An Introduction to Diagnosis in Respiratory Medicine Steve


")



 tracings Volume FEV 1 Normal subject Asthmatic (after bronchodilator) Asthmatic")
 • Irreversible (COPD) •")
, so not much")












: Fibrotic (scarring) conditions • • Characteristics • Many are associated with")


















- Slides: 53
An Introduction to Diagnosis in Respiratory Medicine Steve Renshaw Professor of Respiratory Medicine
Objectives • Understanding: • the main categories of lung disease • how to refine the diagnosis by cause • how to approach diagnosis of a chronically and acutely breathless patient • how to differentiate asthma and COPD • How to structure investigations to understand respiratory disease
Main Disease Categories • Structures involved • Main disease types • Breathing tubes (Obstructive) • • Lung parenchyma (Restrictive) • • • Chest wall (Restrictive) • • Pulmonary circulation • Pleura Inflammatory Neoplastic Infective Vascular
Diagnostic Tests in Respiratory Medicine • Lung Function Testing • Bronchoscopy • Spirometry • Thoracoscopy • Lung Volumes • Oximetry • Transfer factor • Radiology • Plain X-ray • CT scanning • Ultrasound • Functional assessment of respiratory function • 6 minute walk • Incremental Shuttle walking test • Cardio-respiratory exercise testing
Spirometry • Fill lungs as much as possible • Blow the air out as fast as possible and • Keep on blowing out for as long as possible
Spirometry • Fill lungs as much as possible • Blow the air out as fast as possible and • Keep on blowing out for as long as possible
Typical spirometric (FEV 1) tracings Volume FEV 1 Normal subject Asthmatic (after bronchodilator) Asthmatic (before bronchodilator) 1 Each FEV curve represents the highest of three repeat measurements 1 2 3 4 Time (seconds) 5
Restrictive vs. Obstructive Respiratory Disease • Obstructive • Reversible (Asthma) • Irreversible (COPD) • Restrictive • Interstitial Lung disease Fibrosing Alveolitis Intrinsic Extrinsic Sarcoid • Chest wall disease Kyphoscoliosis
Obstructive Lung Disease • Takes a long time to exhale (wheeze), so not much breathed out at 1 second, but volumes not too bad • FEV 1 lower than FVC • FEV 1/FVC <80%
Actual Spirometry Traces 1
Common Obstructive Lung Diseases • Asthma • variable airflow obstruction • COPD (chronic obstructive pulmonary disease) =chronic bronchitis and emphysema • relatively fixed airflow obstruction • Bronchiectasis • dilated bronchi which pool secretions • characteristic feature is copious purulent sputum • may be a mixture of restrictive and obstructive disease
Diagnosis of airflow obstruction: demographics • Young: Asthma? CF? • Older smoker: COPD? Lung cancer? • Older non-smoker: ? asthma/fixed airflow obstruction
Pointers from the history • Asthma suggested by variability: • wheezing in response to: exertion fumes cold air • worse at night and early morning • history of childhood wheezing, presence of other atopic conditions • COPD suggested by insidious onset in a smoker • Lung cancer suggested by recent onset and progressive especially if >40 and a smoker
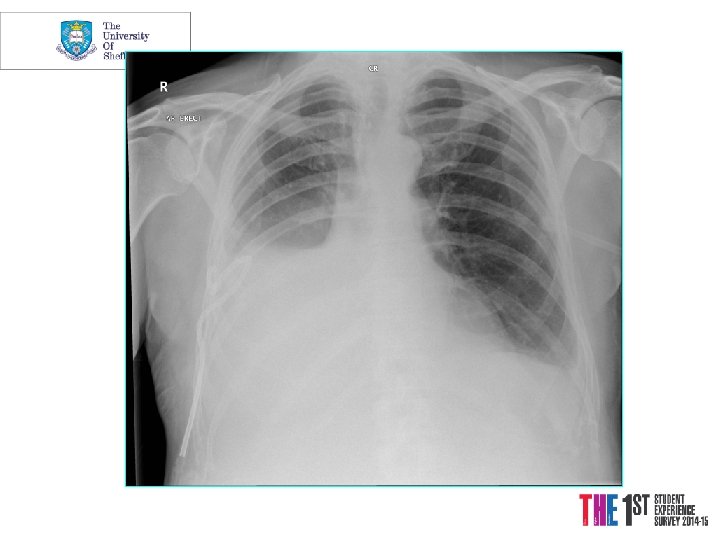
Case History 1 • 64 year man • Increasing SOB over 8 months • Dry Cough • Retired Lathe operator • Ex-smoker (10 pack years) • Bibasal crackles
Actual Spirometry Traces 2
Restrictive Lung Disease • Due to restriction, lung volumes are small and most of breath is out in first second • FVC proportionately lower • FEV 1/FVC >80%
Spirometry; lung volumes and subdivisions Maximal inspiratory level Lung Volumes Inspiratory reserve Inspiratory volume capacity (IRV) (IC) Vital capacity Total (VC) lung Tidal capacity volume (VT) Resting end-expiratory (TLC) Expiratory level reserve volume Functional (ERV) residual capacity Maximal expiratory level Residual (FRC)* volume *Not determined (RV)* by spirometry
Transfer Co-efficient 1 • Measure of ability of Oxygen to diffuse across the alveolar membrane • Inspired low dose carbon monoxide, 10 s breath hold at TLC • Gas transferred is measured
Transfer Co-efficient 2 • Low in: • Severe empysema • Fibrosing alveolitis • Anaemia • Etc. • High in: • Pulmonary haemorrhage
Functional assessment of respiratory function • 6 minute walk • Incremental Shuttle walking test • Cardio-respiratory exercise testing
Case History 1 • 64 year man • FEV 1/FVC 90%, Low TLCO • Fibrosis on CT, and VATS biopsy • Diagnosis: Idiopathic Pulmonary Fibrosis (IPF)
Lung Parenchyma (alveoli): Fibrotic (scarring) conditions • • Characteristics • Many are associated with finger clubbing • The lungs become stiff leading to them getting smaller • Gas exchange is usually impaired (hypoxia) • Often profound breathlessness on exertion Causes • Range of idiopathic conditions • Idiopathic Pulmonary Fibrosis (Cryptogenic fibrosing alveolitis =commonest) • Asbestosis • Sarcoidosis • Extrinsic allergic alveolitis (birds, mouldy hay etc) • Post-infective (esp T. B. ) • Radiation (radiotherapy)
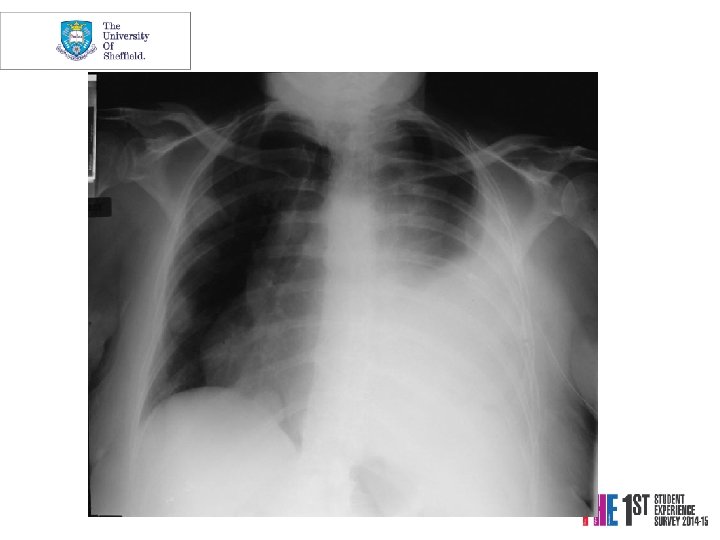
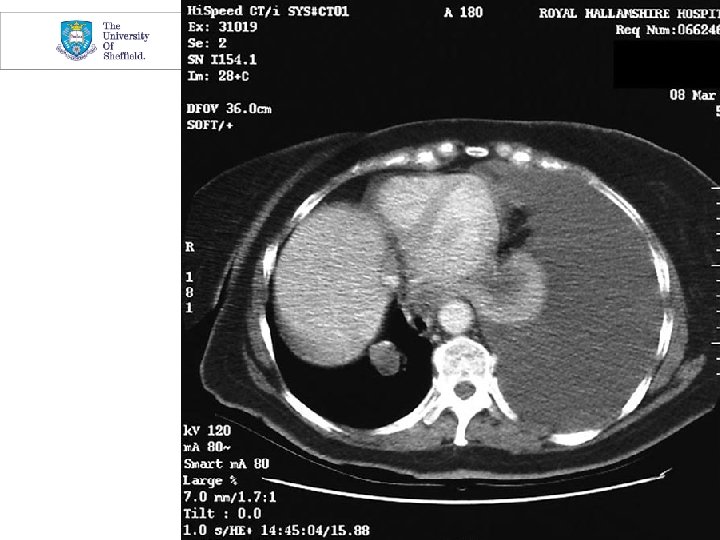
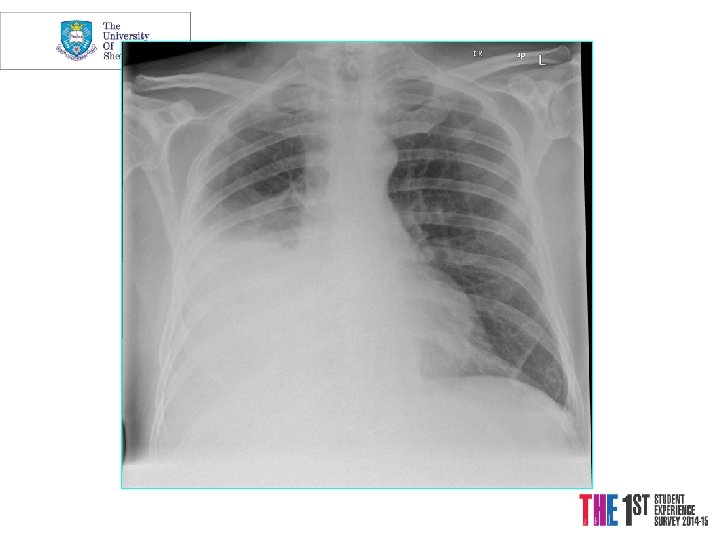
Case History 2 • 76 year old woman • c/o Haemoptysis and weight loss • Smoker of 104 pack years • Clubbed
Diagnostic investigations Plain chest radiology • Lobar collapse / consolidation • Lesion behind the heart • Abnormal hilum • Pleural cap • Peripheral coin lesion • Rib erosion • Central airway tumour • Pleural effusion
Diagnostic investigations Bronchoscopy • Samples • Major complications • washing • pneumonia • brushing • pneumothorax • mucosal biopsy • haemorrhage • transbronchial biopsy
Indications for Bronchoscopy 1 • Radiological • Lobar Collapse • Mass • Persistant consolidation • Haemoptysis • Cough, wheeze, stridor, dyspnoea
Indications for Bronchoscopy 2 • Transbronchial Biopsy for Interstitial dis. • Undiagnosed Infection • esp. in Immunocompromised • Suspected aspiration of foreign body • Therapeutic • Stent • Laser • Brachytherapy
Lung Cancer • Early symptoms include • change in cough • wheeze • haemoptysis (much more sinister if not associated with purulent sputum) • Later symptoms include • weight loss • lethargy
Pulmonary Vascular Disease • Pulmonary hypertension • Pulmonary embolism (P. E. , clots in the pulmonary arterial tree, usually arising from the deep veins of the legs)
3 presentations of PE • Minor • breathlessness/haemoptysis, pleuritic chest pain • “Classic” • Acute Massive • Circulatory collapse • Life-threatening emergency • Multiple/submassive • isolated dyspnea • Often missed
Causation • We not only need to determine the cause physiologically, but consider the aetiology, especially environmental/occupational: • e. g. estimated that about 10% of adult onset asthma may be occupational • asthma may be exacerbated by allergy to a pet • asbestos and other dust/ fume exposures may be causative
Diagnostic Pointers for the Chronically Breathless Patient Airflow obstruction is suggested by: • history of wheezing / bronchitis • wheezing and/or hyperinflation on examination • obstructive spirometry • hyperinflated chest X-ray
The Chronically Breathless Patient with no wheezing or airflow obstruction Is there restrictive lung disease? • On examination: - Crackles on auscultation? - Abnormal chest wall? • Restrictive spirometry? • Interstitial shadowing on chest X-ray? • Remember to distinguish from non-respiratory causes -next slide
Non-Respiratory Causes of Chronic Breathlessness • Heart disease • Anaemia • Deconditioning • Psychogenic
Respiratory causes of acute Breathlessness • Asthma • Pneumonia • Pulmonary embolism • Pneumothorax • Hyperventilation
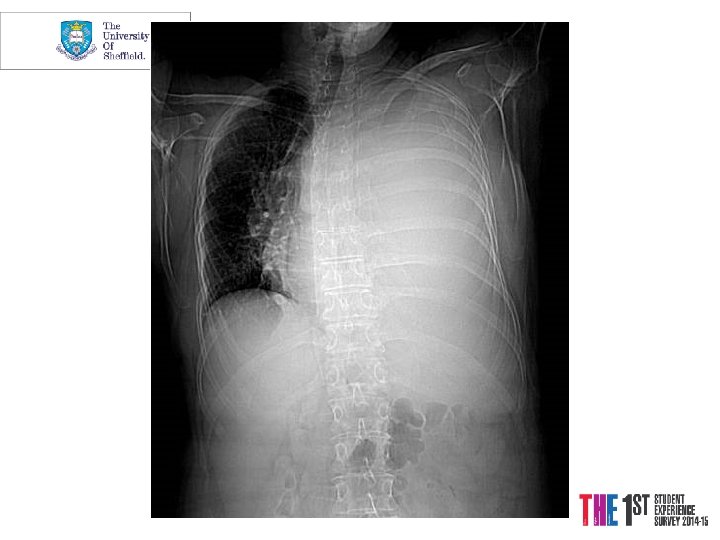
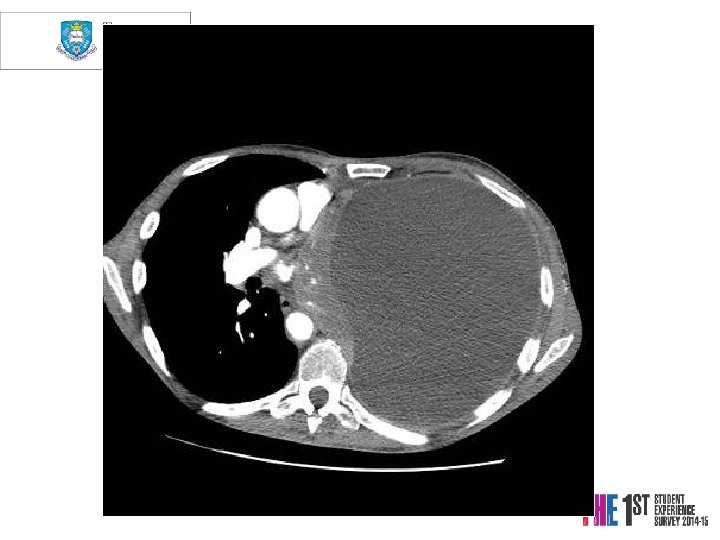
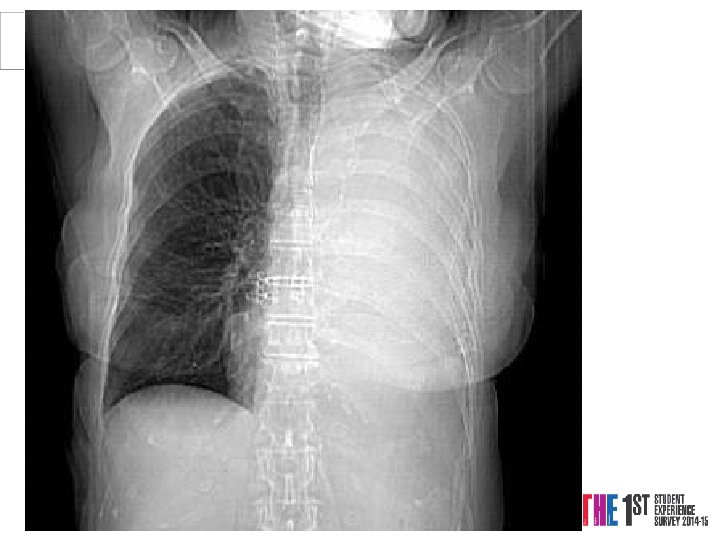
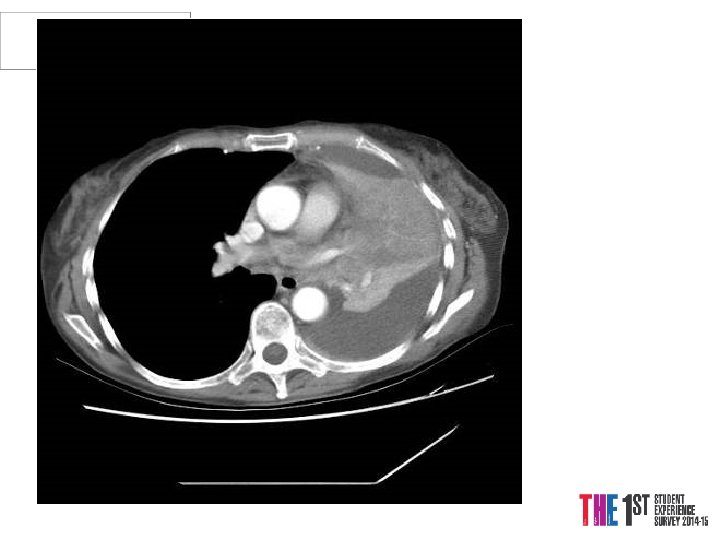
Case 3 Mrs. PD • 66 y. o referred from X-ray • 1/12 SOBOE, now SOB on dressing • Cough 2/52, dry • PMH Throat Cancer Rx Surgery and Radiotherapy 2004 -5, Ex-smoker • o/e L side of chest Dull PN, BS
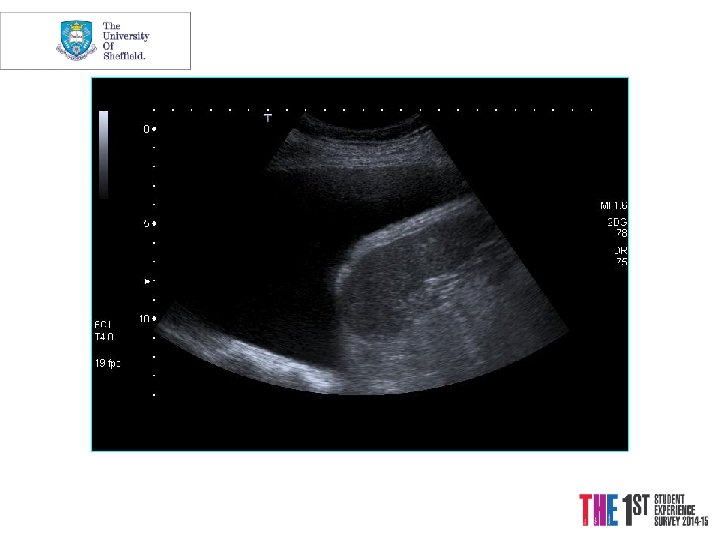
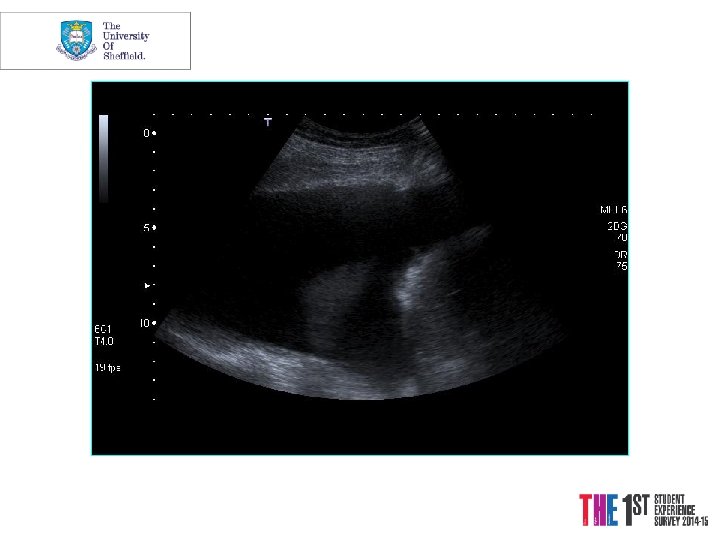
“Safe” triangle
“Safe” triangle
Conclusions • PFT’s allow differentiation between obstructive and restrictive lung diseases • Radiology is central to respiratory medicine • Bronchoscopy and Thoracoscopy allow sampling of otherwise inaccessible areas