AMNIOTIC FLUID EMBOLISM DR NIDHI PATEL ASSISTANT PROFESSOR

AMNIOTIC FLUID EMBOLISM DR. NIDHI PATEL ASSISTANT PROFESSOR DR. AJESH DESAI HEAD OF DEPARTMENT & PROFESSOR, OBSTETRIC & GYNECOLOGY DEPARTMENT GMERS , SOLA CIVIL HOSPITAL, GUJARAT.

Definition AFE is a condition in which amniotic fluid and fetal debris enter the systemic maternal circulation, producing an anaphylactic reaction causing sudden cardiovascular collapse, altered mental status and DIC.
 A breech in the physical")
PATHOGENESIS It requires two things to produce AFE 1) A breech in the physical barriers between maternal and fetal environment, mainly at the level of the endocervical veins, uterine trauma sites, and the placental attachment site. 2) A pressure gradient that favors the entry of amniotic fluid from the uterus into the maternal circulation must be present.

TIMING 70% of Amniotic embolism may occur during labor; 19% during caesarean section; and 11%post delivery. 7 AFE has also been reported during firsttrimester surgical termination of pregnancy, second trimester termination, abdominal trauma and amniocentesis. 12

Incidence The incidence is rare. Approximately 1 in 15, 000 deliveries. 3 Table 1 mentions the incidence of AFE in various studies. Table 1: Incidence of AFE & Case fatality rates in published series Author Year published Incidence (per 100000 maternities) 1. 9 -6. 1 Case fatality rate (%) Knight 10 2012 Knight 11 2010 2. 0 20 Abenhaim 1 2008 7. 7 21. 6 Tuffnell 18 2005 Not reported 29. 5 Gilbert 8 1999 4. 8 26. 4 Clark 6 1996 Not reported 61 Burrows 4 1995 3. 4 22 Morgan 13 1979 Not reported 86 11 -43

Maternal neonatal Morbidity / Mortality and morbidity are high. Accounts for 14% of maternal deaths in developed countries. The second leading cause of maternal deaths in developed countries. Maternal mortality rate has declined from an initial rate of about 80% to a current level of 22% with improved recognition and immediate treatment. 3 Table 2: Survival Rates The maternal fatality rate is reported as 35 %16, within the range of that reported in national registries in the United Kingdom and the United States, respectively 37 % and 61 %. The United Kingdom registry reported neurological impairment in 7 % ofsurvivors. 5 Neonatal survival was 79 % in the US registry and 78 % in the UK registry. Year Survival rates (%) Reason 1979 14 2005 30 Survival rates improved due to improved resuscitation techniques * RCOG 201115 2010 80

RISK FACTORS No definite risk factors have been established and AFE is such a rare event that no risk factor is likely to be of prognostic value. Risk factors are used for retrospective analysis. Risk approach should not be used for altering the clinical management of individual women as base line risk remains low. 2 However following risk factors have been identified and mentioned in literature. 1) Advanced Maternal Age 2) Placenta – previa 3) Placental abruption 4) operative delivery 5) Induction of labour 6) Polyhydramnios 7) Caesarian delivery 8) Uterine rupture 9) PIH 10) cervical laceration

Protective factors: - Maternal age <20 - Dystocia

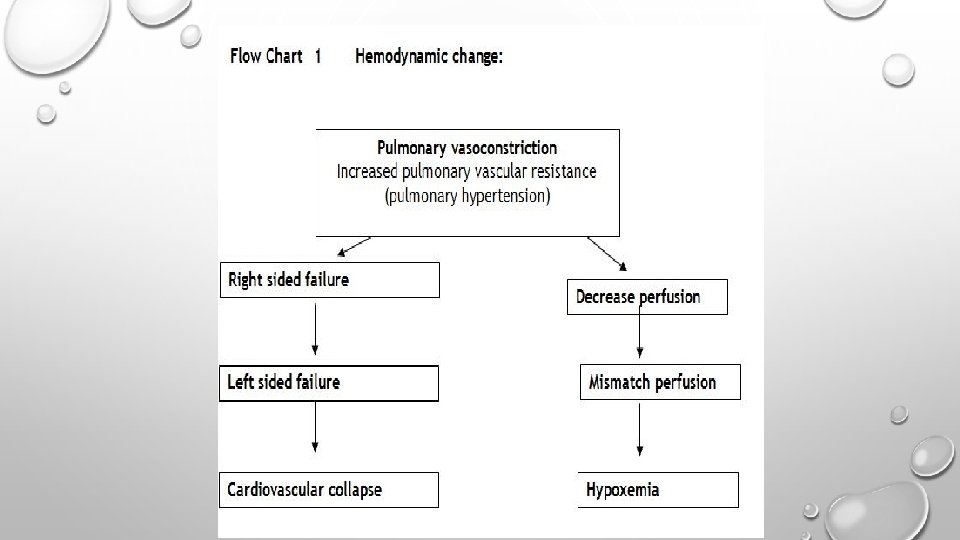
Response The body responds in two phases: • Pulmonary vasospasm causing respiratory and cardiovascular collapse. • The development of coagulopathy (DIC) and hemorrhage.

Clinical presentation • The pregnant women who develop AFE present in any of the phases mentioned below based on place where she has delivered institution or home. Referral cases will present in phase 1 or phase 2 based on severity of AFE. • Not all AFE are rapidly progressive and early diagnosis and supportive treatment may result in better outcomes. • First Phase: The patient experiences acute shortness of breath and hypotension. This rapidly progresses to cardiac failure leading to a reduction of perfusion to the heart and lungs. This may be preceded by “Premonitory symptoms “such as shivering, coughing, restlessness, numbness, agitation, tingling, vomiting and an unpleasant taste in the mouth. Not long after this stage the patient will lose consciousness due to circulatory collapse. More than 80 % of women with AFE experience cardio-respiratory arrest within the first few minutes. 14

Diagnosis • Diagnosis is difficult and may be a matter of exclusion. • Diagnosis is based on suspicion when patient presents with presentation mentioned above. • Currently there are no test available for diagnosis in survivors. Usually autopsy reveals presence of fetal material in pulmonary circulation. Sensitivity of this findings are low as these is also observed in normal women.
 Hypotension")
Table 2 Clinical presentations in AFE 6 Signs or symptoms Frequency ( %) Hypotension 100 Fetal distress 100 Pulmonary edema or ARDS 93 Cardiopulmonary arrest 87 Cyanosis 87 Coagulopathy 83 Dyspnea 49 Seizure 48 Uterine atony 23 Bronchospasm 15 Transient hypertension 11 Cough 7 Headache 7 Chest pain 2 AFE should be suspected in a woman experiencing 1 or more of the following findings during pregnancy, labor and delivery, or up to 48 hours postpartum: Hypotension and/or cardiac arrest , DIC, Coma , Seizures.

TESTS When AFE is suspected following investigation should be advised. Laboratory CBC coagulation profile ECG Tachycardia oxygen saturation ST and T wave abnormality arterial blood gases cardiac arrhythmias or asystole. cardiac enzymes electrolytes Pulse oxymetry Chest X-ray Echocardiography for diffuse bilateral May reveal severe heterogeneous and pulmonary hypertension homogeneous areas of increased opacity acute right ventricular failure with a leftward deviation of the interatrial & interventricular septum obliterating left ventricle cavity

Differential diagnosis • Pulmonary thrombo-embolism • Air embolism • Cardiac arrhythmia • Anesthetic complications (total spinal/epidural) • Peripartum cardiomyopathy • Aspiration of gastric contents • Postpartum hemorrhage

Table 3 Amniotic fluid embolism VS Pulmonary embolism 17 Clinical features of AFE compared to pulmonary embolism AFE PE Timing of onset Most likely to occur during delivery Any time Early symptoms Dyspnoea , restlessness, panic , feeling cold , paresthesia , pain less likely Dyspnoea , cough , haemoptysis Collapse Highly likely May occur DIC Highly likely Absent ECG Non specific CXR Pulmonary edema , ARDS , Right atrial enlargement , prominent pulmonary arc Segmental collapse , raised hemidiaphram , unilateral plueral effusion ABG Non specific CTPA Negative Positive

Complications Complication following the diagnosis of an amniotic fluid embolism includes: • Disseminated intravascular coagulation • Multi organ failure • Death

Recurrence of AFE has not been reported in the literature.
 Aim: Rapid Correction of hypoxia, hypovolaemia, coagulopathy for")
Management of Amniotic Fluid Embolism (AFE) Aim: Rapid Correction of hypoxia, hypovolaemia, coagulopathy for prevention of multiple organ failure. In severe cases, transfer of the patient to HDU may be necessary.

Steps for Management of AFE 1 Lie the patient in the left lateral position 2 Maintain Oxygen saturation at 90% or higher by administering oxygen in adequate concentrations by face mask, bag-valve mask, or endotracheal intubation. 3 Insert two size 16 intravenous cannula. Treatment of hypotension: Optimization of preload, with rapid volume infusion of isotonic crystalloid solutions. Fluid therapy should be based on pulmonary artery catheter or transesophageal echocardiography monitoing. Monitor

6 Monitor vital signs temperature, blood pressure, pulse, respirations, and oxygen saturation levels and record the observations every 15 minutes initially. 7 The obstetric registrar/ consultant on call should request an urgent ECG and monitor arterial blood gases frequently. Request chest x ray and a ventilation perfusion scan (VQ) scan if facilities are available. 8 Cardiac arrest: Cardiopulmonary resuscitation should immediately. Uterine evacuation after unsuccessful resuscitation may be therapeutic for the mother, because the weight of the gravid uterus on the inferior vena cava impedes blood return to the heart and decreases systemic blood pressure. 9 Treatment of refractory hypotension: Inotropes, such as dobutamine, dopamine and milrinone, can be added, because B-adrenergic effects improve myocardial contractility in addition to the a-adrenergic be initiated

10. Maintain the vital parameters as mentioned in table 4 Table 4: Maintenance of vitals parameters during management Essential Parameters Minimum value to be maintain O 2 Saturation > 90 % Blood Pressure > 90 mm Hg PO 2 At least 60 mm Hg Urine Output >25 ml / hour

11 Management of coagulopathy and bleeding : Discuss with consultant hematologist on call for first line treatment for correcting the coagulopathy and potential severe hemorrhage associated with AFE. Packed red blood cells: To maintain oxygen delivery to the tissues Fresh frozen plasma Platelets Cryoprecipitate: Particularly useful to replenish clotting factors in lieu of FFP in volume-restricted patients. It contains fibironectin which could facilitate the removal of cellular and particulate matter from the blood. Recombinant activated factor VIIa: For severe DIC, resistant to conventional blood product replacement Use of heparin to treat consumptive coagulopathy and corticosteroids to induce immunosuppression is very controversial and therefore should not be given.

12 Management of postpartum hemorrhage: Look for the usual causes of PPH such as atony, retained product of conception, or cervical or uterine lacerations. If bleeding is profuse and pharmacological intervention is unsuccessful, hysterectomy may be necessary. Consider mechanical and / or surgical techniques to control uterine haemorrhage (Bakri balloon, B-Lynch suture). Bilateral uterine artery embolisation has been successful in controlling blood loss in 2 reported cases. 9 13 Surgical Intervention Perform perimortem caesarean section in women who have suffered a cardiac arrest and who are unresponsive to resuscitation. It may be appropriate to perform a caesarean section for other maternal or fetal indications before cardiac arrest.

14 Other less common therapeutic approaches: • Aprotinin and serine proteinase inhibitor FOY for DIC • Uterine artery embolization for severe PPH • Cardiopulmonary bypass • Pulmonary artery thromboembolectomy • Thrombolysis with tissue-plasminogen activator • Continuous hemodiafiltration • Arteriovenous hemofiltration • Exchange transfusion • ECMO • Intraaortic balloon counterpulsation • Inhaled nitric oxide

15 Fetal Considerations and Management: In most instances, AFE does not occur until after delivery. When AFE occurs before or during delivery, the fetus is in grave danger from the onset because of the maternal cardiopulmonary crisis. Following steps should be taken - Continuous monitoring should remain in progress. - Ensure that the patient is positioned in the left lateral position. - As soon as the mother’s condition is stabilized, delivery of the viable infant should be expedited. Alert the pediatric team if birth is imminent. If resuscitation of the mother is futile, an immediate Grade 1 emergency caesarean delivery may be necessary to save the infant. The sooner the fetus is delivered after maternal cardiopulmonary arrest, the more favorable is the fetal outcome.

• References: 1 Abenhaim HA, Azoulay L, Kramer MS, Leduc L. Incidence and risk factors of amniotic fluid embolisms: a population-based study on 3 million births in the United States. Am J Obstet Gynecol. 2008 Jul; 199(1): 49 e 1 - 8. 2 Abenhaim HA, Azoulay L, Kramer MS, Leduc L. Incidence and risk factors of amniotic fluid embolisms: a population-based study on 3 million births in the United States. Am J Obstet Gynecol. 2008 Jul; 199(1): 49 e 1 - 8. 3 acog May 28 2014 draft guideline 4 Burrows A, Khoo SK. The amniotic fluid embolism syndrome: 10 years’experience at a major teaching hospital. Aust N Z J Obstet Gynaecol. 1995 Aug; 35(3): 245 -50. 5 Centre for Maternal and Child Enquiries (CMACE). Saving Mothers’ Lives: reviewing maternal deaths to make motherhood safer: 2006– 08. The Eighth Report on Confidential Enquiries into Maternal Deaths in the United Kingdom. BJOG 2011; 118(Suppl. 1): 1– 203. Available from URL: http: //onlinelibrary. wiley. com/doi/10. 1111/j. 1471 - 0528. 2010. 02847. x/pdf 6 Clark SL, Hankins GD, Dudley DA, Dildy GA, Porter TF. Amniotic fluid embolism: analysis of the national registry. Am J Obstet Gynecol. 1995 Apr; 172(4 Pt 1): 1158 -67. 7 Clark SL, Hankins GDV, Dudley DA, Dildy GA, Flint Porter T. Amniotic fluid embolism: analysis of the

8 Gilbert WM, Danielsen B. Amniotic fluid embolism: decreased mortality in a population-based study. Obstet Gynecol. 1999 Jun; 93(6): 973 -7. 9 Goldszmidt E, Davies S. Two cases of hemorrhage secondary to amniotic fluid embolus managed with uterine artery embolization. Can J Anaesth 2003; 50(9): 917 -21. 10 Knight M, Berg C, Brocklehurst P, Kramer M, Lewis G, Oats J, etal. Amniotic fluid embolism incidence, risk factors and outcomes: a review and recommendations. BMC Pregnancy Childbirth. 2012; 12: 7. 11 Knight M, Tuffnell D, Brocklehurst P, Spark P, Kurinczuk JJ. Incidence and amniotic-fluid embolism. Obstet Gynecol. 201 May; 115(5): 910 -7. 12 Moore LE, Smith CV. Amniotic Fluid Embolism Treatment and Management. Emedicine Medscape [serial online] 2009 Dec [cited 2011 May 17]. 13 Morgan M. Amniotic fluid embolism. Anaesthesia. 1979 14 Perozzi KJ, Englert NC. Amniotic fluid embolism: An obstetric emergency. 2004; 24: 54 15 RCOG 2011 guidelines 16 Roberts CL, Algert CS, Knight M, Morris JM. Amniotic fluid embolism in population-based cohort. BJOG 2010; 117: 1417 -21. risk factors for Crit Care. Nurse an Australian

ABBREVIATION • AFE - AMNIOTIC FLUID EMBOLISM • PE - PULMONARY EMBOLISM • DIC - DISSEMINATED INTRAVASCULAR COAGULATION • CXR - CHEST XRAY • CBC - COMPLETE BLOOD COUNT • HDU- HIGH DEPENDENCY UNIT • ABG - ARTERIAL BLOOD GAS ANALYSIS • CTPA - CARDIO THORACIC PULMONARY ANGIOGRAPHY • ARDS - ADULT RESPIRATORY DISTRESS SYNDROME • FFP - FRESH FROZEN PLASMA

THANK YOU
- Slides: 30