Anaesthesia and the Obese Patient Definitions based on

Anaesthesia and the Obese Patient ��. ��������������
 Definition <18. 5 -24. 9 25 -29. 9 Underweight")
Definitions based on BMI (kgm-2) Definition <18. 5 -24. 9 25 -29. 9 Underweight Ideal Weight Overweight 34. 9– 30. 0 Obesity (class I) 39. 9– 35. 0 Obesity (class II) 40 -49. 9 or 35 -49. 9 with Morbidly Obese (class III) obesity-related comorbidity 50 -59. 9 60 -69. 9 >70 Super Obese Hyper Obese

Morbid Obesity
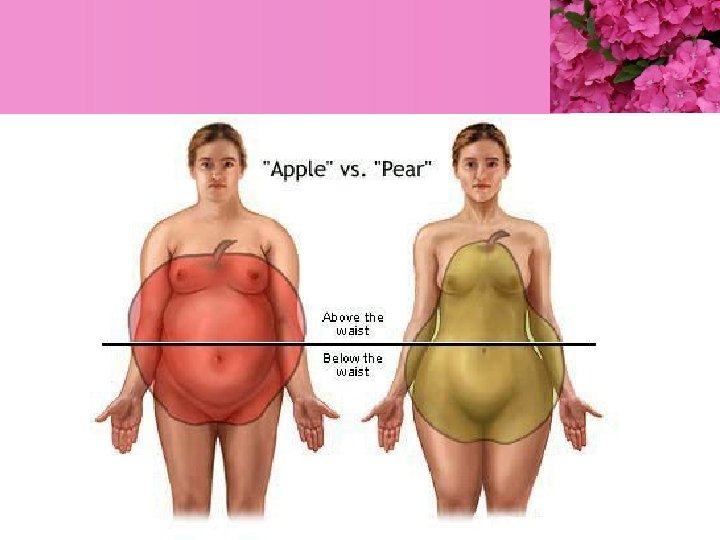

Fat Distribution § Android § § § Central distribution High intra-peritoneal fat content Increased neck circumference Waist-hip ratio >0. 8 women, >1. 0 men Increased morbidity (airway, CVS, metabolic, surgical) § Gynaecoid § Peripheral sites (arms, legs, buttocks)

Interrelationship of cardiovascular and pulmonary sequelae of obesity

Adaptation of the heart to obesity and hypertension


• Medical co-morbidities associated with obesity 1. 2. 3. 4. 5. 6. 7. 8. 9. NIDDM HTM CV DISEASES OSA Liver & Gallbladder diseases Arthritis Colon and postmenopausal breast cancer The risk of dying prematurely increases Quality of life issues: depression, social incompetence, etc.

������� 1 • Underlying – DM – HT – Hypothyriodism

lab ���� �. �. 54 Lab ������ sleep test ����� ��. ����� • • CBC : Hb 14. 1 Hct 45. 4 %plt 357, 000 BUN/Cr 15/0. 7 E’lyte : Na+ 138, K+ 4. 3, Cl- 93, HCO 3 - 39 LFT : Total protein 7. 6, Alb 3. 4 Total billirubin 0. 5, Direct billirubin 0. 2 , SGOT/SGPT 18/19 • FT 4 0. 92 , FT 3 2. 91, TSH 32. 51 • FBS 86



Airway § Difficulty predicted by OSA, short thick neck and BMI § Fatty infiltration pharyngeal wall § pharyngeal wall compliance § Difficult to ventilate by face mask § Rapid desaturation § Consider awake fibreoptic intubation


• Respiratory – – – Airway Obstructive sleep apnea obesity-hypoventilation syndrome Asthma pulmonary hypertension

Obstructive Sleep Apnoea § ���������� pharyngeal collapse occurring during sleep § Airflow ���� , ongoing effort, closed airway § ��� >10 s, >5/hour, >30/night § Snoring, daytime somnolence, headaches § Hypoxaemia, 2˚polycythaemia, systemic vasoconstriction, hypercarbia, pulmonary vasoconstriction, RVF

• Hypopnea ���������� 50% ��� airflow ��� >10 seconds, ���� ≥ 15 seconds ���������� sleep ���� Sp. O 2 ���� 4% • The apnea-hypopnea index – – ����� severity of OSA 30< signifies severe OSA 5 to 15 mild OSA 16 to 30 moderate OSA

Pathophysiology - Respiratory • Fat accumulation ��� thorax ��� abdomen – – – ������� chest wall ��� lung compliance ������������������������� work of breathing Lung capacity ����������� • Polycythemia ������� chronic hypoxemia �������� total blood volume.

Pathophysiology - Respiratory § O 2 consumption, CO 2 production § +/- chronic hybercarbia with renal compensation and altered CO 2 sensitivity § FRC, VC, (A-a) O 2, shunt § Airway closure (CC greater than FRC) § chest wall compliance and lung compliance work of breathing

Asthma § § Multiple factors Acid reflux and micro aspiration Sleep apnoea and partial obstruction Peripheral airway closure sheer stresses proinflammatory response § Bariatric surgery 80 -100% resolution


BP 159/66 EKG : sinus arrhythmia Spo 2 room air 87 -91% ��������� 1 �� �� O 2 cannula ���� Functional class II-III

• Cardiovascular – – – – – Dysrhythmias atherosclerosis cardiac failure coronary artery disease peripheral vascular disease sudden cardiac death systemic hypertension thromboembolism varicose veins

Pathophysiology - Cardiovascular § § § § blood volume + cardiac output ventricular workload myocardial fat content + contractility Endothelial dysfunction + vascular resistance 50% moderate HT, 5 -10% severe HT +/- progressive PVR and PAP Progresses to RVF. Oedema and hepatic congestion


������� 2 • Lab �. �. 54 – CBC : Hb 14. 7 Hct 43. 7 Plt 291, 000 – BUN/Cr : 9/0. 7 – E’lyte : Na+ 136, K+ 3. 9, Cl- 103, HCO 3 - 27 – LTF : TP 7. 8, Alb 3. 7, T billi 0. 4, D billi 0. 1 SGOT/SGPT 48/49, ALP 105


Spo 2 Room air 99% HR 98/min BP 130/100 mm. Hg
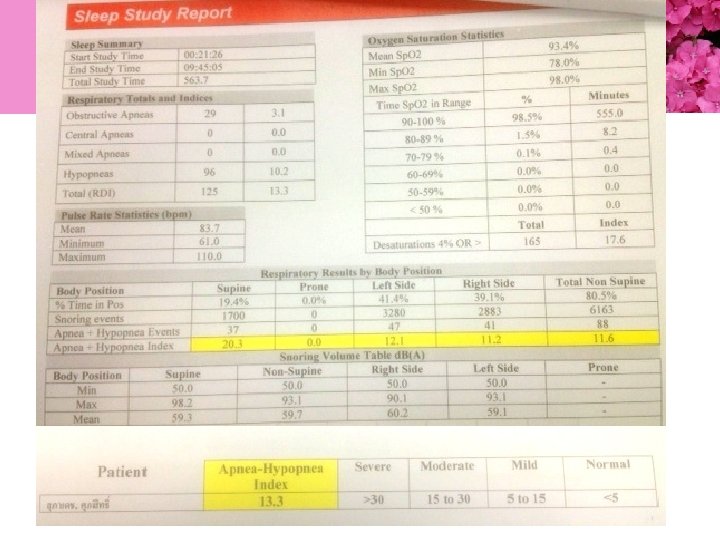

• The apnea-hypopnea index – ����� severity of OSA – 30< signifies severe OSA – 5 to 15 mild OSA – 16 to 30 moderate OSA

������� 3 • Lab 29�. �. 55 – CBC : Hb 16 Hct 45. 7 %Plt 268, 000 – BUN/Cr : 13/0. 85 – E’lyte : ����� – LTF : TP 7. 5, Alb 4. 5, T billi 1. 0, D billi 0. 1 SGOT/SGPT 27/52, ALP 82 – FBS 105


BP 152/95 mm. Hg PR 94 /min

Gastrointestinal Comorbidity § Type 2 diabetes § intra-abdominal pressure § FRC, aortocaval compression, tissue perfusion, risk abdo compartment syndrome § Fatty liver, steatohepatitis, cirrhosis § Hiatus hernia, gastro-oesophageal reflux § Hyperlipidaemia

Musculo-skeletal and Other § § § § Osteoarthritis Compression fractures Increased risk of injury Urinary incontinence Skin infections, candidiasis, poor hygiene Varicose veins Lymphoedema

����� • Endocrine/metabolic – Diabetes mellitus, dyslipidemia, hyperinsulinemia, hypothyroidism, insulin resistance, metabolic syndrome • Genitourinary – End-stage renal disease, macrosomia, menorrhagia, preeclampsia and eclampsia, prostate cancer, urinary incontinence • Neurologic – Carpal tunnel syndrome, pseudotumor cerebri, stroke • Hematology – Hypercoagulability, polycythemia • Psychology/psychiatry – Depression, reduced self-esteem, social stigma

 �������� loading dose")
Pharmacology • ������ dose �� ������� – volume of distribution (VD) �������� loading dose – clearance ����� maintenance dose • ������������ fat ������ lean tissues ���� loading dose ���� LBW • �������� adipose ��� lean tissues dose ������ TBW

Specific Intravenous Agents • Thiopental : – Induction: LBW – highly lipophilic ����� larger VD ������� • Propofol. – – – – Induction: LBW Maintenance infusion: TBW Highly lipophilic High hepatic extraction and conjugation relates to TBW Total clearance and VD at steady state correlate with TBW Negative cardiovascular effects High affinity for well perfused organs

Neuromuscular Blocking and Reversal Agents • Succinylcholine : TBW – ������ extracellular fluid compartment ������ – Pseudocholinesterase activity ���������� • Rocuronium : LBW – Faster onset and longer duration when dosed according to TBW – Pharmacokinetics and pharmacodynamics ����������� • Vecuronium : LBW – Prolonged action when dosed according to TBW – Pharmacokinetics and pharmacodynamics �����������

Neuromuscular Blocking and Reversal Agents • Atracurium : LBW – VD, absolute clearance, and elimination half-life unchanged by Unchanged dose per unit body weight without prolongation of recovery because of organindependent elimination • Cis-atracurium : LBW – Pharmacokinetics similar to atracurium but prolonged duration of action when dosed according to TBW

Opioids • Fentanyl : LBW – Fentanyl dosing ������� “pharmacokinetic mass” ��������� clearance – ������ dose����� TBW ��� overestimates • Sufentanil : LBW – ���� VD ��� prolonged elimination half-life ������� degree of obesity – ��� Overestimation of plasma concentration ��� BMI >40 kg/m 2 • .

Opioids • Remifentanil : LBW – Pharmacokinetics similar in obese and nonobese patients – Systemic clearance and VD corrected per kilogram of TBW is significantly smaller in the obese patient. – Consider age and lean body mass for dosing

highly selective α 2 -adrenergic agonist • Dexmedetomidine : TBW – – sedative-hypnotic, anesthetic-sparing sympatholytic properties Lacks significant effect on respiration Very good analgesic adjuvant in the morbidly obese patient

Benzodiazepines • ������������ highly lipophilic drugs with a larger VD in obese patients • Midazolam – ���� short acting ����� prolonged sedation ���������� initial doses �������������

Preoperative Considerations • Preoperative Evaluation – ������� cardiorespiratory systems and the airway – ������������� – ����� systemic hypertension, pulmonary hypertension • signs of right and/or left ventricular failure • ischemic heart disease. – Signs of cardiac failure • elevated jugular venous pressure, added heart sounds, pulmonary crackles, hepatomegaly, and peripheral edema �����������

PREOPERATIVE EVALUATION CV Systems. v v v The degree of cardiac abnormality is correlated with the degree of obesity. LV dysfunction is often present in young asymptomatic patient HTN Increased Pre-load & After-load Increased PAP (dyspnea, fatigue, syncope). Pulmonary System. v v v O 2 consumption & CO 2 production increased WOB increased Chest wall compliance & FRC are low.
 Tolerance of exercise and ability to")
PREOPERATIVE EVALUATION 1. CV & RESPIRATORY SYSTEMS a) Tolerance of exercise and ability to lie flat. b) Symptoms of sleep apnea should be sought. 2. Airways. Number of abnormalities may exist a) Limitation of extension and flexion of the C-spine. b) Restricted mouth opening from submental fat. c) Large tongue. d) Redundant intra oral tissue. e) Thyromental distance should be assessed. f) Infantile type anterior laryngeal opening. 3. Use of diet tablets (some of them cause valvular regurgitation or pulmonary HT).

PREOPERATIVE EVALUATION 4. Obesity Hypoventilation Syndrome. Pickwickian syndrome: Obesity, excessive daytime sleepiness, snoring cor Pulmonale. a) Hypercapnia b) Severe hypoxemia c) Periodic breathing d) Biventricular enlargement (RT>LT) e) Dependent edema. f) Polycythemia. Pulmonary edema. 5. Metabolic Changes Patient scheduled for surgery following previous Bariatric surgery may have chronic metabolic changes.
")
Preoperative Assessment § § § Anaesthetic history Details of Comorbidities Drug history (appetite suppressants) Airway (MP, neck extension, circumference) Ability to tolerate supine position Routine and specific investigations (may include baseline ABG, lung function tests, sleep studies, Echo, cardiac cath and PA pressure studies)

PREOPERATIVE EVALUATION GI System. v v No difference in gastric volume or PH between lean and obese surgical patient. NIDDM and Gastroparesis. Fatty Liver w or w/o liver dysfunction is common. Gall bladder disease is also common.
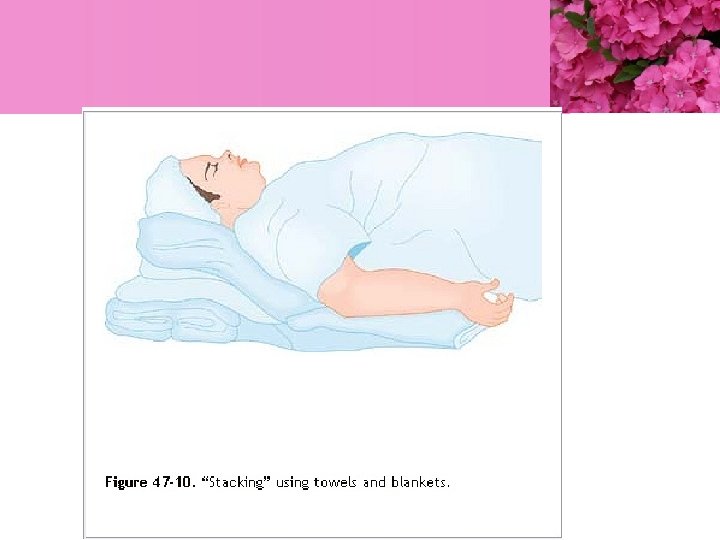

Troop elevation pillow


• Video laryngoscope • ��� King Vision ���

TRACHEAL INTUBATION v v v Increasing weight or BMI is not a risk factor for difficult laryngoscopy. FOB intubation is rarely necessary. Rapid induction with Propofol &Succinylcholine is the best for establishing an airway. • • Since mask ventilation can be difficult a second person experienced with airway management should be present to assist. LMA should be available and can serve as abridge until an ETT is placed.

VENTILATION v v v VT – 10 -12 ML/KG IW Fi. O 2 up to 1. 0 may be needed High Pi. P will be needed PEEP = 5 cm H 2 O N 2 O is avoided Pneumoperitoneum can displace diaphragm causing the ETT to enter bronchus. HEMODNAMIC CHANGES The RTP may cause pooling of blood and hypotention.


ANESTHETIC CONSIDERATIONS PREMEDICATION v v v Avoid heavy sedation. Medication for chronic HTN No diabetic medication on the morning of surgery Antibiotics & heparine prophylaxis H 2 antagonist, metoclopramide? Monitoring v v NIBP can be obtained from the wrist or ankle. A-line highly recommended. CVP or PA lines? Nerve stimulator: needle electrodes are recommended (surface electrode

ANESTHETIC TECHNIQUE. • OPIOIDS I>V> CONTINUOS INFUSION. • CISATRACURIUM I. V. CONTINUOS INFUSION. • INHALATION ANESTHETIC DEFLURANE. POSTOPERATIVE CONSIDERATIONS. Position: Upper body elevated 30 -45 degree. Oxygenation: Restoration of normal pulmonary function after abdominal surgery may take several days. » » » Nasal or mask O 2. Nasal CPAP Bi. PAP Analgesia: An opioid PCA dosed on the basis of IW NSAIDs

Maintenance § Short acting agents eg sevoflurane, desflurane, remifentanil § Temperature maintenance § Neuromuscular monitoring § Ventilate with PEEP § Pressure areas and skin § Calf compression § Fluids - insensible losses BSA § SV/ pulse pressure optimisation

Recovery § Aim: rapid emergence with good airway control § Risks: loss of airway control, inadequate respiration, aspiration, postop chest complications, CVS stress and instability § Extubate wide-awake and sitting up +/- CPAP recruitment procedure prior to extubation § Appropriate postop environment

Illustration of the Walter Henderson maneuver

Analgesia § Multimodal - paracetamol, NSAIDs, opioids, LA, regional § Paracetamol - central compartment so normal dose, clearance dose frequency § NSAIDs - risk renal dysfunction § Opioids - risk respiratory depression § Regional - higher failure rate

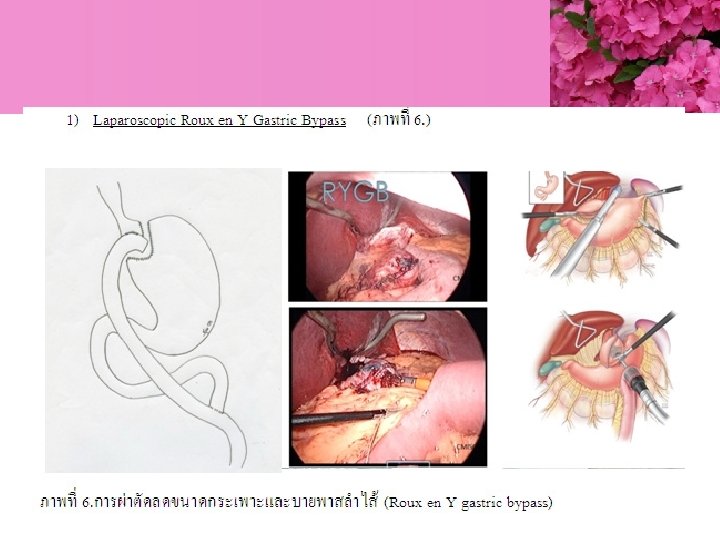
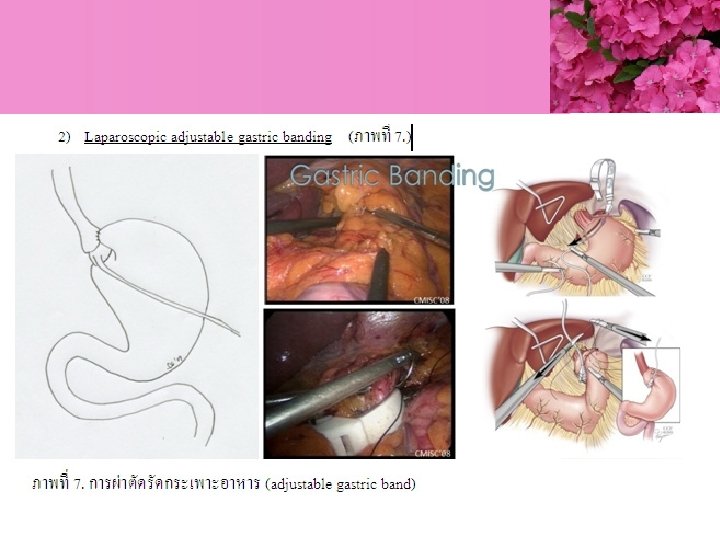
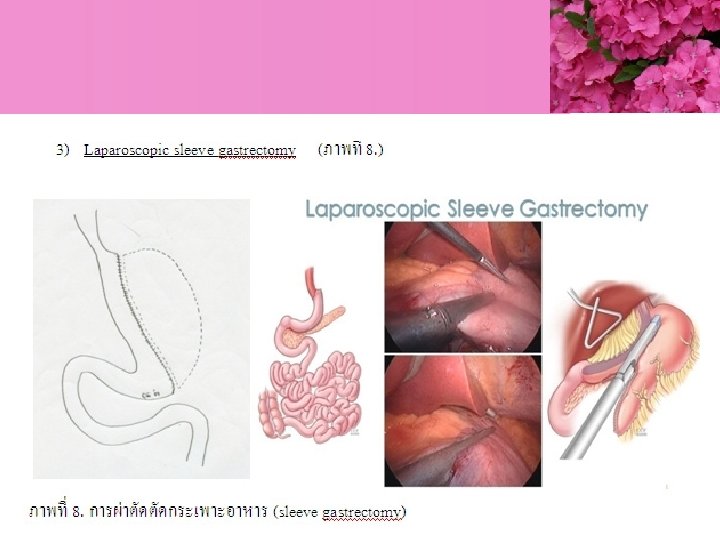
Bariatric Surgery

- Slides: 75