An acute systemic allergic reaction Mast cells basophils



• An acute systemic allergic reaction - Mast cells & basophils - The response can be severe enough to cause death • Allergic or immunologic mechanism, allergic anaphylaxis Non-allergic anaphylaxis (formerly, as an anaphylactoid reaction) (WAO Nomenclature Review Committee JACI 2004)

Gell and Coombs Hypersensitivity Type I Immedicate hypersensitivity – Ig. E Type II Cytotoxic reactions – non-Ig. E – Transfusion reaction (Ig. G, Ig. M) Allergic Anaphylaxis Type III Immune complex reactions – non-Ig. E – IVIG, Dextran Non-allergic anaphylaxis (anaphylactoid reaction) – Radiocontrast media, ethylene oxide gas on dialysis tubing, aspirin, NSAID, opiates, exercise, cold, heat, idiopathic (Kemp SF and Lockey RF, J Allergy Clin Immunol 2002; 110: 341 -8)
 Ig. E mediated anaphylaxis")
Revised Nomenclature for anaphylaxis Allergic anaphylaxis Non-allergic anaphylaxis (previous anaphylactoid) Ig. E mediated anaphylaxis Non-Ig. E mediated anaphylaxis (Type I) (Type II & III) ( WAO Nomenclature Review Committee JACI 2004)
 호염기구 (Basophil)")
비만세포 (Basophil) 호염기구 (Basophil)

알레르겐 Ig. E Histamine, Tryptase
 Tryptase( -, β-) Chymases Carboxypeptidase β-hexosaminidase")
Mast cell • Preformed Histamine (2 -3 pg/cell) Tryptase( -, β-) Chymases Carboxypeptidase β-hexosaminidase β-glucuronidase Arylsulfatase Superoxide dismutase Heparin Chondroitin sulfate • Newly formed PGD 2, PGF 2, TXA 2 LTB 4 LTC 4/LTD 4, LTE 4 PAF Basophil • Preformed Histamine (1 pg/basophil) Neutrophil chemotactic factor N-p-Tosyl-L-arginine methyl ester hydrochloride (TAME) esterase Kallikrein Proteoglycans Unidentified protease Lysophospholipase MBP Tryptase ; less 1% than MC • Newly formed LTC 4, PAF 1 -acyl-PAF Oxygen radicals, superoxide

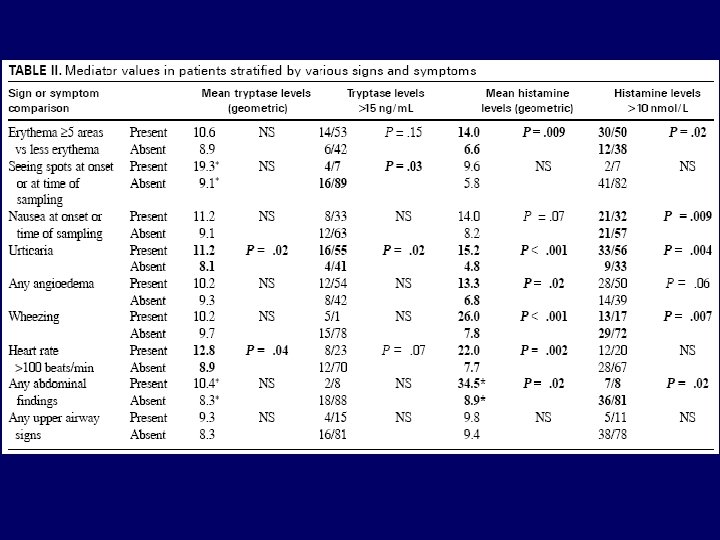
J Allergy Clin Immunol 2000; 106: 65 -71

- 97 adult emergency department patients were prospectively studied by using a questionnaire, physical examination, and serum-plasma sampling. - Plasma histamine and serum total and βtryptase levels were determined.

Figure. Plot of histamine versus total tryptase levels (only for patients who had both determinations).

Cell membrane phospholipid Phospholipase A 2 Arachidonic acid 5 -lipoxygenase Leukotriene A 4 Leukotriene B 4 Cyclooxygenase Prostaglandin G 2 Leukotriene C 4 Prostaglandin H 2 Leukotriene D 4 Leukotriene E 4 Prostacycline. Thromboxane APG D 2 E 2 F 2 a 2

LTB 4 AA BLT receptor LTA 4 Cys. LT 2 receptor 5 -LO inhibitors LTC 4 LTD 4 LTE 4 Leukocyte activation Cytokine secretion Ig. E synthesis Nuclear transcription Vascular effects Bronchospasm Plasma exudation Cys. LT 1 receptor Vascular effects Mucus secretion Eosinophil recruitment Smooth m. proliferation Cys. LT 1 receptor Cardiodepression antagonists
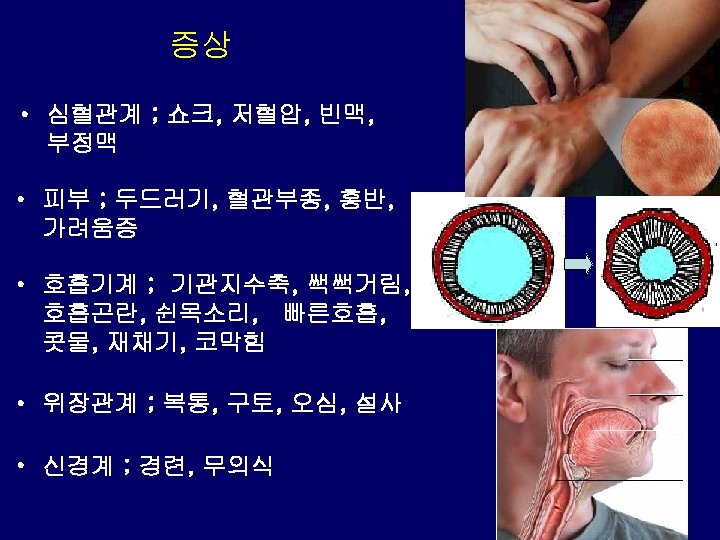

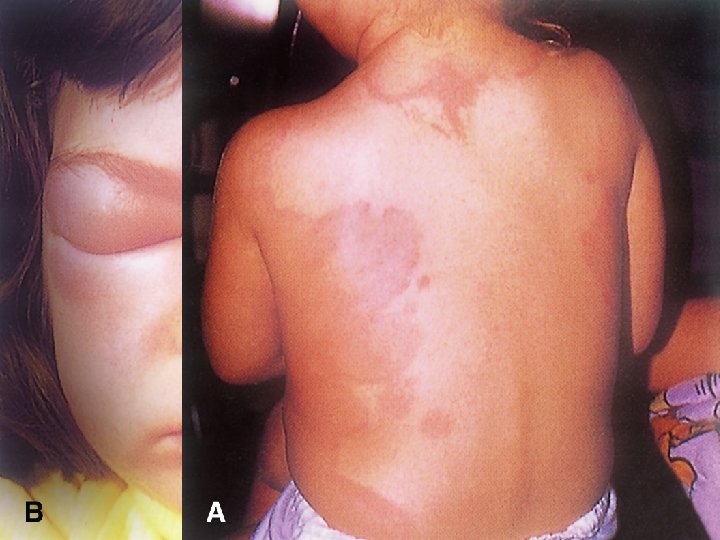
Frequency of occurrence of signs and symptoms of anaphylaxis Cutaneous 90% Urticaria and angioedema 85 -90 Flushing 45 -55 Pruritus without rash 2 -5 Respiratory 40%-60% Dyspnea, wheeze 45 -50 Upper airway angioedema 50 -60 Rhinitis 15 -20 Dizziness, syncope, hypotension 30%-35% Abdominal Nausea, vomiting, diarrhea, cramping pain 25%-30% Miscellaneous Headache 5 -8 Substernal pain 4 -6 Seizure 1 -2

Biphasic reactions

 Infants (1 -12 mo)")
When is it hypotension? Age Term neonates (0 -28 d) Infants (1 -12 mo) Children (>1 y to 10 y) Beyond 10 y Systolic blood pressure (mm Hg) 60 70 70 + (2 x age in yr. ) 90

Laboratory tests to be considered in the differential diagnosis of anaphylaxis - Plasma histamine levels begin to increase within 510 min and remain increased only for 30 -60 min. They are of little help if the patient is seen as long as an hour or more after the onset of the event. - 24 -h Urinary histamine metabolite (methyl histamine) Urinary histamine and its metabolites are increased for a longer period of time, up to 24 hours.

Laboratory tests to be considered in the differential diagnosis of anaphylaxis - Serum tryptase levels peak 60 -90 min after the onset of anaphylaxis and persist to 6 hours. Ideally, the measurement should be obtained between 1 and 2 hours after the initiation of symptoms. -subunit ; constitutional form β-subunit ; secretory form ( +β)/β ratio, 20 이상 ; systemic mastocytosis 10미만 ; anaphylaxis

Laboratory tests to be considered in the differential diagnosis of anaphylaxis - Serum tryptase postmortem increase of serum tryptase concentrations is not a specific finding and therefore cannot be considered diagnostic of an anaphylactic death. The presence of an increased postmortem tryptase level cannot be considered pathognomonic for a death caused by anaphylaxis or an anaphylactoid event

Laboratory tests - Plasma-free metanephrine To rule out a paradoxical response to a pheochromocytoma. - Urinary vanillylmandelic acid Also useful in ruling out a paradoxical response to a pheochromocytoma. - Serum serotonin To rule out carcinoid syndrome. - Urinary 5 -hydroxyindoleacetic acid Also to rule out carcinoid syndrome. - Serum vasointestinal hormonal polypeptide panel, including pancreastatin, pancreatic hormone, vasointestinal polypeptide (VIP), and substance P Useful to rule out the presence of a vasoactive polypeptide secreting astrointestinal tumor or a medullary carcinoma of the thyroid, which also can secrete vasoactive peptides.
 reaction")
감별진단 • • urticaria-angioedema hereditary angioedema, asthma. vasodepressor (vasovagal) reaction
- Slides: 34