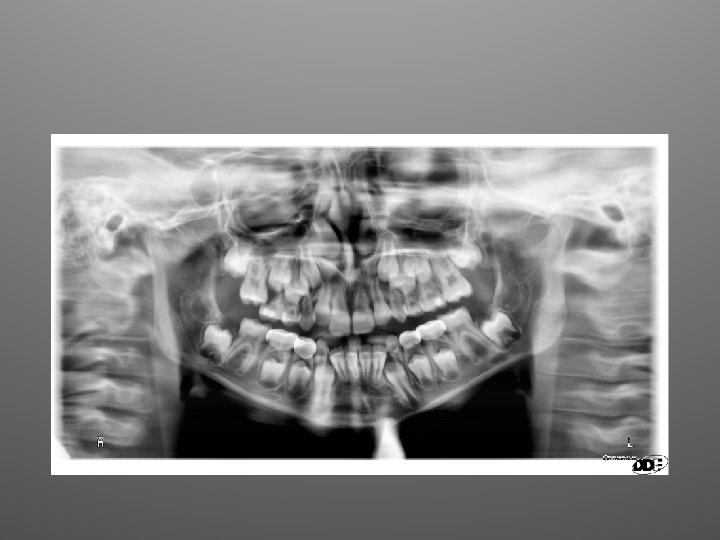
Congenital Agenesis of Teeth • Hypodontia refers to the congenital absence of one to five teeth excluding the third molars. • Oligodontia refers to the congenital absence of six or more teeth excluding third molars. • Anodontia refers to the complete absence of permanent teeth. • Meta-analysis of the research literature indicates that mandibular second premolars are most commonly missing tooth (± 3. 0%), followed by the maxillary lateral incisor (1. 0 -2. 0%). and the maxillary second premolar (1 -1. 5%).
Agenesis of Second Premolar • • • Second Primary Molar can frequently be maintained for an indefinite period of time. Management must be based on overall assessment of occlusal development. One study found that only 7 of 59 retained primary molars were lost between 12 and 20 years of age, and none after age 20 during the observation period. Sound prevention practices critical to preservation of the tooth. Frequently, the primary molar becomes ankylosed creating the potential for loss of arch circumference, and must be extracted. If orthodontics is required the teeth may be sacrificed. If lost later in life, an implant may be employed to replace the missing tooth.
Agenesis of Maxillary Lateral Incisor • Management can be complex. • Options include: – Substituting the canine for the lateral with reconturing of the canine. Orthodontic movement may be required achieve the most favorable esthetic result. – Orthodontic movement to permit prosthetic replacement initially with resin-retained prosthesis (Maryland Bridge) ; ultimately replacement with an implant and crown.
Anomalies of Morphodifferentiation
Peg Shaped Teeth
Hutchinson’s Incisors of Congenital Syphilis (Morphodifferentiation and Apposition)
Mulberry Molars of Congenital Syphilis (Morphodifferentiation and Apposition)
Dens in Dente or dens invaginatus is a malformation of teeth most likely resulting from an infolding of the dental papilla during tooth development or invagination of all layer of the enamel organ in the dental papillae. Teeth most affected are maxillary lateral incisors and bilateral occurrence is not uncommon. The malformation shows a broad spectrum of morphologic variations and frequently results in early pulpal necrosis. Root canal therapy may present severe problems because of the complex anatomy of the teeth.
Taurodontism is a condition found in the molar teeth of humans whereby the body of the tooth and pulp chamber is enlarged vertically at the expense of the roots. As a result, the floor of the pulp and the furcation of the tooth is moved apically down the root. The underlying mechanism of taurodontism is the failure or late invagination of Hertig’s epithelial root sheath, which is responsible for root formation and shaping causing an apical shift of the root furcation.
Dilaceration
Anomalies of Apposition
Fluorosis (Mottled Enamel) Mild Fluorosis: Found in ± 6% of children Moderate Fluorosis: Found in ± 1 -2% of children Severe Fluorosis Found in ± 1% of children
Amelogenesis Imperfecta
Amelogensis Imperfecta • Literally, imperfect enamel formation. A defect of amelogensis. • Prevalence 1 in 700 to 1 in 15, 000. • Four types: Hypoplasitic--a defect in the amount of enamel; Hypomaturation-- defect in maturation of enamel; Hypocalcified—defect in initial crystal formation; Hypomaturation/Hypoplastic. • Various types present various clinical appearances. • Transmitted as Autosomal Dominant (50% of offspring affected); Autosomal Recessive (25% of offspring affected ); and X-linked recessive (no male transmission; all daughters carriers—with 50% of their offspring affected). • Fourteen different mutations of gene.
Dentinogenesis Imperfecta (Hereditary Opalescent Dentin)
Dentinogenesis Imperfecta (Hereditary Opalescent Dentin) • Inherited in an autosomal dominant pattern. • A defect in dentinogensis. • Prevalence estimated at 1 in 6, 000 to 8, 000 individuals. • Type I can occur as a recessive trait with osteogenesis impefecta. Teeth most severely affected are primary teeth versus permanent. • Type II occurs without other inherited disorders; both dentitions equally affected. • Pulp chambers become obliterated.
Molar-Incisor Hypomineralization • Molar-incisor hypomineralization describes the clinical picture of hypomineralization of systemic origin affecting one or more first permanent molars that are associated frequently with affected incisors. • Etiological associations with systemic conditions or environmental insults during the child's first 3 years have been implicated. • Prevalence studies highly variable from 6% to 25% • Management: Early diagnosis, sealants, stainless steel crowns, bleaching, composites.