Anal Rectal Diseases Anal Abscess Anal Cancer Anal

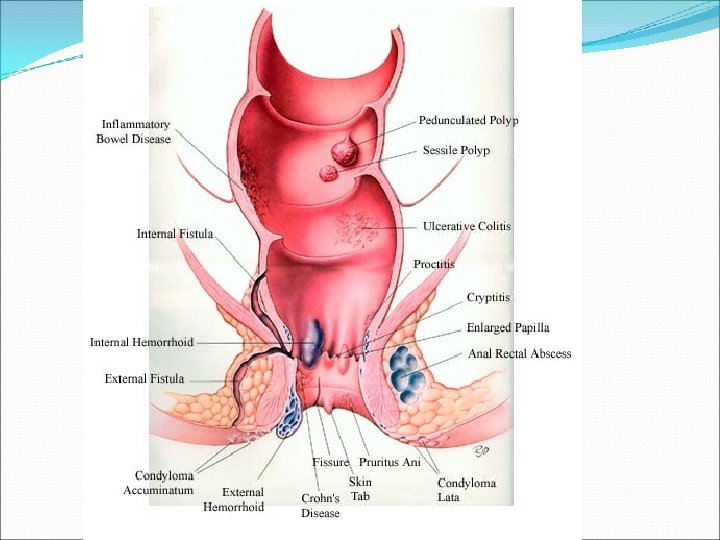
Anal Rectal Diseases Anal Abscess Anal Cancer Anal Fissure Anal Warts Cancer of the Anus Cancer of the Rectum Condyloma Cryptitis Enlarged Papillae Fecal Incontinence Fissure Fistula-in-ano Hemorrhoids Levator Syndrome Pilonidal Cyst Polyps Procidentia Proctalgia Fugax Proctitis Pruritus Ani Rectal Prolapse Rectocele Warts Venereal

Anorectal Anatomy Arterial Supply Nerve Supply Inferior rectal A middle rectal A Sympathetic: Superior hypogastric plexus Venous drainage Parasympathetic: Inferior rectal V middle rectal V S 234 (nerviergentis 3 hemorrhoidal complexes Pudendal Nerve: Motor and sensory L lateral R antero-lateral R posterolateral Anal canal Lymphatic drainage Above dentate: Inf. Mesenteric Below dentate: internal iliac Anal verge

• Pain? -> painless • Bright red bleeding • Prolapse associated with defecation Internal External • Anoderm • Swell, discomfort, difficult hygiene • Pain? -> Thrombosed

Anatomy

Haemorrhoids Back Ground • • They are part of the normal anoderm cushions They areas of vascular anastamosis in a supporting stroma of subepithelial smooth muscles. The contribute 15 -20% of the normal resting pressure and feed vital sensory information. 3 main cushions are found • • • L lateral R anterior This combination is only in 19% R posterior But can be found anywhere in anus Prevalence is 4% Miss labelling by referring physicians and patients is common

Haemorrhoids Pathogensis Abnormal haemorrhoids are dilated cushions of arteriovenous plexus with stretched suspesory fibromuscular stroma with prolapsed rectal mucosa 3 main processes: 1. Increased venous pressure 2. Weakness in supporting fibromuscular stroma 3. Increased internal sphincter tone Risk Factors Habitual 1. 2. 3. 4. 5. 6. 7. 8. Constipation and straining Low fibre high fat/spicy diet Prolonged sitting in toilet Pregnancy Aging Obesity Office work Family tendency Pathological 1. 2. 3. 4. 5. 6. 7. Chronic diarrhea (IBD) Colon malignancy Portal hypertension Spinal cord injury Rectal surgery Episiotomy Anal intercourse

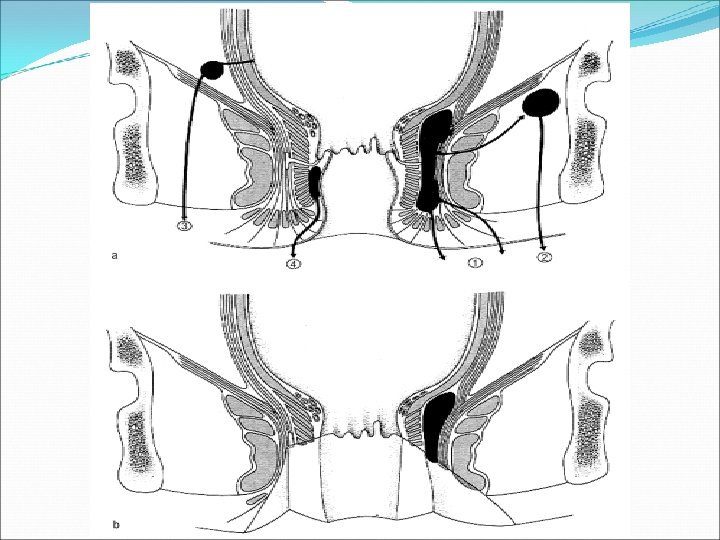
Haemorrhoids Classification: Origin in relation to Dentate line 1. 2. 3. Internal: above DL External: below DL Mixed Degree of prolapse through anus • 1 st: bleed but no prolapse • 2 nd: spontaneous reduction • 3 rd: manual reduction • 4 th: not reducable

A: Thrombosed external B: First-degree internal viewed through anoscope C: Second-degree internal prolapsed, reduced spontaneously D: Third-degree internal prolapsed, requiring manual reduction E: Fourth-degree strangulated internal and thrombosed external Reference : Sabiston Textbook of Surgery, 18 th Edition
 Examination Haemorrhoid directed: • Pain acute/chronic/")
Haemorrhoids Clinical assessment History ( Full history required) Examination Haemorrhoid directed: • Pain acute/chronic/ cutaneous • Lump acute/ sub-acute • Prolapse define grade • Bleeding fresh, post defecation • Pruritis and mucus Local General GI: • Digital: • Change in bowel habit • Mucus discharge • Tenasmus/ back pain • Weight loss • Anorexia • Other system inquiry • Inspect for: –Lumps, note colour and reducability –Fissures –Fistulae –Abscess –Masses –Character of blood and mucus • Perform proctoscopy and sigmoidoscopy General abdominal examination

Haemorrhoids Investigations: The diagnosis of haemorrhoids is based on clinical assessment and proctoscopy Further investigations should be based on a clinical index of suspicion Lab: CBC / Clotting profile/ Group and save Proctography: if rectal prolpse is suspected Colonoscopy: if higher colonic or sinister pathology is suspected

Complications 1. Ulceration 2. Thrombosis 3. Sepsis and abscess formation 4. Incontinence Thrombosed internal haemorrhoids Thrombosed external haemorrhoids



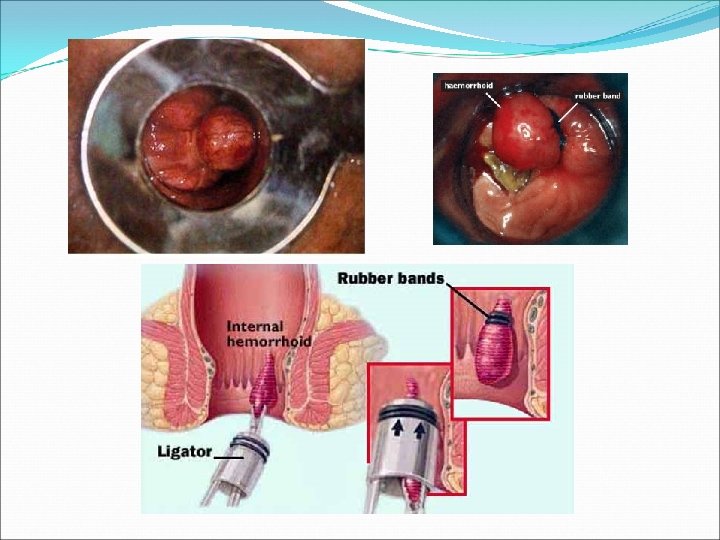
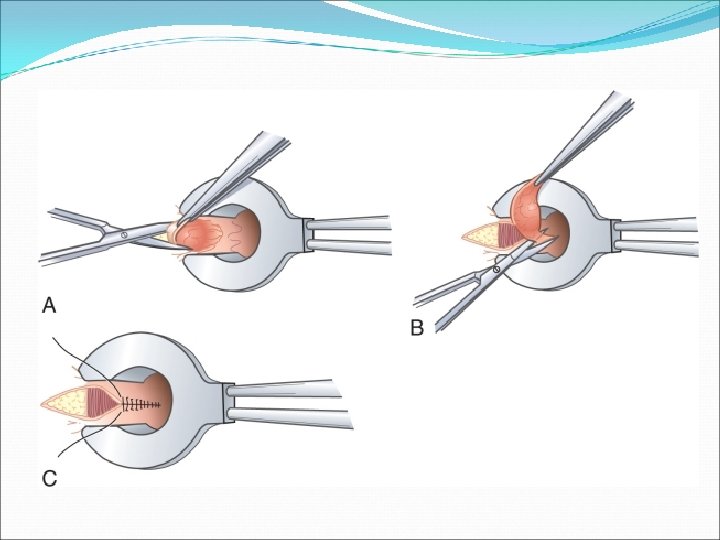
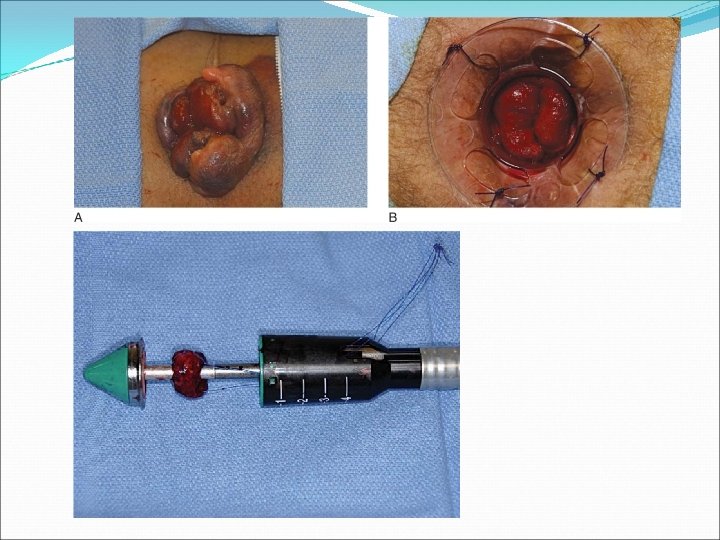
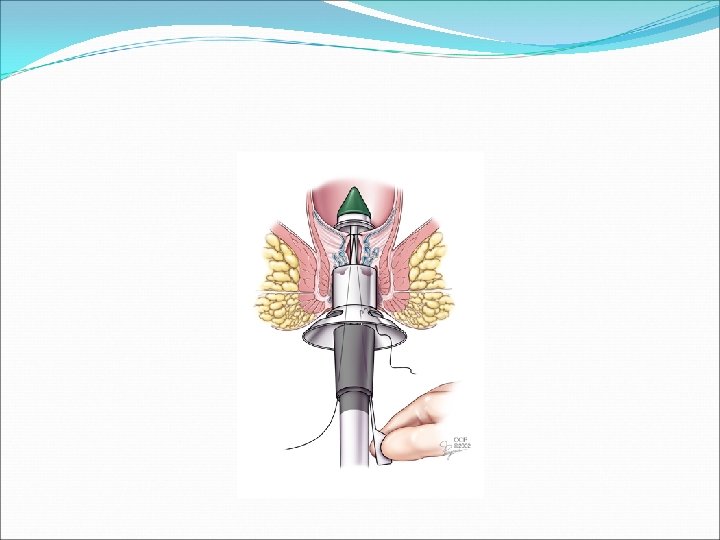
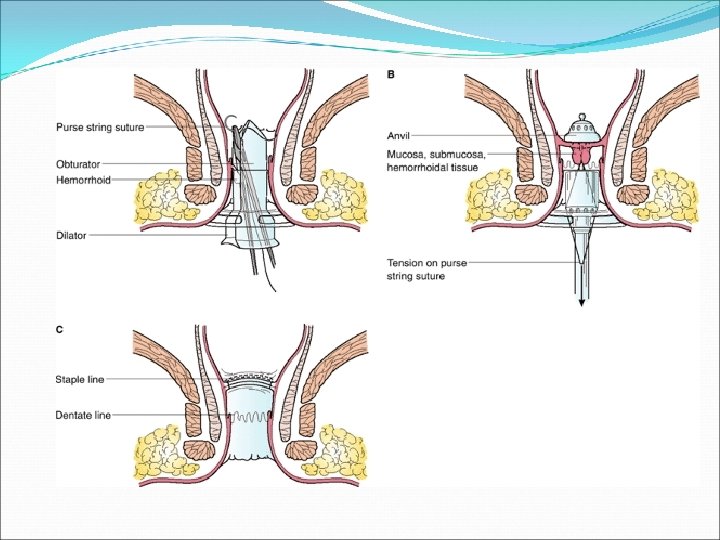
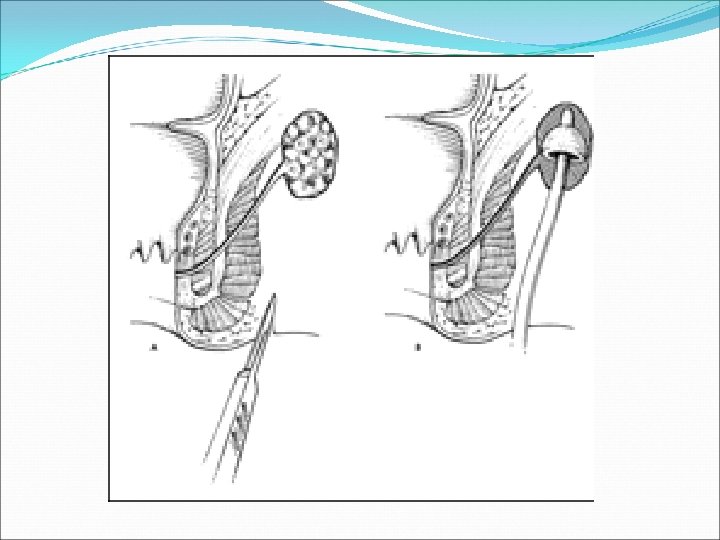
Haemorrhoids Internal H. Treatment : Conservative Grade 1&2 • Dietary modification: high fibre diet Measures • • • Stool softeners Bathing in warm water Topical creams NOT MUCH VALUE Minimally invasive Indicated in failed medical treatment and grades 3&4 • injection sclerotherapy • Rubber band ligation • Laser photocoagulation • Cryotherapy freezing • Stapled haemorrhoidectomy Surgical Indications: 1. Failed other treatments 2. Severely painful grade 3&4 3. Concurrent other anal conditions 4. Patient preference
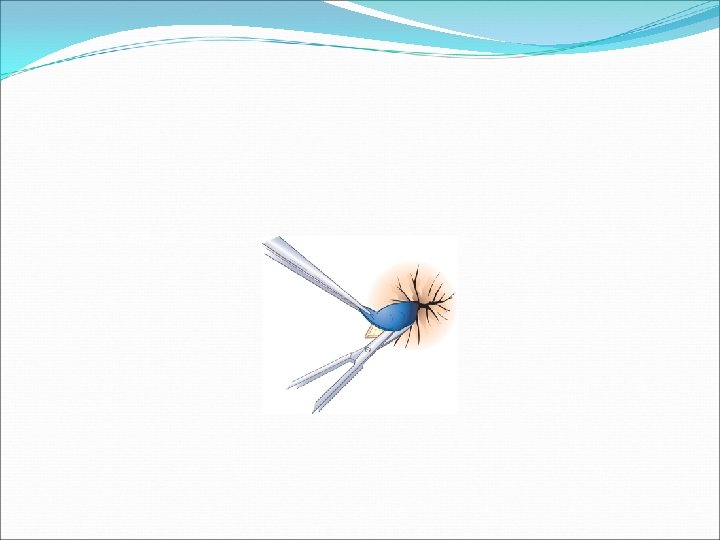

Haemorrhoids External H. Treatment : If presentation less than 72 hours: Enucleate under LA or GA Leave wound open to close by secondary intension Apply pressure dressing for 24 hours post op If more than 72 hours: Conservative measures

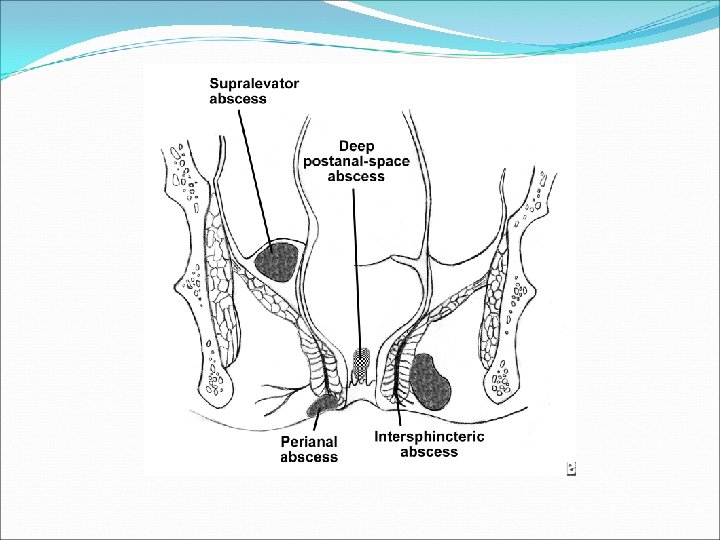
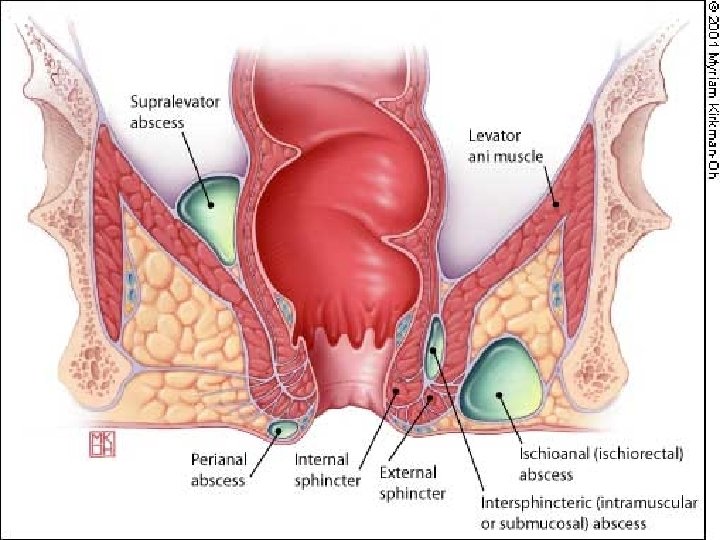
Perianal Fistula and Abscess 5% Perianal abscess almost always arise from a fistulous tract. It is an infection of the soft tissue surrounding the anus. Aetiology & Pathogenesis: • 4 -10 glands at dentate line. • Infection of the cryptglandular epithelium resulting from obstruction of the glands. • Ascending infection into the intersphincteric space and other potential spaces. • Bacteria implicated: E. Coli. , Enterococci, bacteroides Other causes: • Crohn • TB • Carcinoma, Lymphoma and Leukaemia • Trauma • Inflammatory pelvic conditions (appendicitis) 60 % 5% Ischiorectal 20% Intersphincteric suprasphincteric Trans-sphincteric extrasphincteric

Pathophysiology Glandular secretion stasis Infection & suppuration Anal crypts obstruction abscess formation

Perianal Abscess
 and fever • Tender,")
Perianal Abscess Clinical presentation Perianal • Perianal pain, discharge (pus) and fever • Tender, fluctuant, erythematous subcutaneous lump Ischio-rectal • Chills, fever, ischiorectal pain • Indurated, erythematous mss, tender Intersphincteric Supralevator • Rectal pain, chills and fever, discharge • PR tender. Difficult to identify are. EUA needed

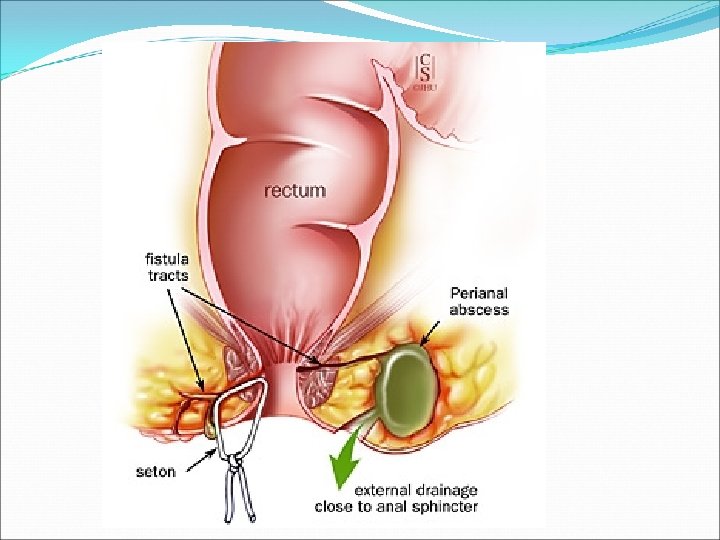
Peri-anal Fistula Clinical presentation Follow 40 -60% of perianal abscess and cryptgland infections Presentation: External openings Purulent discharge Blood Perianal pain Also associated with: • IBD • Malignancy • TB/ Actinomycosis • Diverticular disease Godsalls law Anterior: drain straight Posterior: drain curved to anorectal midline

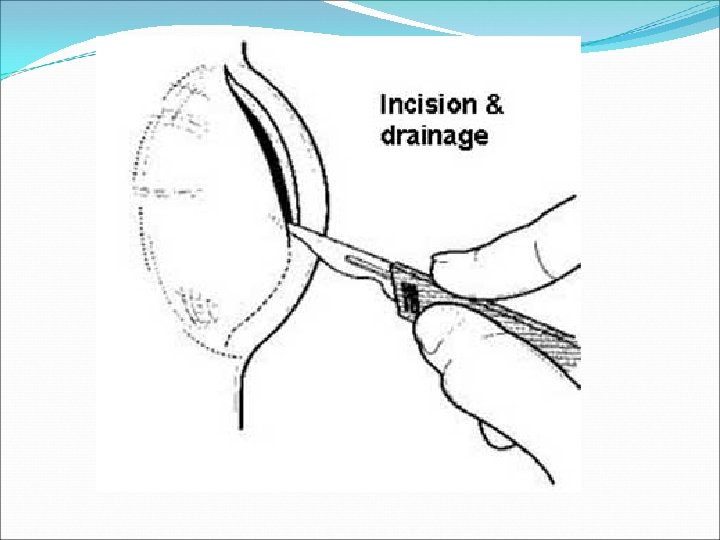
Perianal Abscess Management Aim: adequate drainage of abscess preservation of sphincter function Abscess Perianal Ischio-rectal Intersphincteric Supralevator Treatment • Incision and drainge de-roof cavity • pack with gauze and iodine • IV AB, sitz bath tid, laxitives and anlgesia • F/U for fistula • I&D through interspgincteric plane. • Treat the underlying cause * Preop: full lab evaluation *Always perform Examination under GA ( EUA) and obtain a biopsy.





Perianal fistula Managment Aim: Define anatomy Eliminate tract preservation of sphincter function Fistula Perianal Treatment • Fistulotomy vs fistulectomy Trans/Extra/Supra • Complex treatments using seton sphincteric * Preop: full lab evaluation *Always perform Examination under GA ( EUA) and obtain a biopsy.

Anal Fissure Linear tears in the anal mucosa exposing the internal sphincter 90% are posterior Caused mainly by trauma ( hard Stool). Followed by increased sphincter tone and ischemia. Other causes: IBD, Ca, Chronic infections

Anal Fissure Clinical Assessment Acute • Sever acute pain • Fresh blood spotting • Clean linear tear. Chronic • Pain mild to moderate • More than 6 weeks • Hypertrophied Int. sphincter • Skin tag • Granulation around the edge

Anal Fissure Treatment Conservative • High fibre diet • Medical sphincterotomy: –GTN –Ca channel blockers –Butulinum toxins Surgical Lateral sphincterotomy

Pilonidal Sinus Pathogenesis: A sinus tract at natal cleft resulting from: Blockage of hair follicle Folliculitis Abscess followed by sinus formation. Hair trapping Foreign body reaction The sinus tract is cephald Associated with: Caucasians Hirsute Sedentary occupations Obese Poor hygeine

Presentation & Treatment Acute abscess Incision and drainage Recurrence: 40% Chronic Pain and discharge Wide local excision • with primary closure or • closure by secondary intension Recurrence: 8 -15% Also found: umbilicus, finger webs, perianal area

History Age Hemorrhoids common all ages but are uncommon below the age of 20 years. Perianal haematomata occurs at all ages Fissure-in-ano-(acute) quite common in children Anorectal abscess common between the ages of 20 and 50 years. Pilonidal sinus rare before puberty and in people over 40 years.

History Sex Hemorrhoids common in both sexs Perianal haematomata occurs at all ages Fissure-in-ano common in men Anorectal abscess more common in men Pilonidal sinus more common in men Prolapse of rectum more common in women

History Principal symptoms of rectal and anal conditions: Bleeding Pain Tenesmus Change in bowel habit Change in the stool Discharge pruritis

History - Bleeding Can be fresh or altered Example of altered is melaena Black tarry stool Recognizable blood may appear in four ways: Mixed with faeces On the surface of the faeces Separate from the faeces: after/unrelated to defaecation On the toilet paper after cleaning

History - Bleeding Diagnosis of anal conditions which present with rectal bleeding Bleeding but no pain: Blood mixed with stool = ca of colon Blood streaked on stool = ca of rectum Blood after defaecation = hemorrhoids Blood and mucus = colitis Bleeding + pain = fissure or carcinoma of anal canal The most common causes of rectal bleeding in patients who visit primary care physicians are hemorrhoids, fissures and polyps.

History – Anal pain Diagnosis of anal conditions which present with pain Pain alone Fissure ( pain after defaction) Proctalgia fugax (pain spontaneously at night) Anorectal abscess Pain with bleeding Fissure Pain with a lump Perianal haematoma Anorectal abscess Pain, lump and bleeding Prolapsed haemorrhoids/rectum Carcinoma of the anal canal

Anorectal examination One of the most important examinations in a patient with abdominal disease. Still its the least popular segment of the entire physical examination. Should not be omitted from your examination, especially in middle-aged and older patient, why? risks missing an asymptomatic carcinooma Can be done in numerous positions: Left Lateral (Sims’) position. The usual position when the patient is in bed. Turn patient on to left side with pelvis vertical. Ask patients to draw knees up to chest with buttocks on the side of the couch The Knee-elbow position. Patient kneeling on couch, resting on elbows, of particular use when palpating the prostate and seminal The Dorsal Position. This position with the patient lying on the back with right leg flexed is useful when the patient is in severe pain, and movement is contra-indicated. Enables assessment of rectovesical pouch in abdominal emergencies. Lithotomy. best position for examination but not always available.
. Rectal prolapse. Anal fissure.")
Anorectal examination External inspection: Piles. Skin tags (normal, Crohn's, hemorhoids). Rectal prolapse. Anal fissure. Fistula. Anal warts. Carcinoma. Signs of incontinence, diarrhea. External inspection (straining): Ask pt. to strain. Rectal prolapse upon straining. Hemorrhoid prolapse. Incontinence. Ask if straining is painful

Anorectal examination palpation Lubricate index finger. Insert finger slowly, assessing external sphincter tone as enter. Male: palpate prostate [anterior of rectum]: • Hard nodule (prostate cancer). • Tender (prostatitis). Female: palpate cervix [anterior of rectum]: • Mass in pouch of Douglas. Rotate finger, palpating along left, posterior, right walls. Withdraw finger. Wipe lubricant off pt. Ask if was significant pain during examination.

Anorectal examination Inspect withdrawn fingertip for: Blood, melaena Stool color Pus Mucous. Other examination would be systemically preformed and depends on the case you have e. g swelling such as anorectal abscess or ulcers.

Acute Ano-rectal Conditions

Rectal prolapse is the abnormal movement of the rectal mucosa down to or through the anal opening. Mucosal prolapse Complete rectal prolapse

Rectal prolapse Mucosal prolapse is more often seen in children below 3 yrs of age following an attack of diarrhoea or whooping cough , and if it occurs in adult is usually associated with haemrrhoids. Complete rectal prolapse is seen more commonly in elderly women who have a habit of excessive straining during defecation. Rectal prolapse is often associated with other conditions such as: * Pinworms(Enterobiasis) * Cystic fibrosis * Malnutrition and malabsorption (Celiac disease) * Constipation * Prior trauma to the anus or pelvic area

Rectal prolapse Symptoms: The main symptom is a protrusion of a reddish mass from the anal opening, especially following a bowel movement. Treatment : * Treating the underlying condition * In children, Conservative treatment * The rectal mass may be returned to the rectum manually * Surgical correction for complete rectal prolapse Complications * Constipation * Malnutrition or malabsorption * Other complications of underlying condition

Proctitis An inflammation of the rectum causing discomfort, bleeding, and occasionally, a discharge of mucus or pus, And the anus may also be involved. Causes: * Sexually-transmitted diseases(gonorrhea, herpes, Syphilis , chlamydia, and lymphogranuloma venereum. * Non-sexually transmitted infections( Beta-hemolytic streptococcus , Amoebic dysentry, Bilharzial dysentry) *Autoimmune diseases (Ulcerative colitis and crohn’s disease) * Tuberculous proctitis * AIDS *Radiation Proctitis * noxious agents

Proctitis Symptoms: pain, discomfort rectal bleeding rectal discharge, pus stools, bloody constipation Tenesmus *Tests: proctoscopy sigmoidoscopy rectal culture

Proctitis Treatment: treatment of the underlying cause usually cures the problem. Proctitis caused by infection is treated with antibiotics specific for the causative organism. Corticosteroid or mesalamine suppositories may relieve symptoms in Crohn's disease or ulcerative colitis.
 A polyp is a lesion that projects into")
Benign tumours of the rectum (POLYPS) A polyp is a lesion that projects into the lumen Polyps are commonly found in vascular organs Polyps bleed easily The rectum and sigmoid colon are common sites of polyps Symptoms and signs of polyps * passage of blood and mucus PR * Rarely obstruction or intussusception

Types of Polyps q. Juvenile Polyps Commonest form of polyps in children Are red pedunculated spheres lesions Can occur throughout large bowel but are most common in the rectum Usually present before 12 years Present with Prolapsing lump or rectal bleeding Have little malignant potential Treated by local endoscopic resection

Adenomatous Polyps Are pedunculated lesions Mainly occur in the rectum and sigmoid colon Are often asymptomatic but may produce anaemia from chronic occult bleeding May give rise to crampy pain May secrete mucus Have malignant potential Treated by colonoscopic polypectomy

Villous Papillomas Are flat, sessile lesions within the rectum Secrete copious amount of mucus producing spurious diarrhoea Present with hypokalemia Significant risk of malignant change Treated by transanal excision of complete lesion If lesion is extensive, mucosal proctectomy and coloanal anastomosis should be done

Familial Polyposis Is an autosomal dominant syndrome diagnosed when a patient has more than 100 adenomatous polyps Due to mutation on long arm of chromosome 5 May be asymptomatic but bleeding, , abdominal pain and diarrhoea are all likely symptoms The risk of devoloping carcinoma is virtually 100% within 15 years The most appropriate treatment is panproctocolectomy with ileal pouch-anal anastomosis
- Slides: 67