ANATOMY OF PLACENTAL BARRIER INTRODUCTION Placenta is a

ANATOMY OF PLACENTAL BARRIER

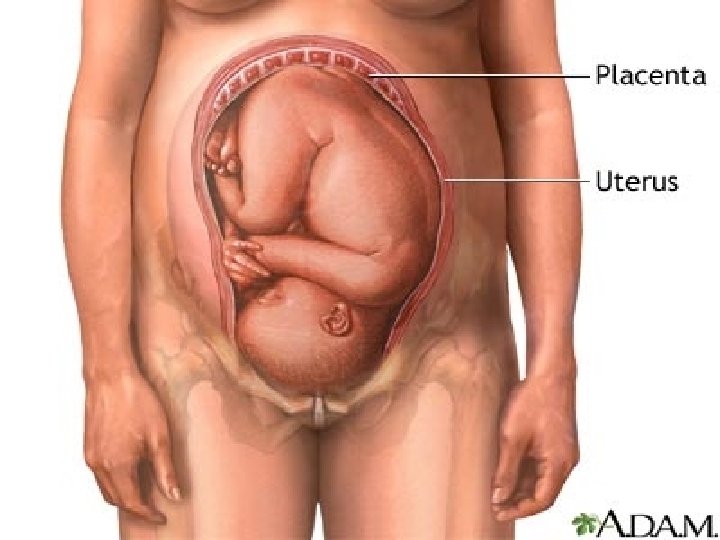
INTRODUCTION ● ● ● Placenta is a remarkable organ Has a relative short life span, it undergoes rapid growth , differentiation and maturation. A unique fetal –maternal communication system which creates a hormonal environment that helps initially to maintain pregnancy and eventually initiates the events leading to parturition

The human placenta is: Discoid Hemochorial Deciduate Larynthine

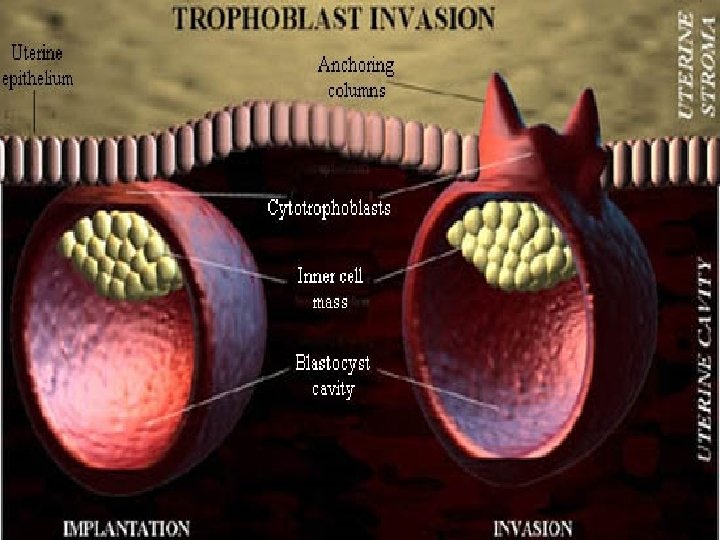
● ● Implantation is complete on 10 or 11 th postovulatory day On the 7 th day ovum Cytotrphoblast Syncytiotrophoblast

Development of Placenta ● ● ● Ovum Morula Blastocyst
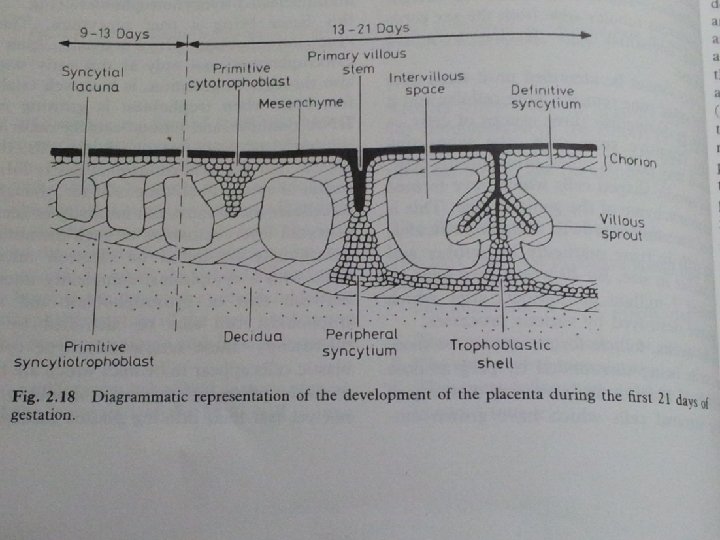

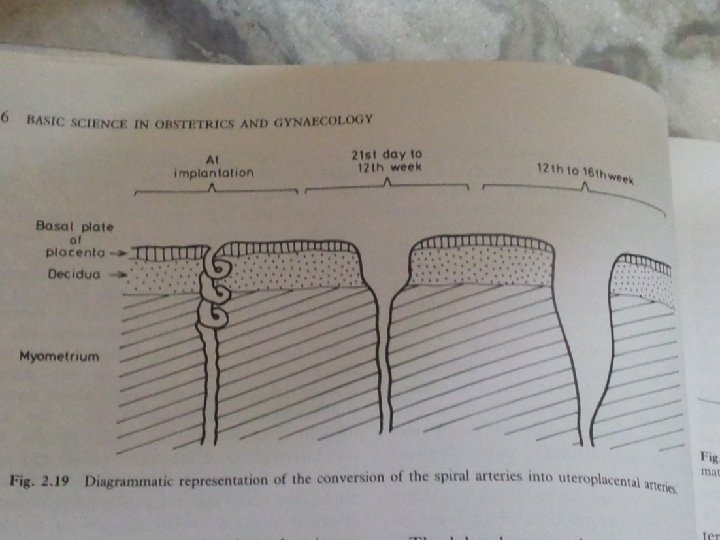
● ● Nitabuch’s layer Placenta on 21 day of gestation – vascularised villous organ The region of fibrinoid degeneration where the trophoblasts meet the decidua is calld nitabuchs layer. This layer is absent in placenta accreta

Primary villi Secondary villi Tertiary villi

● During this period there is some regression of the cytotrophoblastic elements in the chorionic plate and in the trophoblastic shell where cytotrophoblastic columns degenerate and largely replaced by fibrinoid material –Rohr’s layer

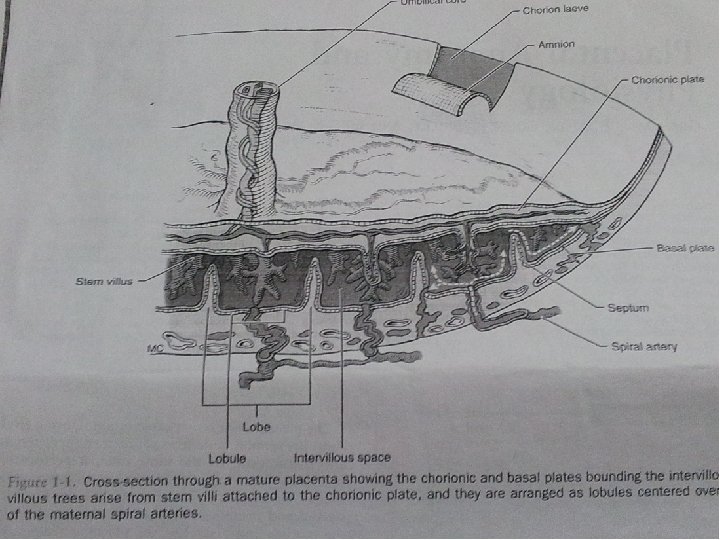
● PLACENTA AT TERM: Placenta is a discoid organ 15 – 20 cm in diameter 3 cm Thick at center Weighs about 500 gms

AT TERM MATERNAL SURFACE

FETAL SURFACE

Aging of placenta

Placental membrane ● ● Total area-4 to 14 sq m Similar to absorbtive area in adult git In later part of pregnancy the membrane thickness reduces from 0. 025 mm to 0. 002 mm Is classified as haemochorial

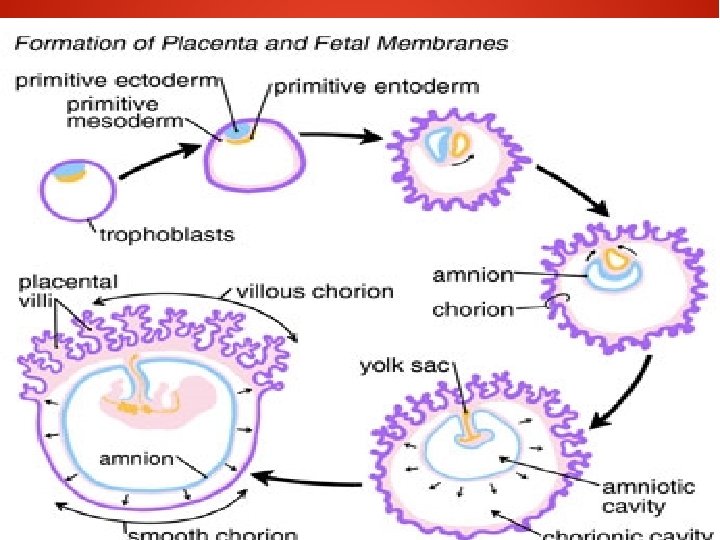
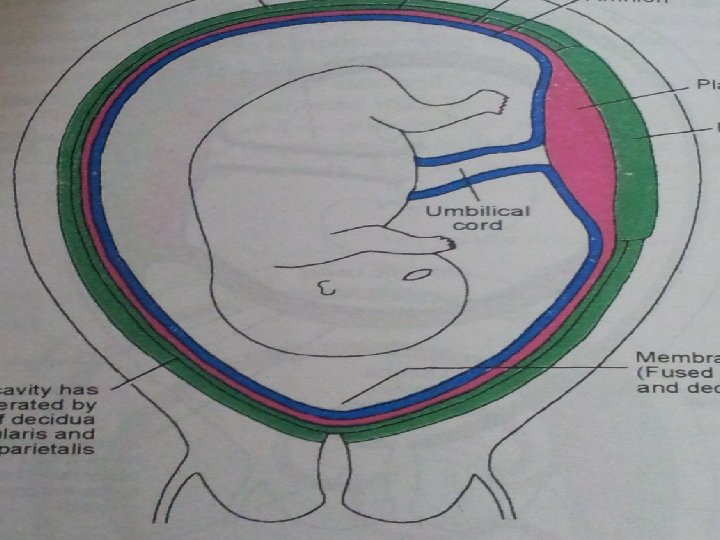
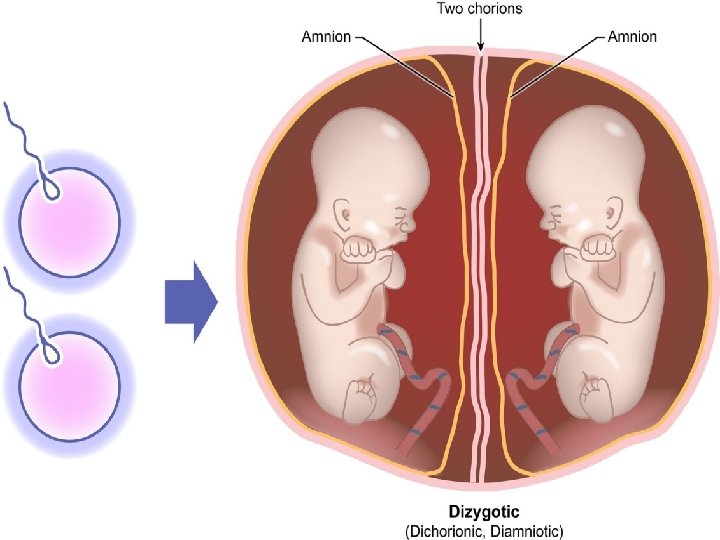
FETAL MEMBRANES 2 LAYERS: Outer chorion Inner amnion

Chorion Internally attached to amnion by loose areolar tissue Externally covered by trophoblastic layer and decidual cells of fused decidua capsularis and parietalis

Amnion Internal surface is smooth and shiny and in contact with liquor amnii Outer surface consists of a layer of connective tissue Amnion can be peeled off from the fetal surface of the placenta except at the insertion of the umbilical cord.

Hypertension

Development of membranes and formation of amniotic fluid ● ● ● ● On the 8 th and 9 th postovulatory day Endoderm Ectoderm Amniotic cavity Primary yolk sac Parietal extra embryonic mesenchyme Visceral extra embryonic mesenchyme

Amniotic fluid ● ● ● ● 12 weeks: 50 ml 16 weeks: 150 ml 38 weeks : 900 -1000 ml At term : 1000 -900 ml Clinical applications Composition of amniotic fluid functions


Placental circulation ● ● ● Uteroplacental circulation Circulation in the intervillous space Feto-placental circulation
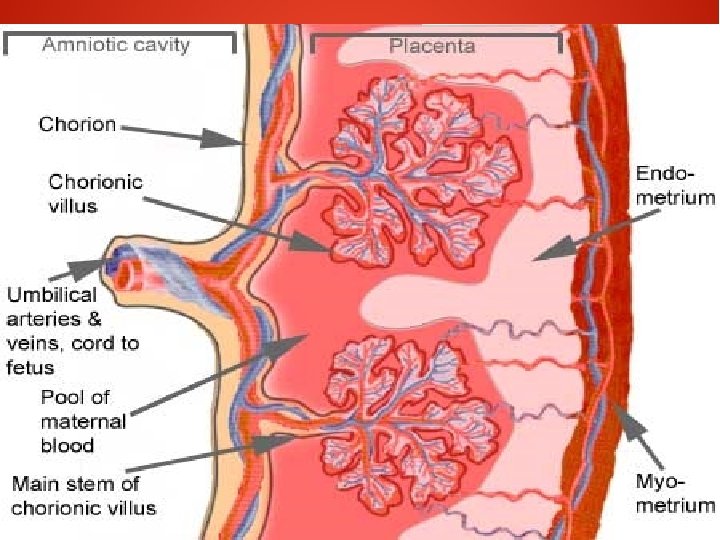
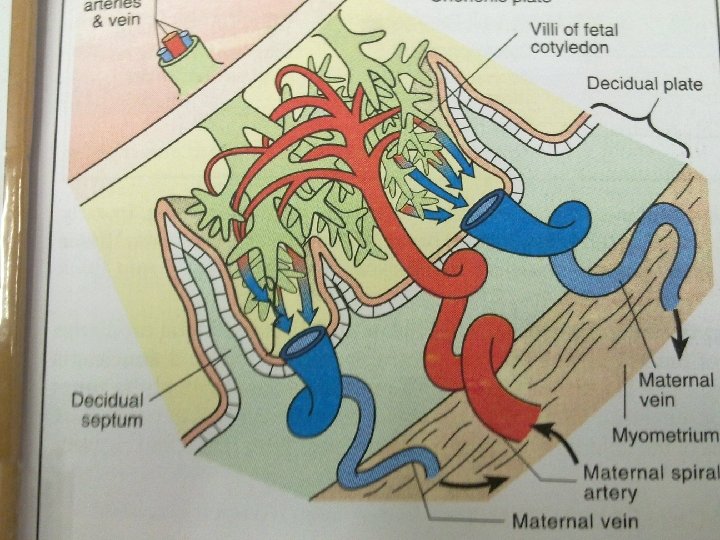

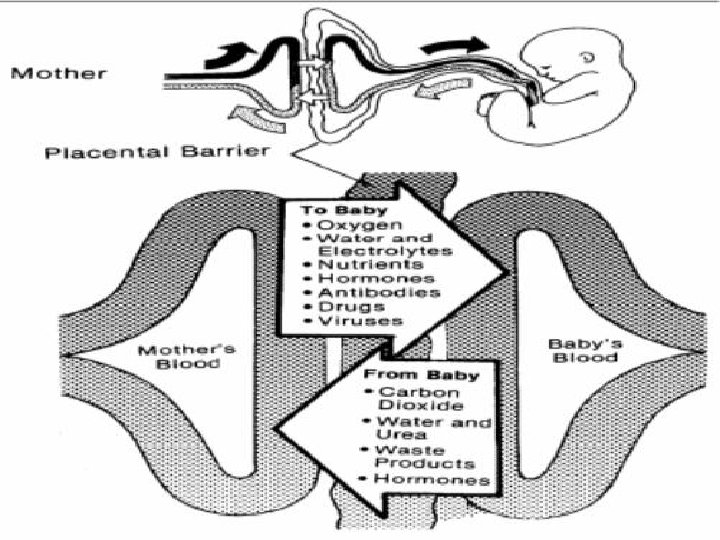

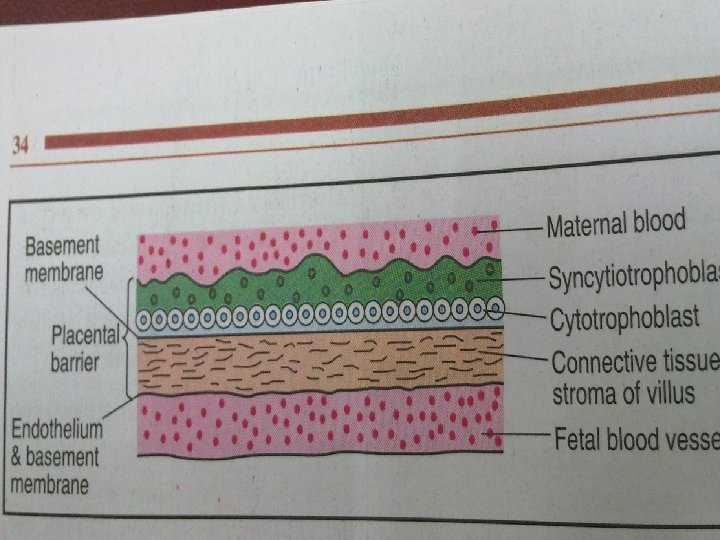
PLACENTAL BARRIER ● ● Inspite of close proximity , there is no mixing of the maternal and fetal blood. They are separated by placental membranes or barrier.

In early pregnancy it consists of: ● Syncytiotrophoblast ● cytotrophoblast ● Basement membrane ● Stromal tissue ● Endothelium with fetal capillary wall ● Its about 0. 025 mm thick

Near term. . ● ● ● Attenuation of syncytial layer Sparse cytotrophoblast and distended capillaries fill the villus. Vasculo- syncytial membrane: is the specialised zone of villi where the suncytiotrophoblast is thin and anuclear These alphazones are for gas exchange. Betazones of terminal villi are for hormone synthesis

BARRIER FUNCTION Fetal membrane is a protective barrier to the fetus against noxious agents circulating in the maternal blood. Antigen and antibody can traverse through the placental barrier The race of drug transfer is increased in late pregnancy

Maternal infections caused by : Virus Bacteria Protozoa , is transmitted to the fetus by crossing the placental barrier.

Placental functions ● ● ● ● Simple diffusion Facilitated diffusion Active transfer Endocytosis Exocytosis Respiratory functions Excretory functions

● ● ● Nutritive function Enzymatic function Barrier function Immunological function Hormones

● ● ● ● ● Hormones produced by placenta HCG HUMAN PLACENTAL LACTOGEN CHORIONIC ADRENOCORTICOTROPIN RELAXIN PARATHYROID HORMONE RELATED PROTEIN GROWTH HORMONE RELATED VARIENT HYPOTHALAMIC LIKE RELEASING HORMONE GONADOTROPIN RELEASING HORMONE CORTICOTROPIN RELEASING HORMONE

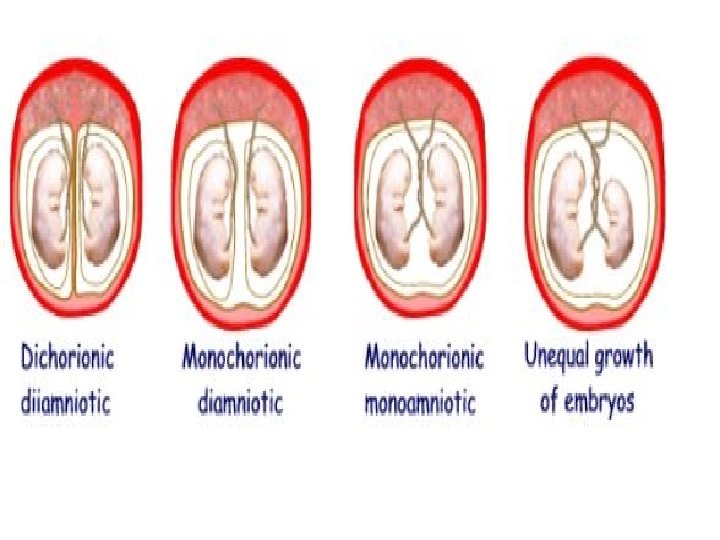
Clinical aspects of placenta ● Multiple pregnancy

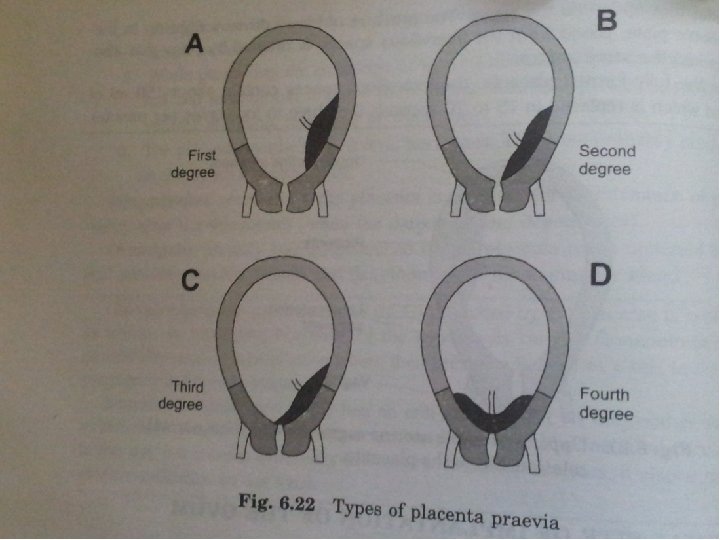
Placenta praevia ● ● ● ● Normal sites of implantation of ovum Upper uterine segment Abnormal sites of implantation of ovum Types of placenta praevia First degree Second degree Third degree Fourth degree

Placental abruption

● ● ● Bleeding following premature separation of normally situated placenta Incidence: 0. 49 to 1. 8% Types : concealed : 20 to 35% revealed : 65 to 85%

Gestational trophoblastic disease ● ● Proliferative abnormality of trophoblast associated with pregancy Persistance GTD = GESTATIONAL TROPHOBLASTIC NEOPLASIA

Classification ● ● ● Hyaditiform mole complete partial Invasive moles Placental site trophoblastic tumors Choriocarcinoma Non metastatic disease confirmed to uterus
 &placental biopsy Indications : Prenatal diagnosis of genetic disorder throughout")
Chorionic villi sampling (CVS) &placental biopsy Indications : Prenatal diagnosis of genetic disorder throughout gestation ●

Procedure

PLACENTAL TRANSFER Drugs that doesn’t cross placenta: Heparin large molecule highly polar Curare ●

Teratogenic drugs Anticonvulsants Phenytoin: cleft lip /palate Microcephaly Hypertelorisum Fingernail hyperplasia Sodium valproate: Neural tube defects ●

Lithium Ebstein’s anomaly Warfarin Chondrodysplasia punctate Microcephaly Aspleenaia Diaphragmatic hernia

Diethyl stil bestrol Adenocarcinoma of vagina Danazol Virulization of female

Retinoids Crainofacial Cardiac Thymic Cns ●

Thank you
- Slides: 58