ANATOMY AND PHYSIOLOGY OF NORMAL DEGLUTITION Anatomic Structures

 • Hard Palate •")












































- Slides: 48
ANATOMY AND PHYSIOLOGY OF NORMAL DEGLUTITION Anatomic Structures • Oral • Pharynx • Larynx • Esophagus
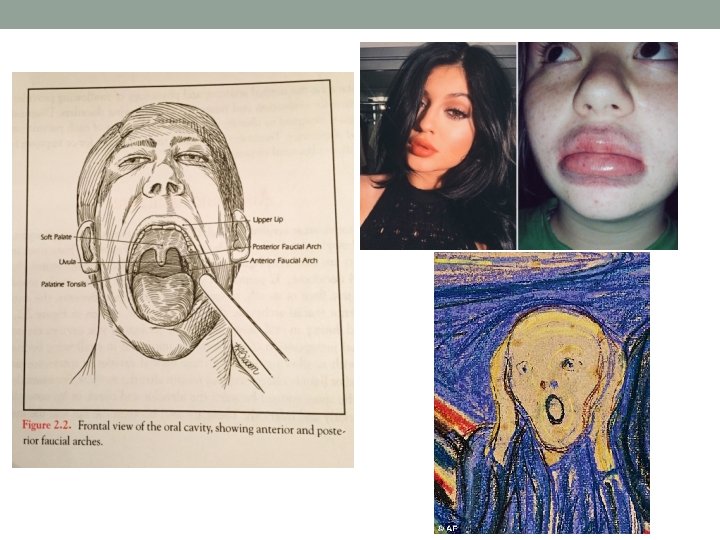
ORAL • Lips anteriorly • Teeth (24 Decidous, 32 Permenant) • Hard Palate • Soft Palate • Uvula • Mandible • Floor of Mouth • Tongue • Facial Arches
Sulci Natural Cavities/Spaces • Anterior Sulcus • Lateral Sulcus • Worried about this due to residue and the client pocketing food
Musculature of the Floor of Mouth • Mylohyoid • Geniohyoid • Anterior Belly of Digastric All of which attach to the body of the mandible anteriorly and the body of the hyoid bone posteriorly
Hyoid Forms foundation of the tongue Larynx is supended from the Hyoid Bone by the Thyrohyoid Ligament and Thyrohyoid muscle If the Hyoid elevates and moves forward, the larynx will move upward and forward unless it is stabilized by other muscles Crucial info for swallow
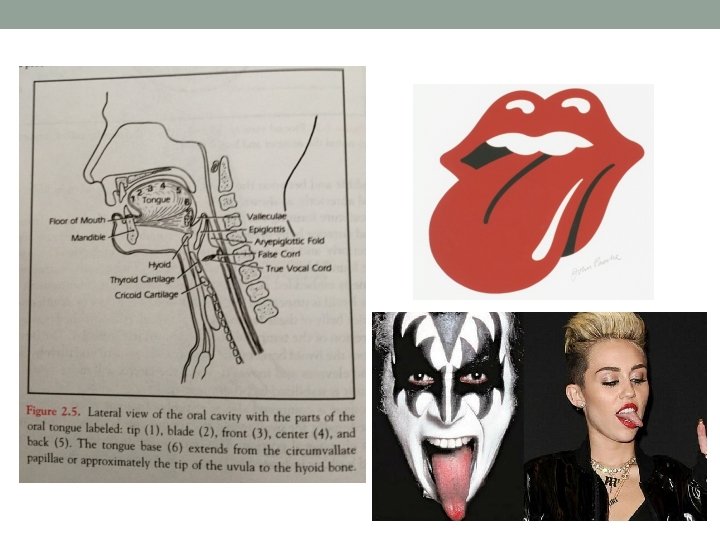
Tongue Oral • • • Tip Blade Front Center Back Ends at Circumvallate Papillae Active Under Cortical/Voluntary Neural control Left hemispehere stroke problem Pharyngeal tongue (Tongue base) Begins at the Circumvallate Papillae, ends at the Hyoid bone Active during pharyngeal swallow Involuntary neural control – brainstem function • We cannot manipulate or control this because it is an involuntary function Can be placed under some degree of voluntary control Brainstem problems= no swallow Swallow while you are sleeping
Oral Cavity • Hard palate/Maxilla • Velum/soft palate • Uvula Velopharyngeal closure muscle pulls • Palatopharyngeus • Levator palatal muscle • Superior Pharyngeal constrictor
Salivary Glands Viscid – mucus like 2. Serous – watery 1. Maintain oral moisture Reduce tooth decay Assist in digestion Neutralize stomach acid • Going down a water slide with no water • With no saliva things will get stuck • Diabetes- dry mouth
Pharyngeal Cavity 3 Pharyngeal constrictors • Superior • Middle • Inferior Forms the posterior and lateral pharyngeal walls They squeeze the food down
Pharyngeal cavity • Run laterally to attach to bony and soft tissue structures located • • anteriorly: pterygoid plates, soft palate, BOT (base of tongue), mandible, hyoid bone, thyroid and cricoid cartilages Form the anterior wall of the pharynx Inferior fibers of the superior constrictor attach to tongue base/glossopharyngeus muscle. TBR (tongue base retraction) and Anterior bulging of the post pharyngeal wall at tongue base. The TB has to make contact with the wall and it’s the contact that literally pushes the food down and opens the cricoid muscle Tongue is like drew brees, if his throw is weak, it wont make it to his person
Cricopharyngeal muscle • Attach to cricoid lamina • Cricoid lamina/cricopharyngeus forms valve into esophagus called the cricopharyngeal region • This is just an area • CP • UES • Upper esophageal sphincter • PE segment • Pharyngeal esophageal • Tonic (tone) when awake, loses tonic with sleep • Prevents air into esophagus with respiration • Reduce material backflow into pharynx • Sphincter 2 -4 cm zone of elevated pressure – greatest pressure immediately prior to swallow and during inspiration
Esophagus Collapsed muscular tube 23 -25 cm long with sphincter at each end UES/LES (lower esophageal sphincter) Pharynx open vs. esophagus closed Sits behind trachea – TE wall (party wall) LES (esophagus and stomach) keep food and secretions in 2 layers of muscle: inner circular and outer longitudinal Job is to pull food down
Peristalsis • Peristalsis is only in a collapsed tube system • It is the actual pulling system • It is an involuntary movement- constriction
Larynx Base of tongue, pharynx opens into larynx Topmost epiglottis Attached into hyoid bone by a ligament Base attached to thyroid notch
Larynx Wedge-shaped space is the Valleculae Open into larynx is Laryngeal Vestibule, which ends at superior surface of false folds • If it goes into the laryngeal vestibule then it is penetration, then when it goes past the true vocal folds then it is aspiration • Penetration can only happen in the anterior part. • Aryepiglottic folds form lateral walls • Rocks up and forward to get it up and it out of the way • Arytenoids tilt anteriorly during swallowing, thought to be form pull of the thyroarytenoid muscle fibers. • Tilt contributes to closure of airway • It brings the cord together to keep things from entering the larynx • True cords form last level of airway protection
Larynx 3 levels of sphincter in the larynx 1. Epiglottis and aryepiglottic folds 2. Arytenoids 3. False Cords If one is compromised others might be compromised
Larynx • Larynx elevates • Pull anteriorly and lowers for various activities • Hyoid bone serves as foundation for the tongue • When one structure moves, it often pulls on and moves attached structures
• https: //www. youtube. com/watch? v=Yo. Dh_g. HDvkk • https: //www. youtube. com/watch? v=hdc. Tmpv. DO 0 I
Physiology 1. Oral prep: food manipulated/masticated 2. Oral phase of swallow: tongue propels food post till pharyngeal swallow triggered 3. Pharyngeal Phase: bolus moved through pharynx 4. Esophageal phase: cervical – thoracic to stomach *duration and characteristics depend on volume and type *580 swallows per day *respiration and swallow are reciprocal – halts w/ pharyngeal phase in all ages. Cant swallow and breath at the same time
1. Oral Prep • Needs sensory recognition • Movement varies w/ viscosity • Requires open nasal airway and nasal breathing Tippers and Dippers • Tippers – food held midline w/ tip elevated and contact w/ alveolar ridge • Dippers – 20%, food held floor of mouth in front of the tongue Tongue thrust – tongue moves anteriorly w/ the bolus pushing food from the mouth. Seen w/ adults with frontal lobe damage and children w/ CP.
Oral Prep • Soft palate is pulled down and forward, sealing off the oral cavity from pharynx • Mastication involves a rotary lateral movement of mandible and tongue. Tongue mixes food w/ saliva w/ peripheral feedback to position bolus on teeth and prevent injury to tongue • Tension in buccal musculature closes the lateral sulcus • After chewing, tongue pulls food into semi-cohesive bolus before oral stage of swallow initiated
Oral Prep • Active chewing, soft palate not pulled down, thus premature spillage common, not normal during hold phase of liquid/pudding • Volume of bolus swallowed varies w/ viscosity; this downsizing w/ viscosity allows easier passage through pharynx and UES. Larger volumes, the tongue will subdivide • Larynx and pharynx are at rest during oral prep phase • Great deal of sensory info is processed from sensory receptors throughout the oral cavity
2. Oral Phase • Initiated when tongue begins post movement of bolus • Sides and tip of tongue anchor against the alvelor ridge. Central groove is formed and acts as a chute • Viscosity thickens, pressure of the oral tongue against palate increases – negative pressure of tension of buccal musculature • 1 -1. 5 seconds • Needs labial seal, intact lingual movement, intact buccal musculature, normal palatal muscle, and ability to breath through nose
Bolus propulsion
3. Triggering of Pharyngeal Swallow • As the tongue movement propels the bolus post, sensory receptors in the oropharynx and tongue are stimulated, sending sensory info to cortex and brainstem • Bolus head passes faucial arches and tongue base crosses the lower rim of the mandible, oral stage is terminated and pharyngeal swallow is triggered • If pharyngeal stage is not triggered by that time, delayed • Humans cannot swallow unless there is something in their mouth
Triggering Pharyngeal Swallow • Sensory portion of pharyngeal swallow cranial IX, X, XI. Impulses travel to the swallow center in brainstem. Motor IX and X • Cortical recognition of bolus critical to initiation of oral phase
4. Pharyngeal Swallow 1. Velopharyngeal closure: elevation and retraction of the velum and complete closure of the velopharyngeal portion to prevent material from entering nasal cavity. Enables build up of pressure in the pharynx. 2. Elevation and anterior movement of the hyoid and larynx: Elevate and move anteriorly by the pull of the floor of mouth muscles (anterior belly of digastric, myolohyoid, geniohyoid, laryngeal elevator-thyrohyoid). Average elevation 2 cm. Elevation contributes to closure of the airway, forward movement contributes to opening of the UES. ****** know this
Pharyngeal Swallow 3. Closure of the Larynx: all 3 sphincters – true folds, laryngeal entrance (false folds, anterior tilt arytenoids, thickening of epiglottic base) and epiglottis. Airway closed 1/3 -2/3 second and 5 seconds w/ sequential cup drinking. TVC-true vocal cordsclose when larynx has elevated approx 50% of max elevation. 4. Cricopharyngeal opening: tension in the cricopharyngeal muscle portion of the sphincter is released. Laryngeal anteriorsuperior motion opens the sphincter, sphincter is yanked open by the motion of the larynx resulting from the upward and forward pull of the floor of mouth muscles. Pressure w/in bolus widens the opening. Once passed, larynx lowers and cricopharyngeal muscle returns to level of contraction. The pull from the elevation of the hyoid and lrynx opens up the cricopharyngeal muscle
Pharyngeal Swallow 5. Tongue base and pharyngeal wall action: when bolus reaches tongue base level, tongue base and pharyngeal walls should make complete contact during the swallow. Move towards each other, pressure builds. Pharyngeal wall contracts and continues down pharynx to UES. You need the contraction for to move it down
Peristalsis Progressive contraction down a muscular tube Pressure generated by TBR and pharyngeal wall constriction increases w/ bolus viscosity. Pressure applied to the tail of the bolus.
Movement • Velopharyngeal closure and hyolaryngeal excursion occurs simultaneously • Open UES and airway closure • Pressure on bolus 1. oral tongue pushes tail 2. tongue base reaches pharyngeal wall and apply pressure to bolus.
Always Remember This • Pharyngeal swallow must trigger for physiological activities (Velar, pharyngeal, tongue base, laryngeal) to occur. These activities occur ONLY as a result of triggering pharyngeal swallow! There is no way to voluntary initiate or modify pharyngeal contraction!
Movement • Pharyngeal transit time – time bolus to move from point pharyngeal swallow is triggered through the cricopharyngeal juncture into esophagus. 1 second or less. • Divides at the valleculae w/ ½ flowing down each side of pharynx through pyriform sinuses • Epiglottis directs food around the airway • Joins again at UES
Esophageal Phase • Time from UES to LES/stomach varies 8 -20 seconds. Bolus pulled through w/ peristaltic wave • UES and the LES relax at the same time. • Globus sensation: pressure again the posterior side of the cricopharyngeal structure. Feeling like you have something stuck in your throat
Mechanism as a Set of Tubes & Valves • Oral cavity – horizontal • Pharynx – verticle UES – musculoskeletal valve (cricopharyngeal muscle & cricoid cartilage) LES – muscular sphincter. Keep food/stomach acid in stomach
Changes with Age Infant: tongue fills the oral cavity. Hyoid bone and larynx are up, velum hangs lower, uvula rests inside epiglottis and forms pocket in valleculae. Greatest elongation of the pharynx and downward displacement of larynx occurs during puberty
Infant • Swallow begins in the fetus. Sucking nipple, infant repeatedly pumps the tongue expressing milk. Normal infants 2 -7 pumps. Bolus of adequate size has been formed, triggers pharyngeal swallow. 1 ml liquid produces oral then pharyngeal swallow (similar to adult). • An infant does not have an oral swallow, just pharyngeal • Bite achieved approx 7 months • Chewing 10 -12 months • Normal adult pattern 3 -4 years • This is when the oral phase starts
Older Adult • Number of chewing strokes related to age and dental status. Increased strokes w/ poor dentition or dentures. • Loss of sensation • Physiological changes occur 70+. Ossification of thyroid and cricoid cartilages and hyoid bone, appear more prominent. • They start to get larger • Larynx may begin to lower. (when it starts to lower it is harder for it to get pulled up and forward) Cervical arthritis, impinge on pharyngeal wall decreases flexibility, decrease strength of pharyngeal contraction. • Cervical osteophites: pieces of bone that have started to form • They also have posture problems
Age and Swallowing • People may become Dippers • longer oral stage • Pharyngeal residue • Everything is becoming weak and flaccid • Increased penetration w/out aspiration • Longer esophageal transit • The striated and smooth muscle in the esophagus get weaker
Age and Swallowing • Decreased max laryngeal and hyoid anterior and vertical movement indicating reduced neuromuscular reserve (difference between necessary movement and actual motion)
Age and Swallowing • Decreased flexibility cricopharyngeal opening – less change as volume increased, exacerbates w/ weakness • Taste – intensity of taste & smell are reduced • Taste buds die when you have dementia
Coordination of respiration & swallowing • Apneic period – fraction of second. Corresponds w/ closure of airway during pharyngeal stage. Duration increases bolus volumes • Airway opens w/ oral prep, oral, and esophageal stages • Interrupting exhalation and returning to exhalation after the swallow • Slight airflow through the larynx and pharynx after the swallow • May clear any residue from around the airway entrance • Dysphagia patients may more often interrupt inhalation to swallow • More subglottal pressure on the exhilation
Variations in normal swallowing 1. 2. 3. 4. 5. 6. Volume effects – bolus volume creates greatest systematic changes in oropharyngeal swallow. Small volume – each phase, whereas large (10 -20 ml) simultaneous oral & pharyngeal activity are going to have to happen at the same time die to size. Increased viscosity increases pressure. Valve functions all increase slightly in duration. It takes more time to get peanut butter down Cup drinking – early airway closure, duration 5 -10 seconds Straw drinking – suction ‘chug-a-lug’ – pull larynx forward & hold breath Pharyngeal swallow w/ no oral swallow
• https: //www. youtube. com/watch? v=_Aw 7 Ek. Is. YK 0 • https: //www. youtube. com/watch? v=-4 y. KOC 1 QT 9 M
Components of All Swallows ***** 1. 2. 3. 4. Components that must be present Oral propulsion bolus into pharynx Airway closure UES opening Tongue base – pharyngeal wall propulsion to carry the bolus through the pharynx and into the esophagus • Variations on normal swallow generally involve changing the timing of these elements, but all must be present and normal for bolus to clear safely and efficiently!