An Introduction to Myofascial Pain Syndrome Content Definition







































 Galvanic Stimulation")





 needle is usually suitable for")











 are extremely common and become a painful")
- Slides: 75
An Introduction to Myofascial Pain Syndrome 神經內科 洪國華
Content • • Definition and examples Clinical characteristics Pathophysiology Clinical importance Diagnosis Treatment Perpetuating Factors
Myofascial Pain syndrome • General definition: A regional pain syndrome of any soft tissue origin • Specific definition: The sensory, motor and autonomic symptoms caused by myofascial trigger points
Example 1: Referred pain patterns and location of corresponding trigger points in the right infraspinatus muscle
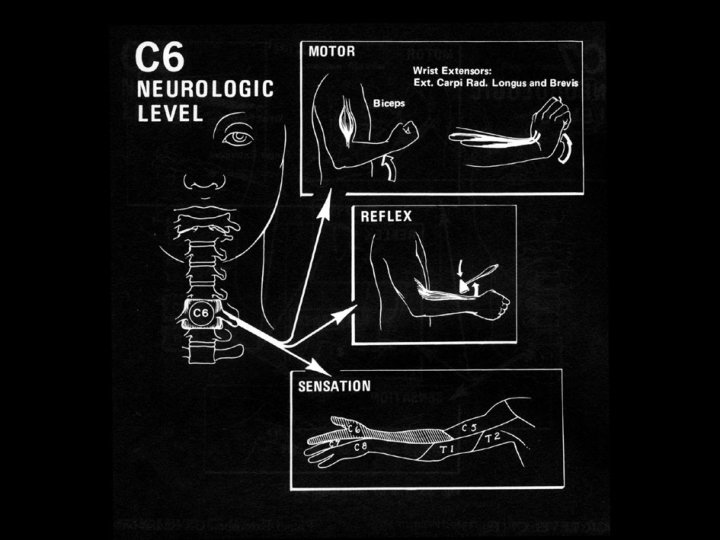
Compression test to test for cervical radiculopathy
The Spurling test to test for cervical radiculopathy
Hand-to-shoulder blade test to test the ROM of infraspinatus
Myofascial trigger points at right infraspinatus muscle
Example 2: Referred pain patterns and location of corresponding trigger points in the right gluteus minimus muscle
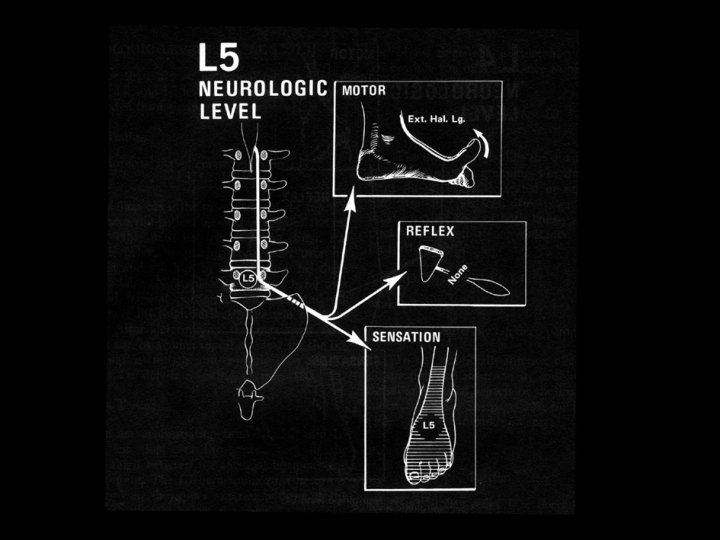
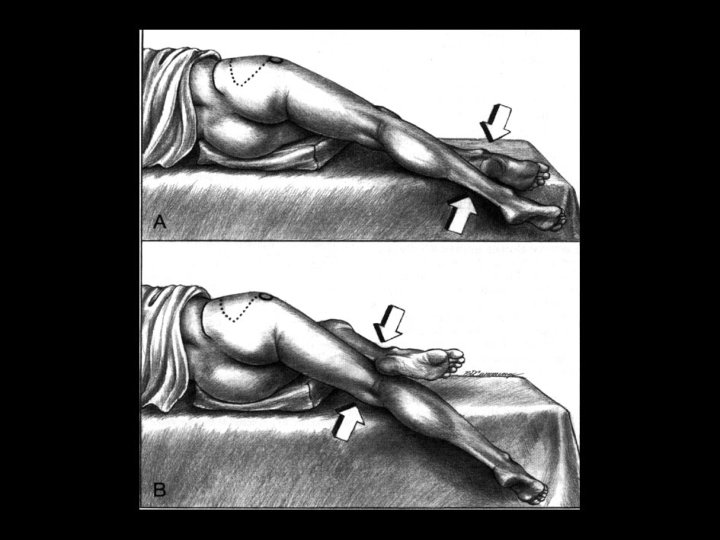
Straight leg raising test to test for sciatica
Myofascial trigger points at right gluteus minimus muscle
Categories of Trigger Points • Active Tr. Ps produce a familiar symptom when the Tr. P is digitally compressed • Latent Tr. Ps produce characteristics of a Tr. P but no spontaneous pain • An active key Tr. P in one muscle can induce an active satellite Tr. P in another muscle
Key Tr. Ps Satellite Tr. Ps (prone to develop in muscles within pain reference zone of key Tr. Ps)
Pain Complaint • Poorly localized, regional, aching pain in subcutaneous tissues, including muscles and joints • More likely to develop in sedentary workers who are prone to intermittent orgies of vigorous physical activity
Neurologic dysfunction • Sensory: Numbness or paresthesia • Proprioception: Imbalance, dizziness • Autonomic: Abnormal sweating, pilomotor activities • Motor: Spasm, weakness, loss of coordination and decreased work tolerance • Sleep disturbance
CNS interactions with a Tr. P
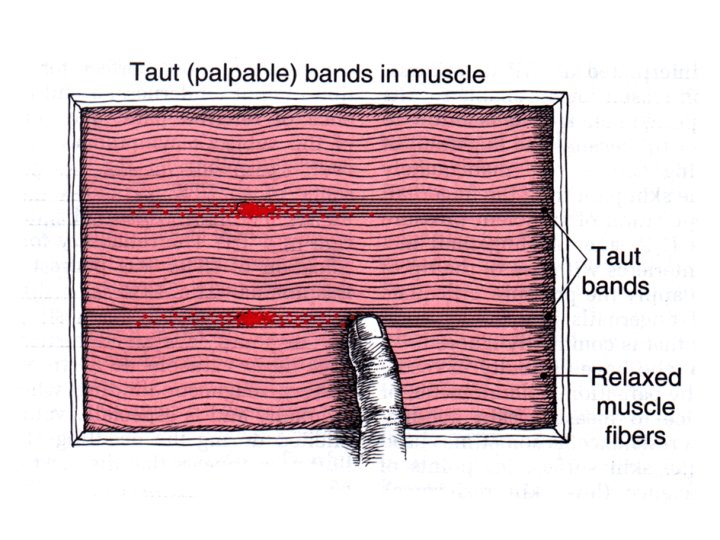
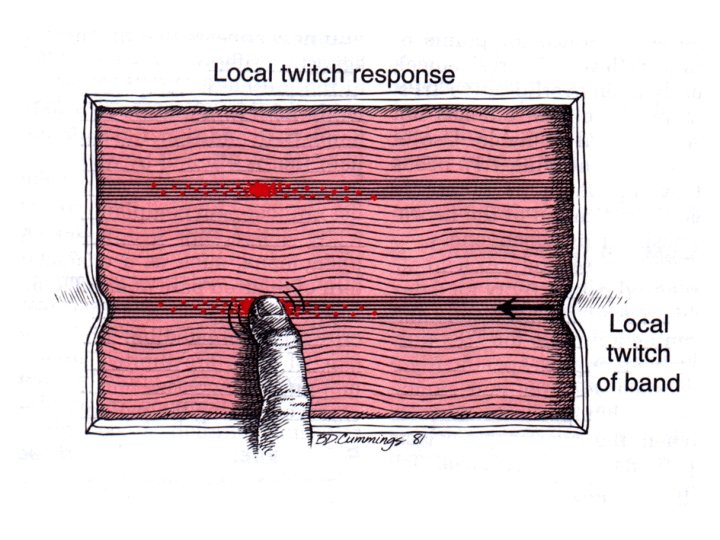
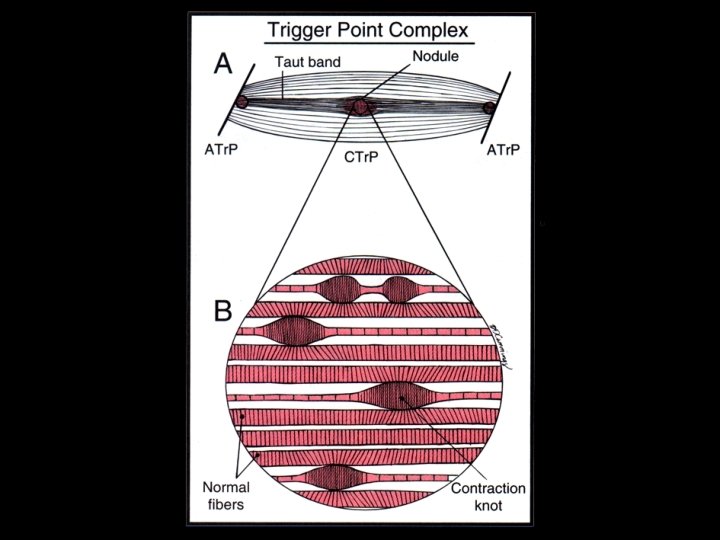
Physical Findings • • • Taut band tender nodule Recognition of familiar symptoms Referred sensory symptoms Local twitch response Limited range of movement
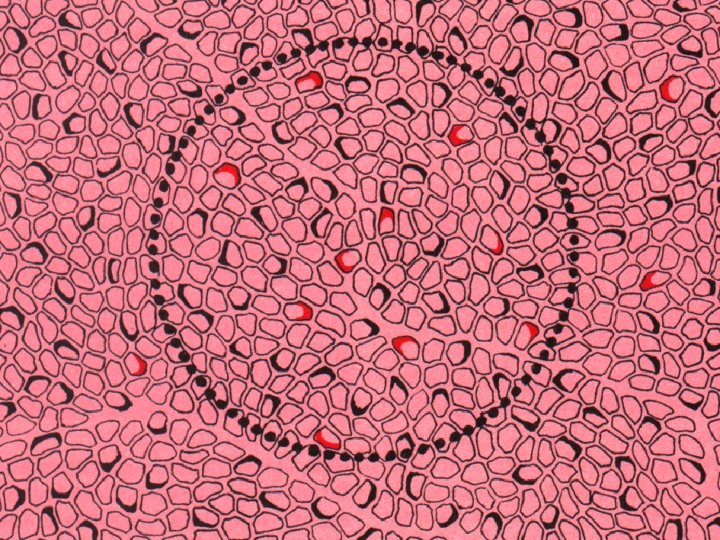
Central Vs Attachment Tr. Ps
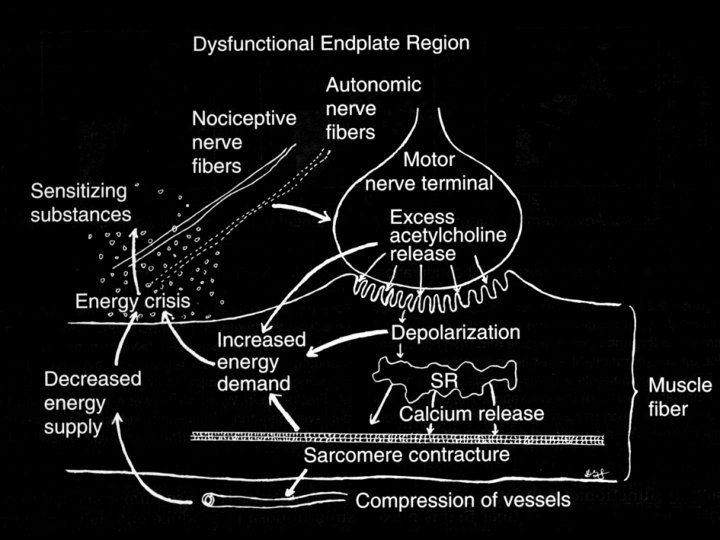
Energy Crisis Hypothesis Initial Sustained Calcium Release from SR Failed Reuptake of Calcium into SR Sustained Sarcomere Contracture Increased Metabolism Local Ischemia Energy Crisis
Prevalence of Trigger Point Pain
Pectoralis Major
MFP syndrome of Serratus Posterior Superior
Rectus Abdominis
Mc. Burney’s Point
Dysmenorrhea
Belch Button External Oblique Abdominis
Lateral Abdominis LLQ & Groin Pain Causes Diarrhea
Extensor Digitorum
Temporalis
Sternocleidomastoid
The 3 Directions of Referred Pain
Referred Pain • Referred at least partly in peripheral direction is most common (85% of patterns) • 48% referred only in direction of periphery • 20% both central & peripheral referral • 17% both local & peripheral referral • 10% only a local pattern • 5% refer only in a central direction
Criteria for Identifying a Tr. P Essential Criteria • Taut band palpable • Exquisite spot tenderness of a nodule in a taut band • Patient’s recognition of current pain by pressure on the trigger point • Painful limit to full stretch range of motion
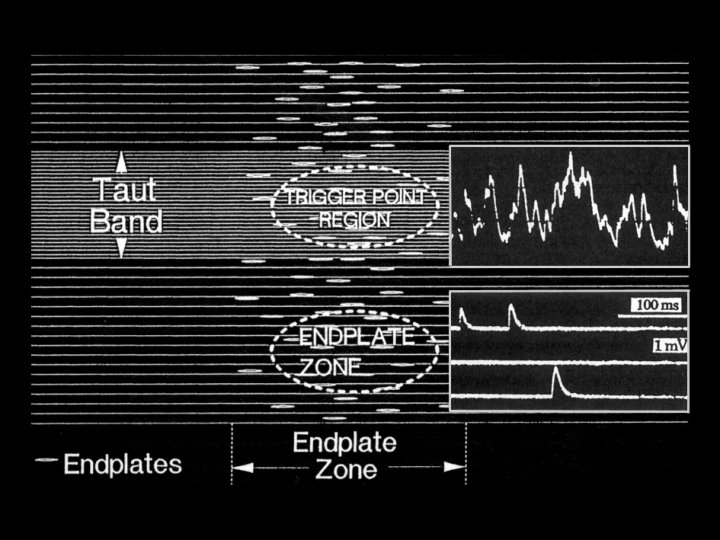
Criteria for Identifying a Tr. P Confirmatory Observations • Visual or tactile identification of local twitch response (LTR) • Imaging of a local twitch response induced by needle penetration of tender nodule • Pain or altered sensation (in the distribution expected) on compression of tender nodule • EMG demonstration of spontaneous electrical activity
Trigger Point Release • Spray and Stretch • Voluntary Contraction and Released Methods • Trigger Point Pressure Release • Deep Stroking Massage
Sequence of steps to use when stretching and spraying any muscle for myofascial trigger point
Neural pathway to explain effectiveness of spray and stretch
Trigger Point Release • Spray and Stretch • Voluntary Contraction and Released Methods • Trigger Point Pressure Release • Deep Stroking Massage
Accessory Techniques • • • Phased Respiration Directed Eye Movement Biofeedback Heat and Cold Iontophoresis and Phonophoresis
Modalities • Therapeutic Ultrasound • High Voltage (and High Frequency) Galvanic Stimulation
Pain Relief • Transcutaneous Electric Nerve Stimulation • Drug Therapy – Pain Killer – Muscle Relaxants – Sleep
Trouble-making Drugs • Caffeine – Small to moderate amounts of caffeine may help to minimize Tr. Ps – Excessive intake of caffeine ( > 2 or 3 cups/bottles/cans of coffee and/or cola) is likely to aggravate Tr. P activity • Alcohol reduces absorption of folic acid • Tobacco increases the need for vitamin C
Trigger Point Injection • Local anesthetic with or WITHOUT corticosteroid • Dry needling – Within 2 - 8 hours, 42% of lidocaine-injected patients and 100% of dry-needled patients developed local soreness • Botulinum toxin A
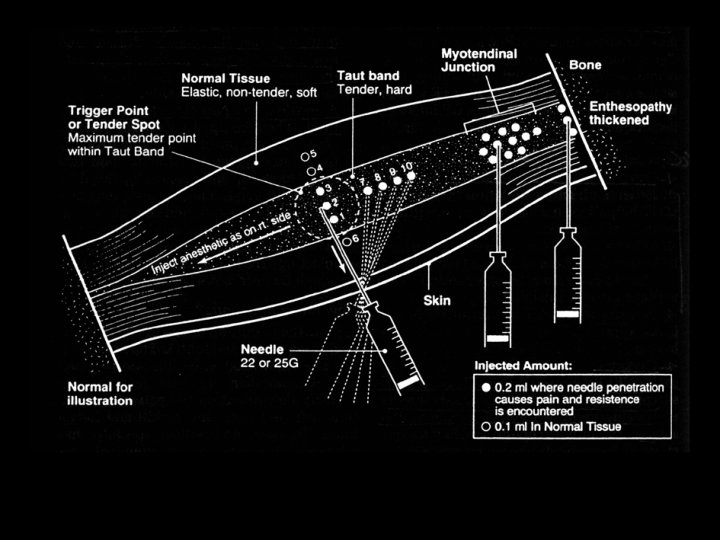
Flat palpation to localize and hold the trigger point for injection
Two approaches to the flat injection of a Tr. P
A 22 -gauge, 3. 8 -cm (1. 5 -in) needle is usually suitable for most superficial muscles. A 21 -gauge, 6. 4 -cm (2. 5 -in) needle is generally long enough to reach Tr. Ps in the deepest muscles.
Appropriate Activities • Strenuous activities should be avoided for at least 2 or 3 days if soreness develops • Use muscles in gentle, normal way through their full range of motion • Avoid placing muscles in fixed, shortened position for long time • Any activity that produces pain for more than a few seconds should be avoided
Perpetuating Factors • • • Mechanical stress Nutritional Inadequacies Metabolic Factors Psychological Factors Chronic infection Other factors (e. g. Allergic Rhinitis, Dysomnia, Nerve impingement)
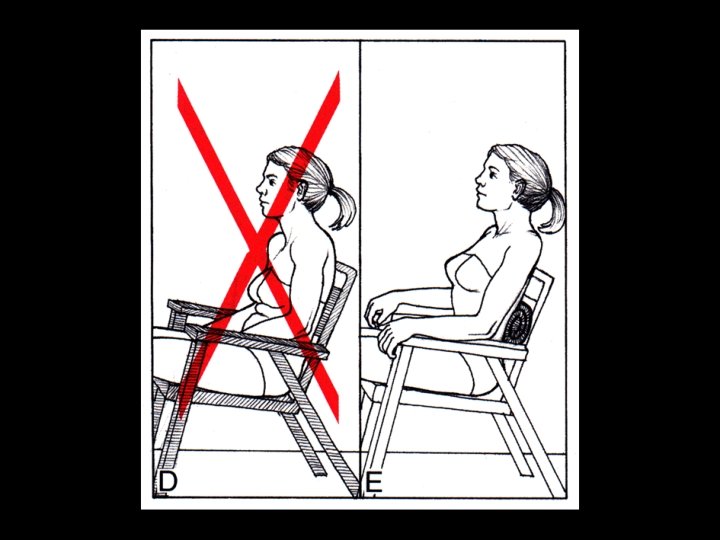
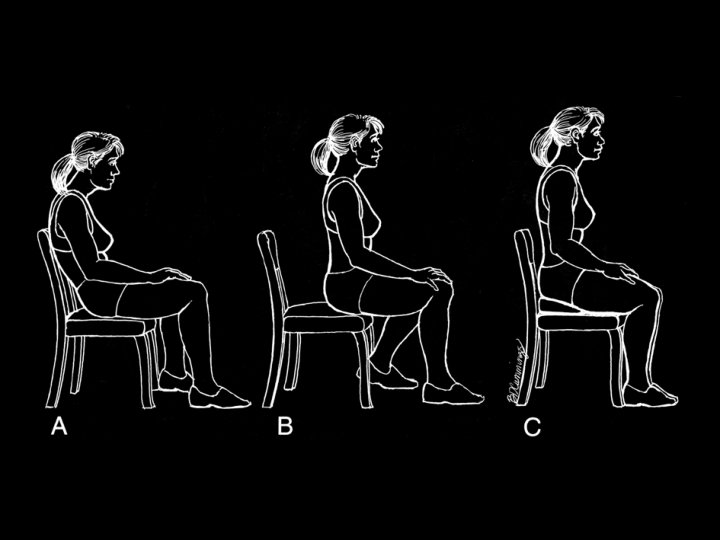
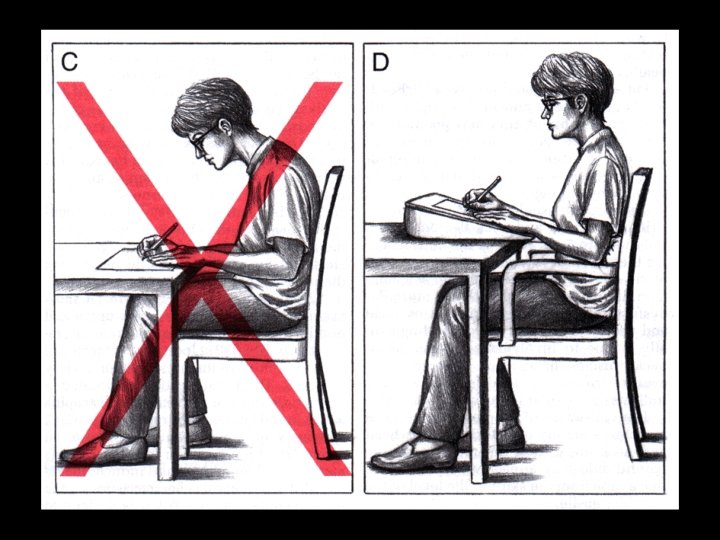
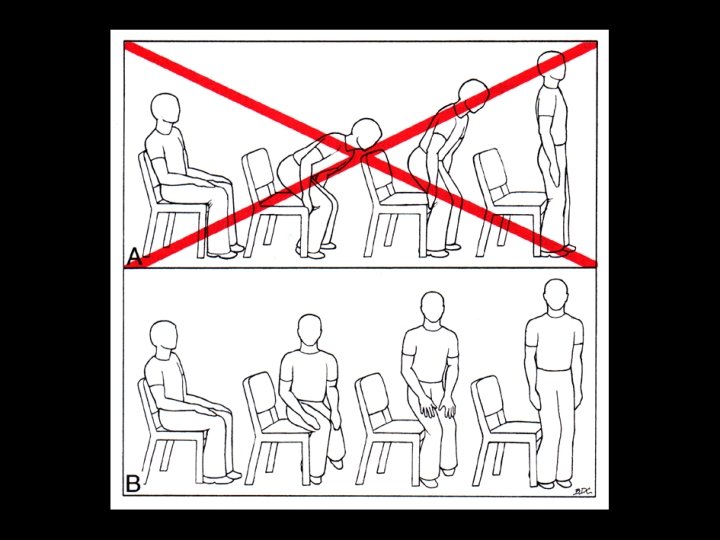
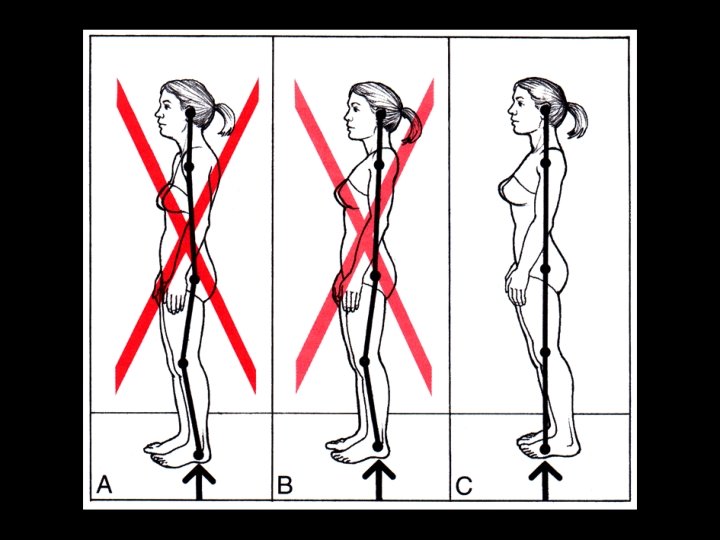
Which one is better ?
Which one is better ?
Which one is better ?
Structural Inadequacies • Lower Limb-length Inequality • Small Hemipelvis • Short Upper Arms
Lower Limb-Length Inequality
Small Hemipelvis
Small Hemipelvis
Short Upper Arms
Short Upper Arms
Conclusion • Myofascial trigger points (Tr. Ps) are extremely common and become a painful part of nearly everyone’s life at one time or another • Try to seek for Tr. P in any cases of pain and dysfunction