Anemia in Pregnancy Rajeev Ojha Table 1 Blood

Anemia in Pregnancy Rajeev Ojha

Table 1. Blood Sample Results Red Blood Cell Count 3. 5 million/mm 3 Hemoglobin (Hb) 7 g/dl Hematocrit (Hct) 30% Serum Iron low Mean Corpuscular Volume (MCV) low Mean Corpuscular Hb Concentration low (MCHC) Total Iron Binding Capacity in the Blood (TIBC) high

l. A diagnosis of anemia due to iron deficiency is made and oral iron supplements prescribed. Her symptoms are eliminated within a couple of weeks and the remainder of her pregnancy progresses without difficulty.
 - Hb 7. 1 gm/dl, Hct 23% -")
Labs: l Complete blood count (CBC) - Hb 7. 1 gm/dl, Hct 23% - WBC 5, 400/mm 3 (differential is normal) - Platelets 450, 000/mm 3 - Mean Corpuscular volume (MCV) is 74 fl (normal 85 -95 fl) - Red cell Distribution Width (RDW) is 17. 1% (normal 13 -15).

Defination of Anemia during Preg. l Hemoglobin below 11 gm/dl in 1 st and 3 rd trimester and below 10. 5 gm/dl in second trimester.

WHO l 11 gm/dl l By or less this standard, 50% of women not on hematinics become anemic.

Incidence l Anaemia may affect 10% of pregnancies in developed countries and is considerably commoner in developing countries, where it is a major source of maternal morbidity and a contributor to mortality. l Up to 56% of all women living in developing countries are anaemic (Hb < 11 g/dl) due to infestations.

Classification l Physiologic l Pathologic: a. Deficiency: Iron, Folic A. , Vitamin B 12 b. Hemorrhagic: APH, Hookworm c. Hereditary: Thalassemia, Sickle, H. Hemolytic Anemia d. Bone Marrow Insufficiency: Aplastic Anemia e. Infections: Malaria, TB f. Chronic Renal Diseases or Neoplasm.

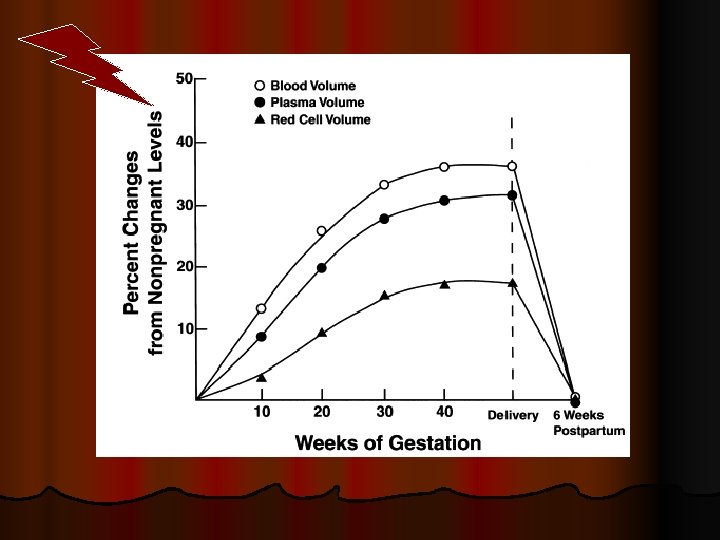
Concept of Physiologic Anemia l Disproportionate increase in plasma vol, RBC vol. and hemoglobin mass during pregnancy l Marked demand of extra iron during pregnancy especially in second trimester

Criteria for Physiologic Anemia l Hb: 10 gm% l RBC: 3. 2 million/mm 3 l PCV: 30% l Peripheral smear showing normal morphology of RBC with central pallor


Significance of Hypervolemia 1. To meet the demands of the enlarged uterus with its greatly hypertrophied vascular system. 2. To protect the mother, and in turn the fetus, against the deleterious effects of impaired venous return in the supine and erect positions. 3. To safeguard the mother against the adverse effects of blood loss associated with parturition.

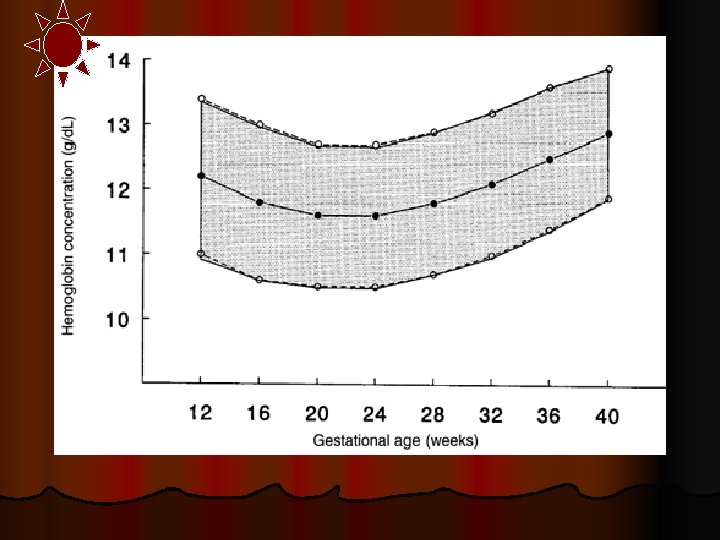
l Normal hemoglobin by gestational age in pregnant women taking iron supplement l 12 wks l 24 wks l 40 wks 12. 2 [11. 0 -13. 4] 11. 6 [10. 6 -12. 8] 12. 6 [11. 2 -13. 6]

Most common causes of Anemia l Iron loss : sweat, repeated pregnancy, hookworm infestation and malaria l Faulty absorption mechanism : due to high incidence of intestinal infestation, there is intestinal hurry l Faulty diet habit : rich carbohydrate and high phosphate reduce absorption of iron

Factors lead to develop Anemia l Increase iron demand l Diminished intake of iron l Disturbed metabolism l Pre-pregnancy health status l Excess demand

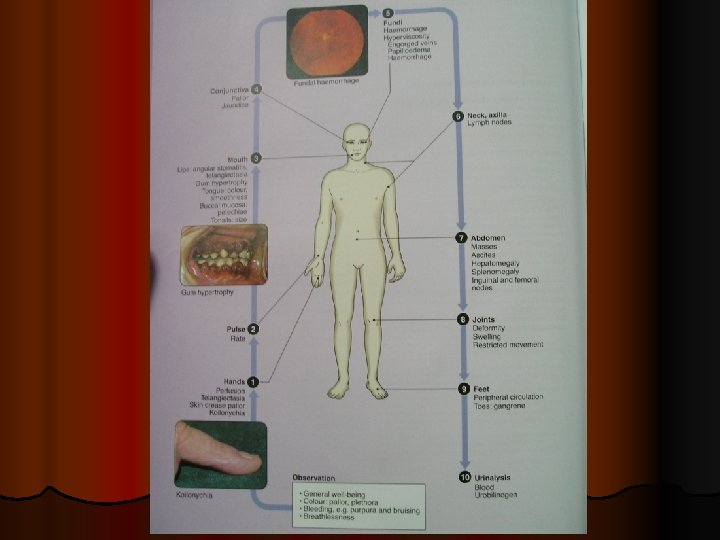
Iron Deficiency Anaemia Symptoms: lassitude, weakness, anorexia, palpitation, dyspnea l Signs: Pallor, glossitis, soft systolic murmur in mitral area due to physiologic mitral incompetence l l Degree: Mild: 8 -10 gm% Moderate: 7 -8 gm% Severe: <7 gm%

pallor

Conjunctival Pallor

Koilonychia

Smooth Tongue

Interpretation of plasma Iron deficiency anemia Anemia of chronic disease Pregnancy TIBC Ferritin Decrease Increase Decrease Increase Normal

Normal Iron Requirements l Iron requirement for normal pregnancy is 1 gm 200 mg is excreted 300 mg is transferred to fetus 500 mg is need for mother l Total volume of RBC inc is 450 ml 1 ml of RBCs contains 1. 1 mg of iron 450 ml X 1. 1 mg/ml = 500 mg l Daily average is 6 -7 mg/day

Treatment l Prophylactic: Supplement Fe – 60 mg elemental Fe with Folic Acid l Curative: 200 mg Fe. So 4 3 times daily till Hb level becomes normal, then maintenance dose of 1 tab for 100 days

Megaloblastic Anemia l l Due to impaired DNA synthesis, derangement in Red Cell maturation It may be due to Def. of Vit. B 12 or Folic Acid or both. Megaloblastic anemia in pregnancy is almost always due to Folic Acid def. Vit B 12 def is rare in Pregnancy becoz its need is less in amount and amount is met with any diet that contains animal products.

Sign and symptoms l Insidious onset, mostly in last trimester l Anorexia and occasional diarrhoea l Pallor of varying degree l Ulceration in mouth and tongue l Hemorrhagic patches under the skin and conjunctiva l Enlarged liver and spleen

Angular Cheilosis

Blood values l Hb<10 gm% l Hypersegmentation of neutrophils l Megaloblast l MCV>100 micrometer 3 l MCH>33 pg, but MCHC is Normal l Serum Fe is Normal or high TIBC is low

Treatment l Prophylactic - all woman of reproductive age should be given 400 mcg of folic acid daily l Curative -daily administration of Folic acid 4 mg orally for at least 4 wks following delivery

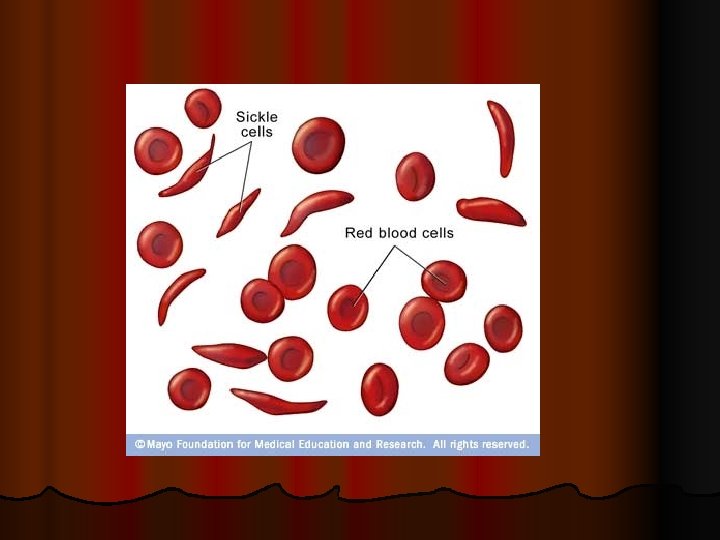
Sickle cell Hemoglobinopathy l l Hbs comprises 30 -40% total Hb There is substitution of Lysine for glutamic acid at the sixth position of B chain of Hb Red cells in oxygenated state behave normally, but in deoxygenated state it aggregates, polymerises and distort red cells to sickle. These cells are more fragile and increased destruction leads to hemolysis, anemia and jaundice.

Effects on pregnancy l Increase incidence of abortion, prematurity, IUGR and Fetal loss. l Perinatal mortality is high. l Incidence of pre-eclampsia, postpartum hemorrhage and infection is increased.

Management l Careful antinatal supervision l Air travelling in unpressurised aircraft to be avoided. l Prophylatically Folic A. 1 gm daily. l Regular blood transfusion at approx. in 6 weeks interval

My References


Thank You
- Slides: 41