Anaesthesia in Renal Failure Nadia van Heerden Kimberley

Anaesthesia in Renal Failure Nadia van Heerden Kimberley Hospital Complex 30 January 2015

OVERVIEW �Kidney Anatomy �Renal Physiology �Anaesthesia for Patients with Kidney Failure �Chronic Kidney Disease �Preoperative Evaluation �Intraoperative Considerations �Postoperative Considerations �Pharmacological considerations

KIDNEY ANATOMY

KIDNEY BLOOD SUPPLY

Kidney Blood Supply �Kidneys are the only organs for which oxygen consumption is determined by blood flow �Renal cortex - extracts little oxygen; high blood flow with mostly filtration function �Renal medulla – high metabolic activity dt solute reabsorption and requires low blood flow to maintain high osmotic gradients – RELATIVELY VULNERABLE TO ISCHAEMIA

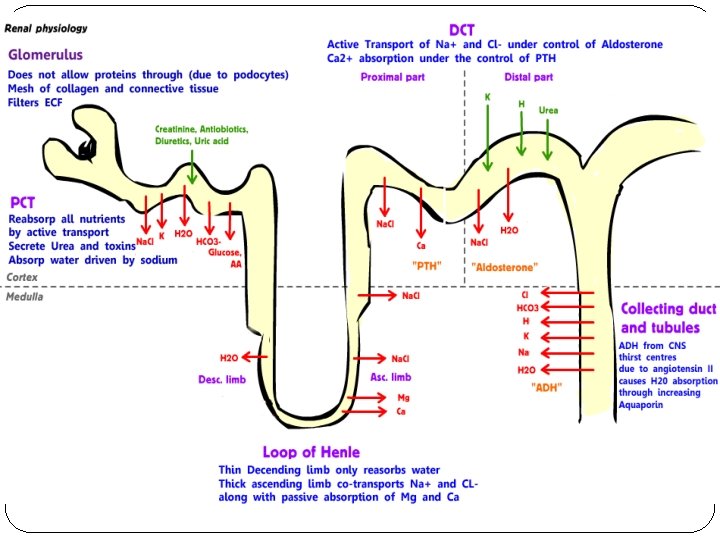
The Nephron: Functional unit of the Kidney � 6 Major Anatomical and functional divisions �Glomerulus �Proximal Convoluted Tubule (PCT) �Loop of Henle: descending thin limb, ascending thick and thin limb �Vasa Recta �Distal Convoluted Tubule (DCT) �Collecting Duct

Countercurrent Mechanism
 enters descending")
Countercurrent System: ESTABLISHING & MAINTAINING MEDULLARY OSMOTIC GRADIENT COUNTERCURRENT MULTIPLIER Filtrate (isotonic) enters descending loop Henle (water permeable; salt impermeable) Filtrate flows from cortex to medulla and water leaves tubule by osmosis (ie filtrate osmolality increases) Ascending loop of Henle epithelium changes to water impermeable and salt permeable Salt leaves ascending limb and dilutes filtrate Urea diffuses from lower portion of collecting duct to contribute to high omolality in medulla DIFFERENT PERMEABILITIES OF 2 LOOPS OF HENLE COOPERATE TO ESTABLISH OSMOTIC GRADIENT IN MEDULLARY INTERSTITIAL FLUID COUNTERCURRENT EXCHANGE Blood in vasa recta continuously equilibrates with interstitial fluid ie more concentrated as it follows descending loop of Henle and less concentrated as it approaches the cortical region PREVENTS DISSIPATION OF MEDULLARY OSMOTIC GRADIENT High porosity and sluggish bloodflow in specialised vessels

Renal Blood Flow � 20% of cardiac output goes to kidney � Clearance: volume of blood that is completely cleared of a substance per unit of time � RPF most commonly measured by PAH clearance � GFR: total amount of filtrate formed per minute by the kidneys �Inulin (fructose polysaccharide) clearance a good measure (freely filtered; not reabsorbed) but not practical �Creatinine (product phosphocreatinine breakdown in muscle) clearance used; tends to overestimate GFR (some creatinine normally secreted by renal tubules) �Cockroft-Gault equation �Factors governing filtration rate at capillary beds � Total surface area available for filtration � Filtration membrane permeability � Net filtration pressure � Ratio GFR to RPF called filtration fraction (FF); normally 20%

GFR �GFR held relatively constant by 3 mechanisms that regulate renal blood flow 1. RAAS (hormonal mechanism) 2. Neural controls (sympathetic nervous system controls) 3. AUTOREGULATION (intrinsic)
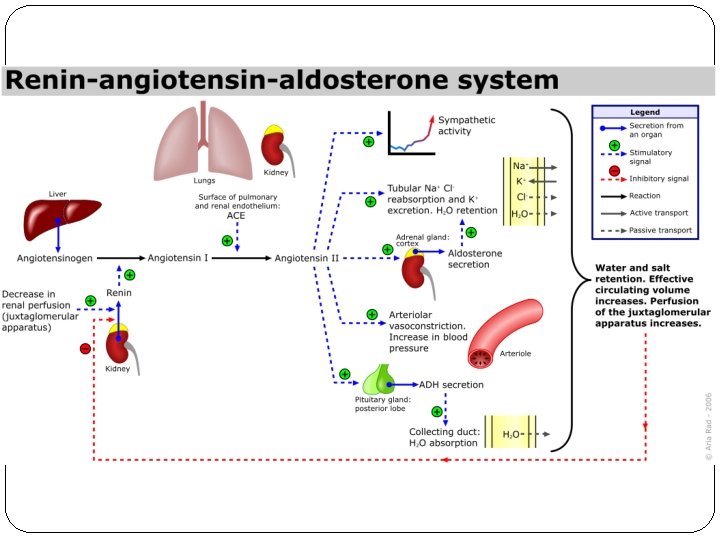

Extrinsic Neural Controls LOW BP IN RENAL BLOOD VESSEL S EXTRINSI C NEURAL CONTROL S Increased systemic BP Increased peripheral resistance GF R Renin release from JG cells in kidney Vasoconstriction of systemic arterioles RAAS Baroreceptor s in bloodvessels of systemic circulation SN S Increased blood volume & systemic BP

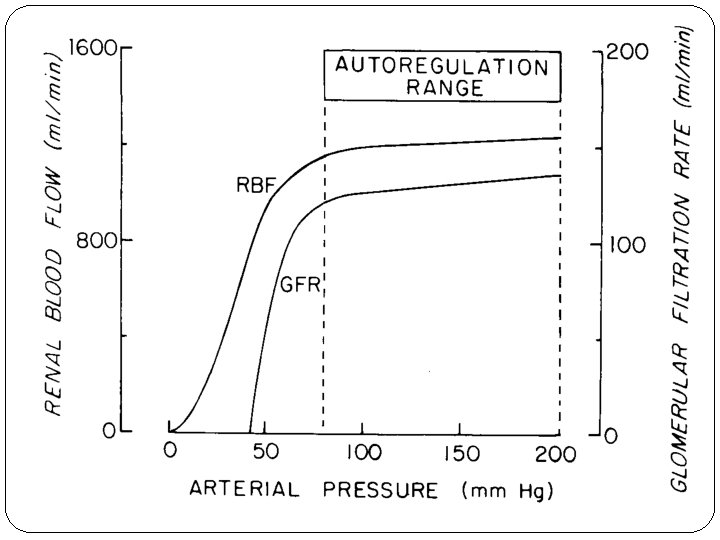
Autoregulation �Kidney can maintain a nearly constant GFR despite fluctuations in in systemic arterial BP �Arterial pressure range from 80 to 180 mm. Hg �Outside autoregulation limits RBF becomes pressure dependent �Directly regulated the diameter of afferent (and lesser extent efferent) arterioles �Mechanism: 2 types of control �Myogenic mechanism � General tendency for vascular smooth muscle to contract when stretched � Increased BP afferent arterioles constrict (decreased blood flow into glomerulus) and decrease in glomerular pressure � Decreased BP dilatation of afferent arterioles and increase in glomerular hydrostatic pressure �Tubuloglomerular feedback mechanism � Directed by macula densa cells of juxtaglomerular apparatus � Located in walls of distal tubules – responds to filtrate flow rate and osmotic signals � Either allows or prevents release of chemicals that produces intense vasoconstriction of afferent arterioles � Eg if macula densa exposed to slow flowing filtrate or low osmolarity filtrate vasodilatation of afferent arterioles promoted ie allows more blood flow into

Main Functions of the Kidneys �Salt & Water Balance or Homeostasis �Toxin Removal �Calcium & Phosphate Homeostasis �Acid Base Homeostasis �Stimulation of Erythropoiesis

Salt & Water Balance �Water Homeostasis �Controlled by ADH: Increase nr of aquaporins within collecting ducts (Facilitates greater water reabsorption) �Sodium Balance � 2 most NB mechanisms: �RAAS: Aldosterone increases NA reabsorption by increases nr of NA channels and Na pumps (DCT and collecting duct) �ANP : Released with atrial stretch (salt &water overload) and Increases Na excretion by INHIBITING the RAAS �Potassium Balance �K freely filtered by glomerulus and most of it reabsorbed by PCT (not respond to differing plasma K concentration) �DCT and collecting ducts regulates K balance �Aldosterone : reabsorption Stimulates K secretion by increasing Na �K-H exchange pump: Collecting duct stimulates pump

A D H

A N P

ALDOSTERO NE

Toxin Removal • 2 Mechanisms: - Filtration - Secretion • Most water soluble toxins e. g creatinine are freely filtered and not reabsorbed • Ie the levels should remain constant and at non-toxic levels in blood unless - Ingestion - Production changes - GFR changes

Calcium & Phosphate Homeostasis

Acid Base Homeostasis

Bicarbonate Reabsorption Distal nephron reclaims any HCO 3 that remains in the filtrate after passing through PCT

Acid Base Balance � Enzyme systems are very p. H sensitive � Excess acid generation by metabolism that body needs to excrete � Vast majority excreted as CO 2 in lungs but NB fraction (phosphate and sulfate ions) excreted by collecting ducts � Bicarbonate main buffer in human body � When filtrate reaches the collecting ducts it is acidic (dt HCO 3 reabsorption and NOT excretion of acid) � H ions are actively secreted by H-K antiporter (urine acidity would increase if H not buffered) � All HCO 3 has been reabsorbed ie H ions are now buffered primarily by ammonia (metabolised glutamine) and filtered phosphate ions

Stimulation of Erythropoiesis

ANAESTHESIA FOR PATIENTS WITH KIDNEY FAILURE CKD Preoperative Evaluation Intraoperative Considerations Postoperative Considerations Pharmacologic Considerations
 increasing worldwide – in USA prevalence of")
CKD � Incidence of ESRD (aka CRF) increasing worldwide – in USA prevalence of ESRD more than doubled between 1990 and 2001 � 4 – Year survival for ESRD patients in UK only 48% � Approximately 26 million Americans have some form of CKD (pre-dialysis kidney disease) and many remain undiagnosed � The CKD patient population fits the “ 2 nd hit injury” paradigm because they have some stable chronic baseline organ dysfunction that is disproportionately worsened when exposed to acute physiologic stress such as hypotension, hypovolaemia, or drug toxicity
 guidelines")
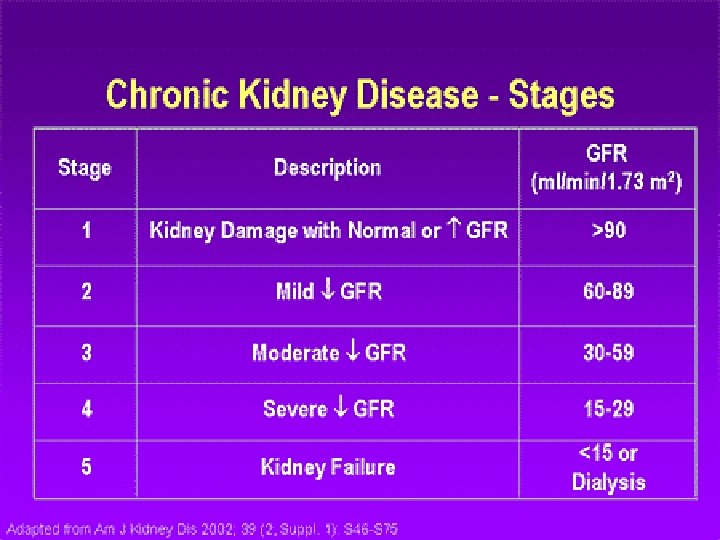
Definition CKD � 2002 National Kidney Foundation Kidney Disease Outcomes Quality Initiative (K/DOQI) guidelines proposed a 5 stage classification for CKD based on GFR �GFR < 60 m. L/min/1, 73 m 2 for > 3 months where there is evidence of kidney damage or �Evidence of kidney damage for > 3 months based on pathologic specimen, imaging or laboratory tests (e. g proteinuria) irrespective of GFR

RIFLE criteria

Aetiology of CKD Diabetic Nephropathy Hypertensive Nephroscler osis Glomerular Disease Interstitial Diseases of the Kidney Vascular Diseases of the Kidney Inherited Kidney Diseases

Pathophysiology of CRF
 effects resulting from �The inability to excrete")
Uraemia �Refers to the multitude of (uncorrected) effects resulting from �The inability to excrete products of metabolism of proteins and amino acids �Impaired wide range of metabolic & endocrine functions of the kidney �Usually seen when GFR <25 m. L/min �GFR <10 m. L/min is dependent on RTT for survival �RTT (renal replacement therapy) �Haemodialysis �Haemofiltration �Peritoneal dialysis �Renal transplantation
")
FLUID OVERLOAD & CHF HYPERTENSION (Na & H 2 O retention // altered RAAS) PERICARDITIS (haemorrhagic uraemic) ARRYTHMIA (IHD & electr abn) CONDUCTION BLOCKS VASCULAR CALCIFICATION (increased Ca-PO 4 product & PTH conc. bacterial endocarditis more common in RRT pt) ACCELERATED ATHEROSCLEROSIS HYPERVENTILATION • May require increased MV to compensate for metabolic acidosis INTERSTITIAL OEDEMA • Increased alveolar to arterial gradient risk hypoxaemia ALVEOLAR OEDEMA • Permeability alv-cap membrane PLEURAL EFFUSION CARDIO VASCULAR URAEMI A ANAEMIA (Hb 6 – 8 g/d. L) • Decreased EPO production • GIT blood loss • Haemodilution • BM suppression (rec infxn) PLATELET DYSFUNCTION • Increased bleeding time • Consider when choosing regional anaesthesia LEUCOCYTE DYSFUNCTION • Increased susceptibility infxn HAEMAT O LOGICAL PULMO NARY

PERIPHERAL NEUROPATHY & AUTONIMIC NEUROPATHY • Delayed gastric emptying • Postural hypotension • Silent Myocardial Ischaemia DIALYSIS PATIENTS • Dialysis dementia • Dysequilibrium syndrome GASTRO INTESTINA L ANOREXIA & NV (malnutrition) DELAYED GASTRIC EMPTYING (RSI) HYPERACIDITY (PUD – PPI) MUCOSAL ULCERATIONS (urea mucosal irritant) HAEMORRHAGE ADYNAMIC ILEUS NEURO LOGICAL UREMI A MET A BOLI GLUCOSE INTOLERANCE • Peripheral insulin resistance SECONDARY HYPERPARATHYROIDISM • Metabolic bone disease • Osteopenia predispose to # HYPERTRIGLYCERIDAEM IA • Accelerated ENDO atherosclerosis CRINE ACIDOSIS • Less clearance H and HAGMA FLUID & ELECTROLYTE ABN’s • Hyperkalaemia – NB acidosis (avoid hypercarbia in GA) • Sodium balance – NB diuretic use and cardiac function Ca & PO 4 DERANGEMENT

Preoperative Evaluation �Multidisciplinary approach involving anaesthetists, surgeons and renal physicians �Optimise medical condition & address potentially reversible manifestations of uraemia �Cardiorenal syndrome & Cardiovascular Risk �Renal Risk Assessment and Interventions �Dialysis and Renal Transplant Patients

Basic outline of the “Premed” � History & Physical Examination �CVS & Respiratory system evaluation NB ? ? Fluid overload � Visidex (diabetic patients) � Basic bloods �FBC (Hb), U&E (postdialysis), INR/PTT (NB platelet dysfunction in uraemia – count may be normal) � CXR (clinical impression) � ABG �Acid-Base status (Resp. distress); oxygenation; ventilation � ECG � Echo � Blood transfusion – only in severe (symptomatic) anaemia � Consider Anaesthetic Technique

Cardiorenal Syndrome �Pathophysiological disorder of the heart and kidneys wherein the acute or chronic deterioration of one organ results in acute or chronic deterioration of the other �Classified into 5 types

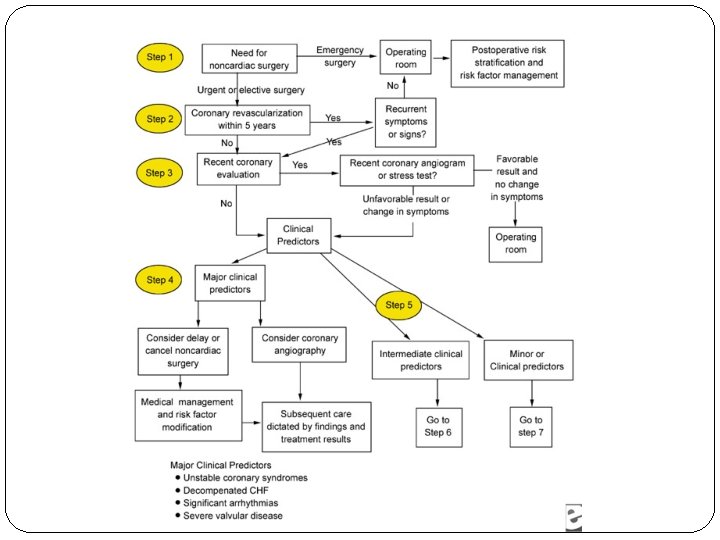
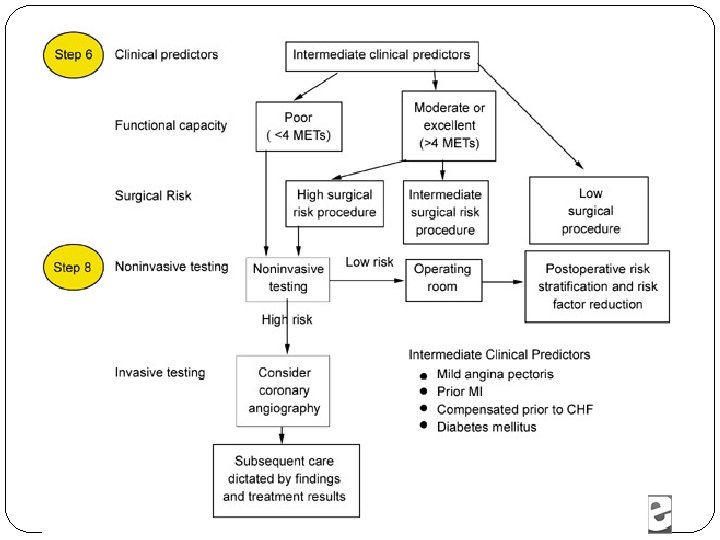
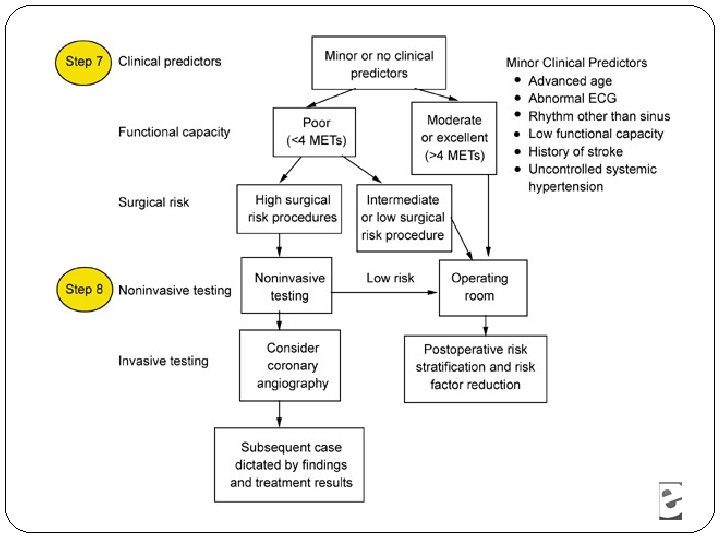
Cardiovascular Risk �High prevalence of cardiovascular disease and increased perioperative morbidity �Cardiovascular risk assessment according to ACC/AHA guidelines �Surgical risk for noncardiac procedures �Major risk factors (before elective surgery) �Risk profile for surgery �Risk with intended procedure �Decompensated HF or unstable coronary syndromes postpone procedure until medical management optimised �Intermediate/Minor risk factors (before elective noncardiac surgery) �Functional capacity (METs- metabolic equivalents or tasks) � Self-reported/treadmill testing � 6 METs – better prognosis; good functional capacity – proceed to
 �Detailed Background History �Co-morbidities �Duration CKD �Usual")
Renal Risk Assessment and Interventions (non-dialysis pt) �Detailed Background History �Co-morbidities �Duration CKD �Usual fluid intake �Usual daily urine output �Renal function (baseline & current) �Urea & Creatinine �GFR �Electrolyte concentrations �Na �K

Renal Risk Assessment and Interventions Cont. . � Uncomplicated cases �Euvolaemic, �Responsive to diuretic therapy with �No significant electrolyte abnormalities and �No bleeding tendencies � Complicated cases �Oedema, CHF, Pulmonary congestion or responsive to diuretic therapy cardiovascular evaluation �IF Cardiovascular evaluation OPTIMAL – fluid overload can be attributed to CKD �Consider combination diuretics to achieve euvolaemia prior to surgery � Consider preoperative dialysis �Diabetes – greater tendency to volume overload or cardiovascular disease �Advanced CKD with diuretic resistance and progressive

Dialysis and Renal Transplant Patients �Extra Considerations �Dialysis adequacy �Preoperative dialysis needs �Usually 12 -24 hr prior surgery � Fluid depletion & redistribution, electrolyte disturbances & residual anticoagulation from heparinisation �Post dialysis U&E prior surgery – NB intraoperative cardiac dysrythmias �Postoperative dialysis timing �Dosage requirements for all medications

Intraoperative considerations: Kidney Failure � Monitoring �Risk thrombosis – BP cuff not on arm with AV fistula �Continuous intraarterial BP in uncontrolled HPT � Induction �RSI in patient with N&V or GI bleed �Induction dose adjustment � Anaesthesia maintenance �Control BP with minimal deleterious effect on CO �Volatile agents, propofol & opioids (NB morphine effect prolonged) �Ventilation control to avoid respiratory acidosis and alkalosis � Hypercarbia may exacerbate existing acidaemia circulatory depression & increase in serum potassium � Fluid therapy �Replace insensible losses in superficial operations involving minimal tissue trauma �Procedures associated with major fluid losses � Isotonic crystalloids, colloids or both � Ringers Lactate contains potassium NB Hyperkalaemic patients

Postoperative Considerations � Emergency surgery � Postoperative cardiac assesssment � Lack preoperative evaluation � Diagnosis of postoperative MI should be based on combination of clinical, laboratory & ECG evidence � Environment � Normal ward � High Care/ICU � Analgesia � Regional anaesthesia reduces requirement for systemic analgesic drugs � Epidurals potentially reduced incidence of postop respiratory complications and VTE events � Systemic anaglesia � WHO pain ladder � PO vs IMI vs PCA (IV) � Immune Suppression with transplants – postoperative sepsis risk increase

Pharmacological Considerations �INTRAVENOUS AGENTS �Induction Agents �Muscle Relaxants �Reversal Agents �Benzodiazepines �Opioids �INHALATION AGENTS �Volatile Agents �Nitrous Oxide �OTHER

Induction Agents PROPOFOL & ETOMIDATE Pharmacokinetics minimally affected and pharmacodynamics unchanged Changes in volume distribution and mental state Decreased induction dose required BARBITURATES Pharmacokinetics unchanged but Increased sensitivity dt increased free circulating barbiturates (decreased protein binding) and acidosis increases entry into brain by increasing nonionised fraction KETAMINE Pharmacokinetics minimally changed Hepatic metabolites may depend on renal excretion and can potentially accumulate

Muscle Relaxants SUCCINYLCHOLINE Safe if HYPERKALAEMIA absent CISATRACURIUM & ATRACURIUM DRUG OF CHOICE; plasma ester hydrolysis, nonenzymatic Hoffman elimination VECURONIUM Primary hepatic metabolism, 20% eliminated by kidneys. If use >0, 1 mg/kg dose prolonged effect ROCURONIUM Hepatic elimination but prolonged action in kidney disease reported. Can be used if appropriate NM monitoring available PANCURONIUM 60 – 90% dependant on renal excretion NEOSTIGMINE Renal excretion. Halflife prolonged. Inadequate reversal often related to other effects (“recurarizaton’) ATROPINE & GLYCOPYROLLATE Safe for use. Repeated doses potential for accumulation (50% drug excreted in urine) Reversal Agents
 may have greater activity than parent drug and")
Opioids MORPHINE Active metabolites (morphine-6 -glucoronide) may have greater activity than parent drug and may accumulate Start at lower suggested dosage and titrate dosage upwards slowly and increase dose intervals FENTANYL REMIFENTANYL ALFENTANYL Inactivated by liver and excreted by urine Significant accumulation does not occur No active metabolites Benzodiazepines MIDAZOLAM & DIAZEPAM Hepatic metabolism with urine elimination Active metabolites accumulate Protein bound ; increased sensitivity in hypoalbuminaemic patients Dose reduction 30 – 50%

Inhalation Agents �Not dependent on renal function �Sevoflurane and Enflurane may produce nephrotoxic fluoride ions �Some physicians avoid use in lengthy procedures

Other PHENOTHIAZINES Pharmacokinetics minimally altered but potentiation of central depressant effect can occur H 2 RECEPTOR BLOCKERS Depend on renal excretion Dose reduction required PPI Dose adjustment not required METOCLOPRAMIDE Accumulates in kidney failure DOLASETRON Dose adjustment not required NSAIDS Avoid in kidney disease LOCAL ANAESTHETICS Decreased duration of action Maximum dose to be decreased by 25% due to decreased protein binding and lower CNS seizure threshold

Renal Protection: Pharmacological Interventions � Dopamine � Volume management by increasing. UO � Evidence does not support “renal protective effect” � Loop Diuretics – Furosemide � Used to preserve intraoperative UO – high doses in ARF reduce need for dialysis (no improvement in mortality) � “Protective effect” only demonstrated in rodent models � Osmotic Diuretic Mannitol � Old data in kidney transplants – impaired renal perfusion with goal of renal protection and maintenance of adequate UO � Recent randomised trial failed to show protective benefit patients undergoing major vascular surgery � ACE inhibitors � No data to support benefit � CCB’s � Data insufficient to support benefit � N -Acetyl Cysteine � Prevention of contrast nephropathy (high risk in CKD) � Combination with adequate hydration � Data fails to show benefit when used as renoprotective agent during major surgery

References � Butterworth JF, Mackey DC, Wasnick JD. Morgan and Mikhail’s Clinical Anaesthesiology 5 th Edition. Ch 29 pg 631 – 652 (Renal Physiology and Anaesthesia) and Ch 30 pg 653 – 670 (Anaesthesia for patients with kidney disease) 2013 The Mc. Graw Hill Companies, Inc. � Marieb EN. Human Anatomy and Physiology 5 th Edition. Ch 26 pg 1013 – 1029 (The Urinary System: kidney physiology) 2001 Pearson Education, Inc publishing as Benjamin Cummings � Mc. Phee SJ & Papadakis MA. Lange Current Medical Diagnosis & Treatment. 2012 Mc. Graw Hill Companies, Inc. � Wallace K. Renal Physiology. Update in Anaesthesia (www. worldanaesthesia. org) � Milner Q. Pathophysiology of chronic renal failure. British Journal of Anaesthesia 2003; 3; 130 – 133 (http: //ceaccp. oxfordjournals. org) � Salifu MO. Perioperative Management of Patients with Chronic Renal Failure. Jun 7 2013 (emedicine. medscape. com/article/284555) � Rang ST, West NL, Howard J, Cousins J. Anaesthesia for Chronic Renal Disease and Renal Transplantation. EAU-EBU Update Series 4 (2006) 246 – 256 � Eilers H, Liu KD, Gruber A, Niemann CU. Chronic kidney disease: implications for the perioperative period. Minerva Anestesiologica 2010; 76: 725 – 736
- Slides: 56