Anesthetic management of a patient requiring placement of




, HTN(-), other systemic dz. (-)")

, thrill(-), heave(-) Abdomen:")
 RBC: 4. 09 l Hb:")
 PT: 11. 8/11. 5 l PTT: 39. 8/35. 5")





















- Slides: 34
Anesthetic management of a patient requiring placement of a Y- stent Presented by 林起翎 蔡鵠遠 戴家煌
Brief History 呂xx, 61 y/o, male Persistent dry cough since 3 yrs ago. Dyspnea and wheezing on left side down. Tuberculosis was diagnosed at 署立新竹H. He started to receive regular medical therapy. CXR showed a granuloma at LUL on OPD follow-up in Aug. 2001.
He was transferred to Dr. 李元麒‘s OPD in Oct. 2001. Echo-guide biopsy was performed. Pathology report revealed tuberculosis. Sputum culture yielded “Mycobacterium gordonae” in March, 2002. Chest CT-scan showed persisted granuloma in May, 2002.
Left main bronchus stenosis was noted. Tracheostomy with left main bronchus dilation was done first on 10/3, 2002. Stenting for left main bronchus was inserted on 10/21, 2002. Productive cough with massive sputum was noted after he was discharged on 10/26. He was admitted again and bronchoscope revealed granulation tissue over distal end of the stent on 11/8. Arrange Y-stent on 11/11.
Past History Old MI at 4 years ago DM(-), HTN(-), other systemic dz. (-) No known food or drug allergy Smoking(+), quitted for 3 yrs Alcohol(-), betel nut(-) Family history:non-contributory Previous operation history:tracheostomy and stenting
Physical Examination Consciousness: clear, E 4 M 6 V 5, easy-looking Vital signs: BP=115/75 mm. Hg, HR=68/min, RR=20/min, BTR=37. 0℃ HEENT: conjunctiva: not pale, sclera: anicteric, pupil: isocoric, prompt light reflex L/R: +/+ Neck: supple, JVE(-), LAP(-), carotid bruit(-), tracheostomy(+)
Chest: L’t side decreased breathing sound Heart: Regular heart beat, murmur(-), thrill(-), heave(-) Abdomen: soft and flat, tenderness(-) Extremities: freely movable, pitting edema(-) Peripheral pulsation: intact 51. 6 kg, 156. 4 cm
Laboratory data Complete Blood Cell Count (91 -11 -07) RBC: 4. 09 l Hb: 12. 7 l Hct: 36. 3 l HCV: 88. 8 l MCHC: 35 l PLT: 466 l WBC: 7360 l
Coagulation Profile (91 -11 -07) PT: 11. 8/11. 5 l PTT: 39. 8/35. 5 l Blood Biochemistry (91 -11 -07) Albumin: 4. 06 l Globulin: 3. 63 l Bilirubin(T): 0. 3 l Bilirubin(D): <0. 1 l
ALP: 196 Na: 138 l AST: 21 K: 3. 65 l ALT: 111 Cl: 96 l BUN: 10. 9 Ca: 2. 31 l Creatinine: 0. 96 l Glucose AC: 105 l
EKG: normal sinus rhythm, Q wave at V 1~3 CXR: left apical fibrotic change
Anesthesia IVA
Monitor EKG , BP , A line , 2 IV line end-tidal CO 2 , pulse oxymeter Urinary output
Induction: Fentanyl: 1 ml Pentothal: 250 mg Atracurium: 25 mg Xylocaine: 100 mg Robinul: 0. 2 mg Nitroderm: 1 TTS Vitacal: 1 amp Maintenance: IV propofol infusion: 50~100 mg/h
Problem Tube without seal air leakage Øno gas anesthesia Øventilation efficiency Sa. O 2 Pa. CO 2 Left bronchial stenosis
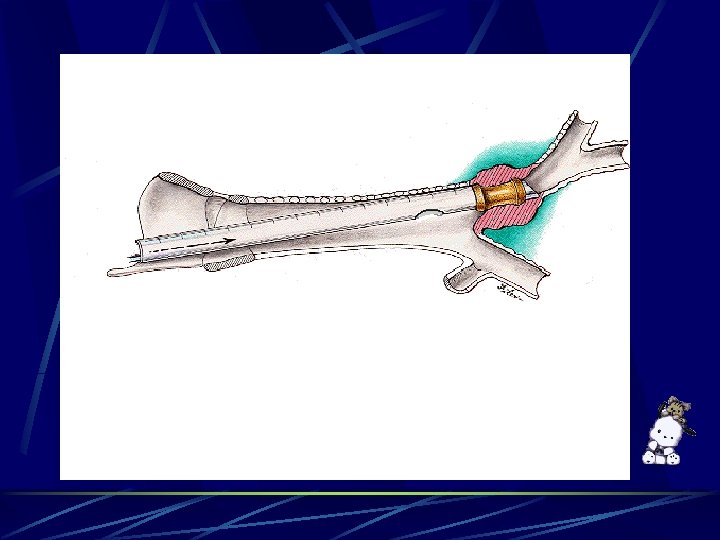
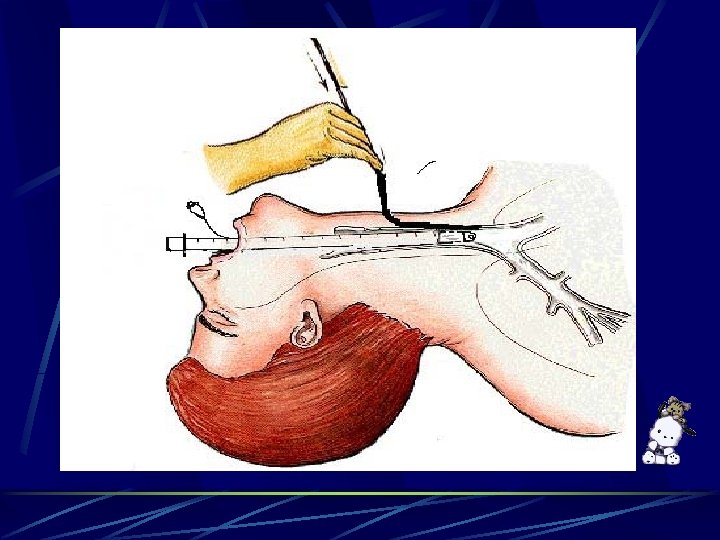
procedure dilated the left main bronchus check the lesion of left main bronchus with flexible scope measure the length to insert Y stent
Problem Tube without seal air leakage Øno gas anesthesia Øventilation efficiency Sa. O 2 Pa. CO 2 Irritation of airway Ølaryngospasm, bronchospasm ØHR BP
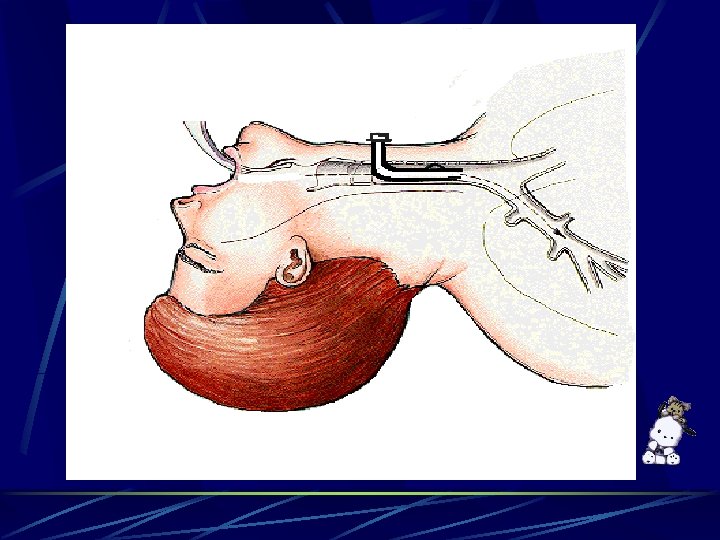
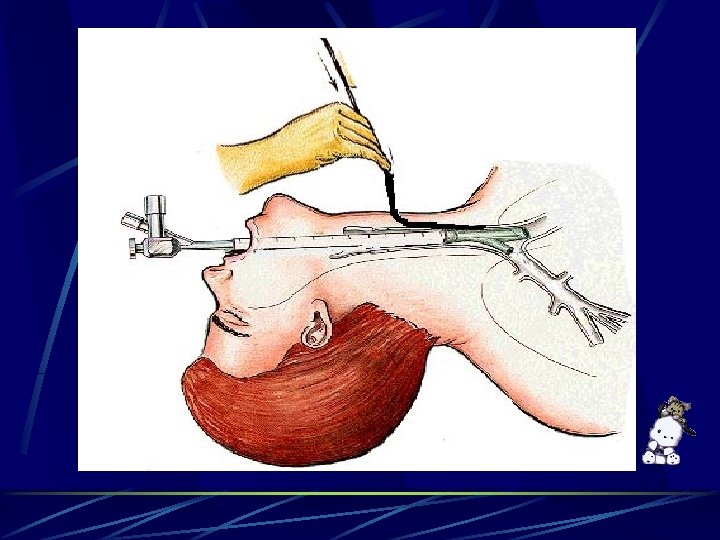
procedure Remove the granulation tissue and blood clot 13 mm Y stent insertion by rigid bronchoscope Adjust Y stent position via tracheostomy tube under flexible scope guide
Problem Apnea: O 2 supply via side hole of rigid bronchoscope ØSa. O 2: 99% 92% in about 5 mins Irritation of airway Ølaryngospasm, bronchospasm ØHR BP : BP up to 180/110
Problem Blood clot and debris: lower airway obstruction
Major Problems T. B. Poor ventilation efficiency upper airway leakage lower airway obstruction Apnea during procedure Surgical airway manipulation is a strong stimulus resulting in bronchospasm Blood clot and debris: lower airway obstruction
Discussion Airway management ventilation l laryngospasm and bronchospasm l bleeding due to surgical manipulation l Tuberculosis
Ventilation Intermittent ventilation Closely monitor Avoid continuous positive pressure ventilation l increased intrathoracic pressure
Laryngospasm Anesthetic depth should be adjusted If laryngospasm occurs Remove the offending stimulus l Give 100% oxygen l Increase anesthetic depth l Succinylcholine l
Bronchospasm Intravenous aminophylline or salbutamol Volatile anesthetic agents and ketamine are also effective bronchodilators Epinephrine is indicated in lifethreatening situations
Bleeding during surgery Suction One lung intubation
Anesthesia in patients with TB Delay elective surgical procedures until no longer considered infectious Perform tracheal intubation in a negative pressure environment Place a high efficiency particulate air filter between the Y-connector and mask or tracheal tube
Place bacterial filters on the exhalation limb of the anesthesia delivery circuit Use a dedicated mechanical ventilator Postoperative care in an isolation room
Conclusion O 2 saturation Anesthetic depth
Thank you for your attention!