Anatomy and Injuries to the Spine Adapted from


 1 st-atlas")






































 Don’t")




























 l ¡ If athlete")







- Slides: 89
Anatomy and Injuries to the Spine Adapted from Connie Rauser
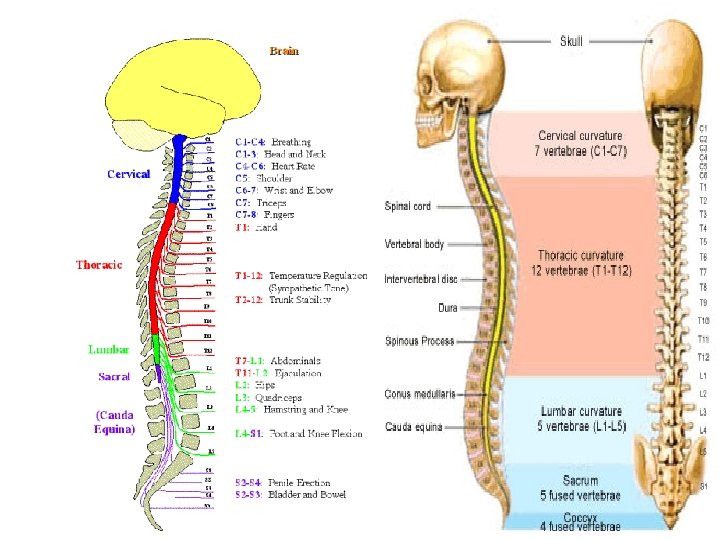
Function of anatomy Protects spinal cord ¡ Holds body upright ¡ Site for muscle & ligament attachment (support spine) ¡ Discs provide shock absorption ¡ Nerves provide sensation and motor function ¡
Bony anatomy ¡ Vertebrae l 7 cervical (flexion, extension, lateral flexion, rotation) 1 st-atlas ¡ 2 nd-axis ¡ l l 12 thoracic (little movement) 5 lumbar (less flexion than extension, some rotation 5 sacral (fused) 3 -4 coccyx (fused)
Anatomy of spine ¡ Parts of vertebrae l l l Spinous process Transverse process Body
Cervical vertebrae
Thoracic vertebra
Lumbar Vertebrae
Sacrum and coccyx
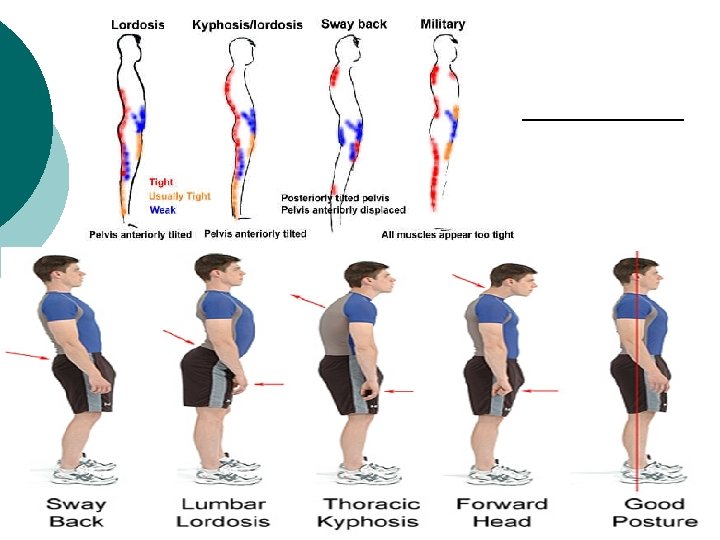
Posture ¡ Neutral spine l ¡ Thoracic curve l ¡ Normal alignment Excessive--kyphosis Lumbar curve l Excessive--lordosis
Discs Fibrocartilaginous ¡ Shock absorbers ¡ Resist compression ¡ Keep vertebrae separated ¡ Allows movement & flexibility ¡ Provides space for nerves to exit ¡ No blood supply ¡
Discs l Nucleus pulposus ¡ l Jelly-like core Annulous fibrosus ¡ Cartilaginous outer rings
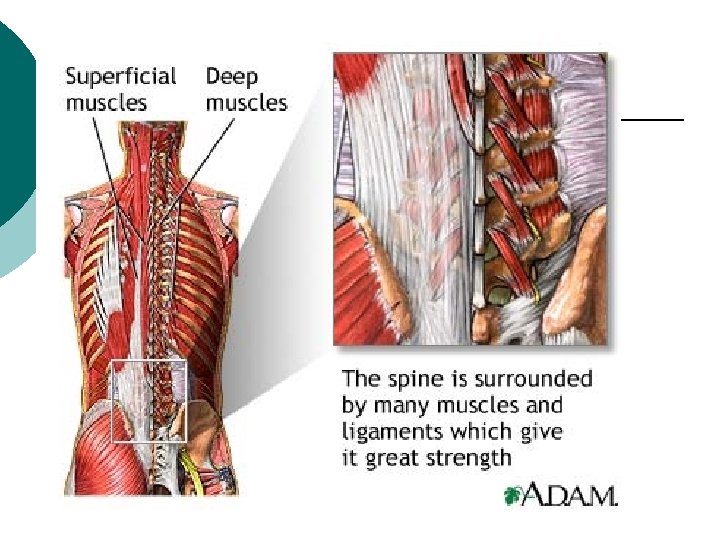
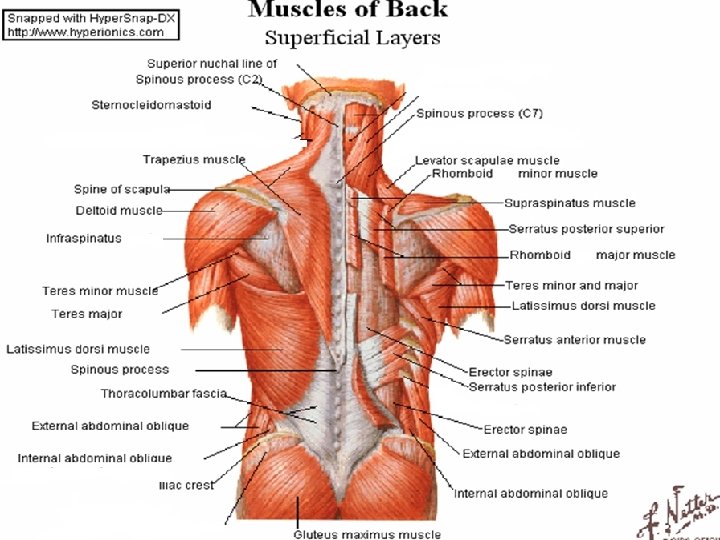
Muscles Provide movement & stability ¡ Deep—erector spinae ¡ l l Attach to vertebrae, ribs, pelvis 3 groups (ERECTOR SPINAE) ¡ Spinalis, iliocostalis, longissimus
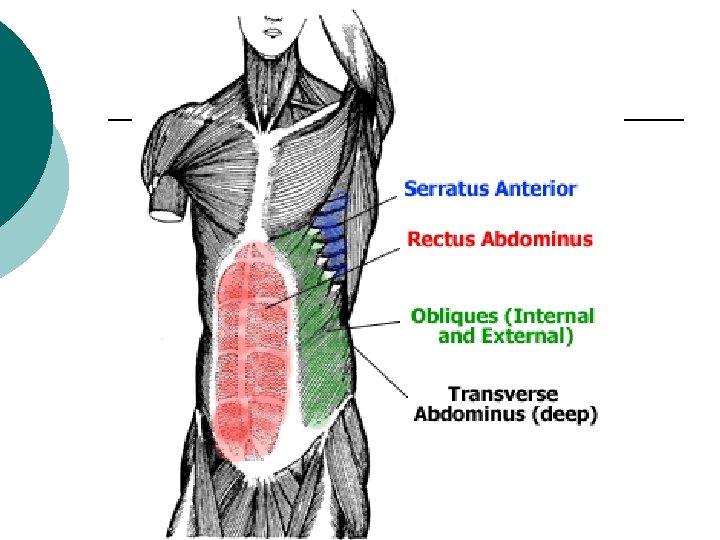
Muscles Abdominal muscles play big role in stabilizing back ¡ Trunk flexion, lateral flexion, rotation ¡ l l Rectus abdominus External oblique Internal oblique Transverse abdominus
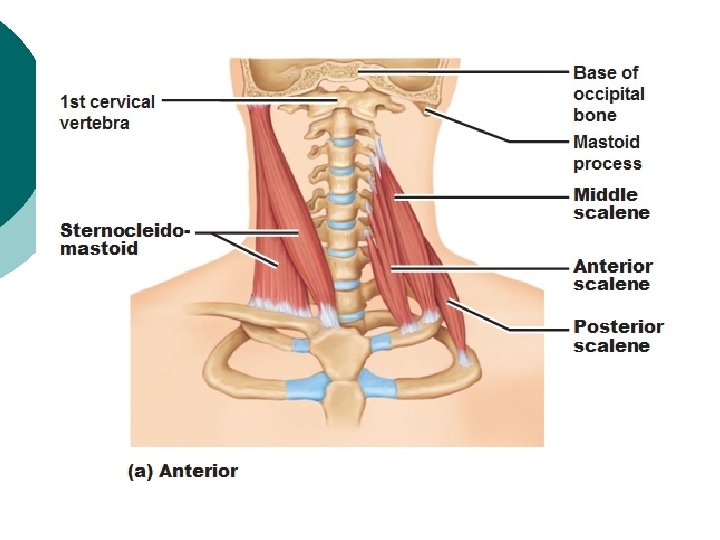
Muscles ¡ Trapezius l ¡ Sternocleidomastoid l ¡ Lateral flexion, rotation Scalenes l ¡ Upper portion aids in cervical extension Flexion of cervical area Multifidis l Rotation of spine
Muscles
Nerves Each vertebrae has a nerve that exits either below or above it ¡ 31 pairs of spinal nerves ¡ l l l 8 cervical nerves 12 thoracic nerves 5 lumbar 5 sacral 1 coccygeal
Spinal Cord Part of the CNS along with brain ¡ Contained within vertebral canal ¡ Extends from cranium to 1 st-2 nd lumbar vertebrae ¡ Lumbar roots & sacral nerves for a “horse-like tail” called cauda equina ¡ 2 plexuses ¡ l Brachial, lumbosacral
Brachial Plexus
Brachial Plexus
Lumbosacral plexus
Lumbosacral plexus
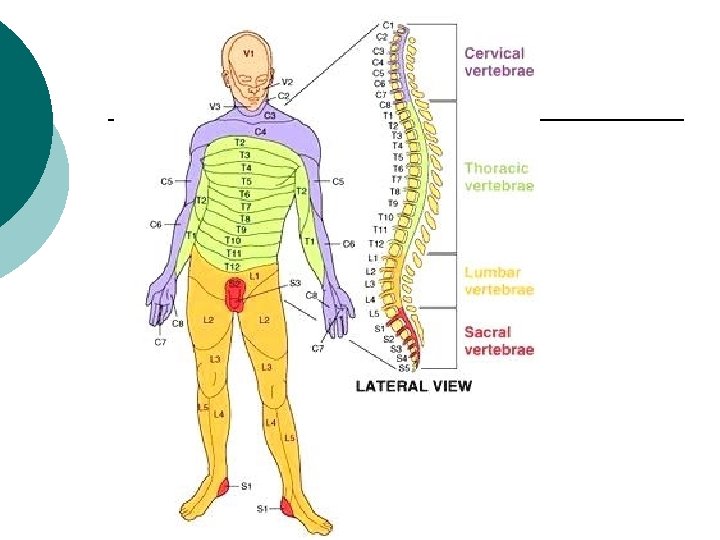
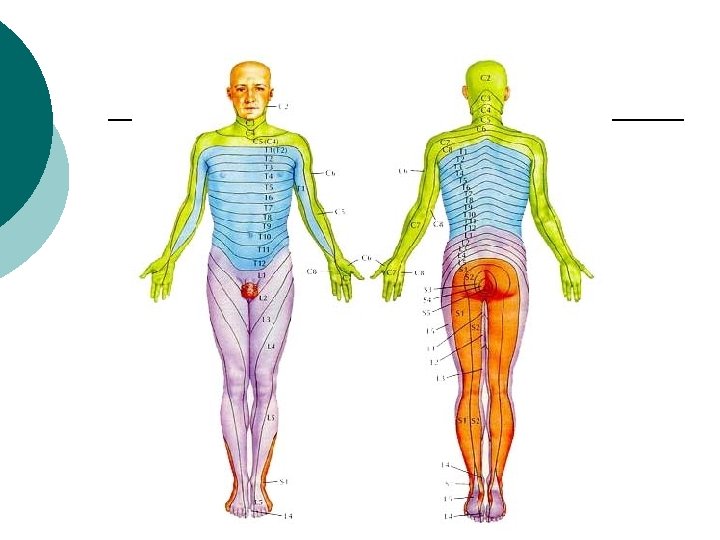
Dermatomes ¡ Area of body that has nerve sensation for each nerve root
Dermatomes ¡ Cervical l l l C 4 -shoulder C 5 -lateral arm C 6 -lateral forearm C 7 -middle finger C 8 -medial half of ring finger & forearm T 1 -medial arm
Dermatomes ¡ Thoracic l At the level of the respective thoracic vertebrae
Dermatomes ¡ Lumbar/Sacral l l l L 1 -upper anterior thigh L 2 -middle anterior thigh L 3 -lower anterior thigh L 4 -medial side of leg L 5 -lateral side of leg, dorsum of foot S 1, 2 -lateral malleolus, plantar surface of foot S 2, 3, 4 -nerve supply for bladder, intrinsic muscles of toes
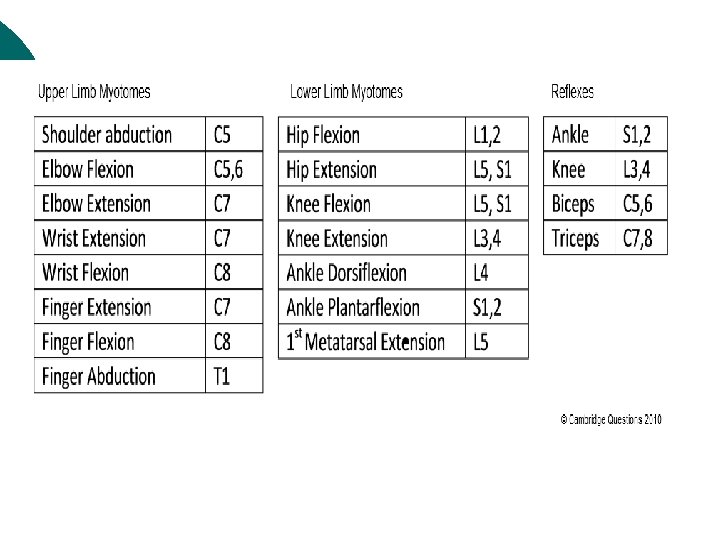
Myotomes ¡ Area of the body that has motor function
Myotomes C 5 -deltoid—shoulder abduction ¡ C 5 -6 -biceps—elbow Flexion ¡ C 6 -wrist extensors—extension ¡ C 7 -triceps & wrist/finger flexors— elbow extension, wrist/finger flexion ¡ C 8 -finger flexors—finger flexion ¡ T 1 -finger Abductors--abduction ¡
Myotomes L 1, 2, 3 -iliopsoas—hip flexion ¡ L 2, 3, 4 -Quads—knee extension ¡ L 4 -tibialis anterior— dorsiflexion/inversion at ankle ¡ L 5 -Extensor hallicus longus, extensor digitorum longus/brevis, extension/inversion at ankle ¡ S 1 -peroneus longus/brevis-eversion ¡ S 1, 2 -gastroc/soleus—plantar flexion ¡
Posture ¡ Normal l Slight curve at thoracic and lumbar areas, ears in line w/ shoulders
Posture ¡ Problems l l Forward head position-ears in front of line with shoulder Kyphosis-excessive curve of thoracic spine Lordosis-excessive curve of lumbar spine Scoliosis-lateral curve of spine
Posture ¡ Preventing poor posture l l Don’t be lazy Walk and stand as if something is pulling you up straight Carry bags/backpacks on both shoulders/alternate Carry bags at small of back (lumbar area)
Prevention of Injuries Most injuries to cervical/lumbar area ¡ Maintain adequate strength and flexibility of hip flexors and back ¡ Maintain strong abdominals/core strength ¡ Work on proper posture ¡
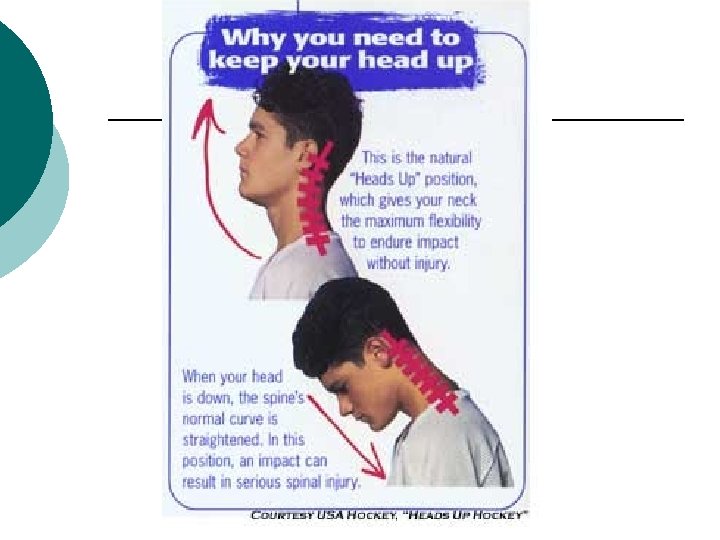
Prevention ¡ Learn to lift properly l l Maintain slight curve in lumbar spine Lift with knees and hips (legs) Keep head up ¡ Keep your butt behind you!!! ¡
Lumbar spine injuries Sprain ¡ Strains ¡ Fractures ¡ Spinal Cord Injury ¡ Dislocation ¡ Disc injury ¡
Lumbar Sprain MOI: forced into excessive trunk flexion and rotation at some time ¡ Posterior aspect of vertebral joints separate and stretch ligaments ¡
Lumbar Sprains S/S: localized pain to one side of spine ¡ Limited ROM ¡ Pain ¡ Spasms ¡ Push each vertebra anteriorly to attempt to reproduce pain ¡
Lumbar Sprains ¡ TX: l l l RICE After 48 hours—heat Active rest Maintain comfortable neutral spine Stretching Strengthening and stability exercises
Lumbar Strain Mild/moderate strains very common ¡ MOI: same as for sprains ¡ S/S: ¡ l l pain on one side spasms decreased ROM pain moves up and down length of muscles
Lumbar Strains ¡ TX: l l l RICE Gentle stretch Heat Strengthening Flexibility
Fractures ¡ MOI: l l l Severe compression type force Direct blow Extreme flexion
Fractures ¡ S/S: l l l ¡ Severe pain Pt. Tender over vertebra, especially spinous process Muscle spasm LOM Possible tingling, numbness, etc. Secondary Complication: l Spinal Cord Involvement
Fractures ¡ TX: l l l Be conservative Call 911 Neurological exam (dermatomes/myotomes) Don’t move athlete Spineboard prior to transport
Fractures
Disc Injury Common in older people but not so much in younger athletes. ¡ Referred to as “slipped” disc ¡ Nucleus pulposus pushes through rings of annulous fibrosus causing a “bulge” which can lead to herniation ¡ Most are posterior to one side ¡ Pressure exerted on nerve root ¡
Disc Injury ¡ MOI: l l Improper lifting Poor posture Poor body mechanics (excessive flexion over prolonged time frame) Trauma due to direct fall
Disc ¡ S/S: l l l Pain radiating down leg Numbness Tingling down leg Increased pain with sitting/flexion motion Decreased/absence of reflex
Disc ¡ TX: l l l l Active rest Work on posture Extension exercises Proper mechanics Core stability—especially lumbar area Traction Surgery if rehabilitation doesn’t work
Herniated disc
Disc injury
Lumbar traction
Cervical Injuries Similar to those in lumbar area ¡ May have to treat differently due to the increased mobility in that area ¡
Cervical Sprains ¡ MOI: move beyond normal ROM l l Hyperextension or hyperflexion of neck Whiplash type MOI ¡ Body forced forward by the blow while the head moves backwards, placing the cervical spine into extension stretching the ligaments & muscles at front of neck. When body stops head snaps forward stretching the posterior ligaments & muscles of neck
Cervical Sprain
Sprains ¡ S/S: l l l Neck and arm pain Pain between scapula Possible numbness or tingling Decreased ROM due to Pain Pt. Tender over the cervical area, usually localized
Cervical Sprain
Sprains ¡ TX: l l l l Check for nerve injury Ice Soft neck collar Medical referral if severe Traction Stretching strengthening
Cervical Strains ¡ MOI: l ¡ Whiplash type –same as for sprains S/S: l Muscle spasms, Decreased ROM, Muscle weakness, pain along the muscle, Pt. Tender over muscles TX: same as for sprains ¡ Return to Activity: No symptoms, full ROM & strength, Dr. release ¡
Cervical Strain
Cervical sprains/strains
Cervical Traction
Cervical Fractures/Dislocations Can result in permanent disability/death ¡ MOI: axial loading—neck flexion with force to top of head (fracture) or flexion w/ rotation (dislocation) ¡
Cervical Fx
Cervical FX/Dislocations ¡ S/S: l l l Pain & Pt. Tender over cervical spine Numbness and/or tingling down arms Muscle weakness Loss of motion Visible deformity possible (esp. w/ dislocation) but may not see it due to equipment worn
Situations in Which Cervical Spine Injury Should be Suspected Neck pain or stiffness ¡ Cervical muscle spasm ¡ Asymmetrical or Abnormal head position ¡ Respiratory difficulty (chest not moving) ¡ Unconsciousness ¡ Numbness, tingling, burning ¡ Muscle weakness or paralysis ¡ Loss of bowel or bladder control ¡
Cervical Fx/Dislocation
Cervical Fx
Cervical Fx/Dislocations ¡ TX: l l l Rule out life-threatening situations Call 911 Stabilize/immobilize head/neck If in helmet/shoulder pads, leave those in place Monitor athlete/treat for shock
Spinal Cord Injury ¡ Decerebrate vs. Decorticate Posturing
Decerebrate The worse of the two posturings ¡ Disruption of nerve pathway between brain and spinal cord ¡
Decorticate Damage to nerve pathway between brain and spinal cord ¡ May occur on one or both sides of the body ¡
Spine Boarding ¡ Observation: ( On the way to athlete) l ¡ If athlete is unconscious ALWAYS assume spinal injury. Arrival and Primary Survey l l Stabilize head and neck Check for level of consciousness If unconscious call 911 ¡ If conscious and able to communicate signs/symptoms of neck injury call 911 ¡
Spine Boarding Continued ¡ If unconscious: Look, listen and feel l l If not breathing either you (if alone) or another member of medical use pocket mask or remove face mask and begin rescue breathing/CPR If breathing continue to maintain stabilization and assess athlete
Spine boarding continued ¡ If athlete is supine with neck turned to side, maintain stabilization and rotate head in align with neck. If athlete is able to communicate, if movement increases symptoms STOP. ¡ Reasons not to move neck: l l l l Increased pain Neurological symptoms Muscle spasm Airway compromise If it is physically difficult to reposition the spine Resistance is encountered Patient expresses apprehension
Disc injury Not as common as in lumbar area ¡ MOI: overuse/previous injury ¡ S/S: pain with sitting/flexing neck down back between scapulae, weakness in arms, tingling, numbness ¡ TX: Improve neck posture, traction, strengthening, stretching, possible surgery ¡
Brachial Plexus Nerve Injury ¡ Also called l l Burner Stinger
Brachial Plexus Nerve Injury MOI: head forced to one side & shoulder depressed (they are spread apart) stretching brachial plexus ¡ S/S: tingling, burning, numbness down arm that lasts for a few seconds to minutes, muscle weakness in any/all muscles of upper extremity ¡
Brachial Plexus Nerve injury ¡ TX: l l l Ice Neck collar Physician referral if necessary Strengthening ROM exercises Return to activity when symptom free, full strength, full ROM of neck and shoulders
Brachial Plexus Nerve injury