AMERICAS OPIOID CRISIS Deidre Bell St Dominics Hospital

AMERICAS OPIOID CRISIS Deidre Bell St Dominics Hospital Gordon Lyons, MD St Dominics Hospital Geralyn Datz, Ph. D Southern Behavioral Medicine Associates, PLLC

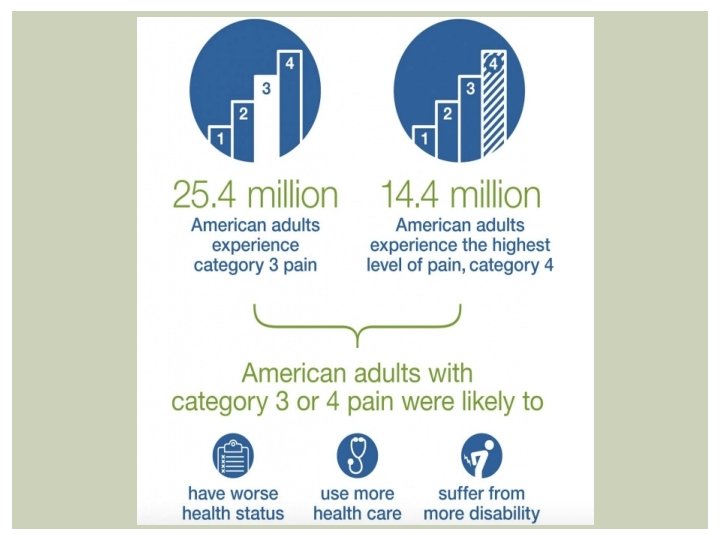
PUBLIC HEALTH IMPACT OF CHRONIC PAIN Chronic pain affects 116 million Americans (one-third of the population) and costs $550 billion to $635 billion a year in medical bills and lost productivity. The most common types people reported in a survey: • Low back pain – 28% • Knee pain – 20% • Severe headache or migraine - 16% • Neck pain – 15% • Shoulder pain – 9% • Finger pain – 8% • Hip pain – 7% Source: Institute of Medicine; 2011 survey of U. S. adults reporting that they had pain in the past three months

Estimates of Pain Prevalence and Severity in Adults: U. S. 2012. (Nahin RL/Journal of Pain 2015/NHIS/NCCIH/NIH)

ON THE OTHER HAND…. . Every 10 seconds someone dies from opiate overdose Overdose by opiates (heroin-1 st, medication-2 nd) is the #1 cause of death under age 50 Opioids extend the duration of temporary disability benefits (WCRI) Opioid use is dropping dramatically in some states. But few alternatives have been proposed to address pain in return. PEOPLE magazine did a recent story on this overdose epidemic from heroin and prescription drugs

FACES OF AMERICANS WHO HAVE DIED FROM OVERDOSE

TIME MAGAZINE

SOURCES OF DIVERTED PAIN MEDICATION
")
MS OPIOID & HEROIN TASK FORCE (2017)

MS TASK FORCE Last year in Mississippi, there were enough opioids dispensed legally for each person, from infants to elders— 2. 9 million people—to have 70 pills each, " Dowdy said. "That is in excess of 201 million dosage units dispense legally in Mississippi. ” Rankin County, alone in 2016, had a population of 150, 228 and 159, 733 opioid prescriptions filled. "There were 9, 500 more prescriptions filled than there were people, " Dowdy said.
 of all")
MS TASK FORCE Heroin was involved in 24. 0 percent (35 cases) of all opioid-related overdose death in 2015, data from the Mississippi Department of Health show. Dowdy says the amount of heroin in Mississippi has increased significantly. "Ten years ago, we may have seen one or two instances, " Dowdy said. "We had more than 275 separate seizures of heroin in Mississippi in 2016. The fact of the matter is, what we are seeing in Mississippi is the trend we have seen in every other state that has been battling this epidemic. There is substantial over-prescribing, people get addicted, they may not be able to afford it, and then all of the sudden they realize heroin is a lot cheaper. "

OPIOID EPIDEMIC

CDC REPORT: JULY 2014 PRESCRIPTION PAINKILLERS WRITTEN AT HIGH RATES

DO WE HAVE 2 EPIDEMICS? Heroin/Opioid/Prescription Drug Epidemic Chronic Pain Epidemic

OVERVIEW We have a systems based problem There is no one party to blame § Doctors / Healthcare Providers § Insurers § Adjusters and Case Managers § Patients § Pharmaceutical Companies § Media

OPIOIDS ARE THE TREATMENTS THAT ARE NEVER DISCONTINUED Medications should never have become a cornerstone of chronic pain treatment. Why? § Tolerance § Side effects § Opioid induced hyperalgesia § Drug Interactions, Toxicity § Passivity of patient § Symptom based § Brain and Body adapt to Rx as new normal

OPIOIDS ARE THE TREATMENTS THAT ARE NEVER DISCONTINUED Doses may go up over time Rotations are suggested Functional changes are often not seen as part of the treatment plan Detox is rarely, if ever, suggested for “normal” pain patients


WORKPLACE INSURERS SPEND AN ESTIMATED $1. 4 BILLION ANNUALLY ON PAINKILLERS, OR OPIOIDS If used too early in treatment, too frequently or for too long opioids can drive up associated disability payouts and medical expenses by delaying an employee’s return to work. Workers who received high doses of opioid painkillers to treat injuries like back strain stayed out of work THREE times longer than those with similar injuries who took lower dose, (2008, California Workers Compensation Institute).

THE RX FIX When medical care and disability payments are combined, the cost of a workplace injury is NINE times higher when a strong narcotic like Oxy. Contin is used than when a narcotic is not used (2010 analysis by Accident Fund Holdings, an insurer that operates in 18 states)

RISK FACTORS FOR OPIOID ABUSE Personal hx of substance abuse Family hx of substance abuse Young age Hx of childhood sexual abuse Mental illness Psychological stress Social patterns of drug abuse Polysubstance abuse Osler, W. (2007) Risk factors for opioid abuse. In: Webster, L. R. & Dove, B. (Eds. ) Avoiding Opioid Abuse While Managing Pain. New York: Sunrise River Press pp. 69 -70.
 A psychological evaluation is strongly")
GUIDELINES FOR THE CHRONIC USE OF OPIOIDS (ACOEM, 2011) A psychological evaluation is strongly recommended in select patients who have a relatively low threshold for chronic opioid use Considerations include: § any dissonance between subjective/objective findings § the need to add or escalate opioid usage § any psychological disorder or prior history of psychological disorder § ANY substance use (including tobacco)
 Identification of risk factors should")
GUIDELINES FOR THE CHRONIC USE OF OPIOIDS (ACOEM, 2011) Identification of risk factors should prompt the practitioner to EITHER § include consideration of factors in treatment OR § recruit assistance from another provider (such as a psychologist or pain management physician) to define relevant psychosocial factors and coordinate treatment § Develop a treatment plan addressing these factors or the role they play (hampering) rehabilitation

THE GOLDEN KEY Q. What is the most powerful differentiating variable between those who are employed and those who are not following traumatic injury? A. Psychological functioning. These factors are stronger predictors than injury severity / level. DATZ 2015

MODIFIABLE FACTORS Predictive of Higher RTW: § High motivation to work § Positive expectations about recovery § Functional beliefs about back pain, injury, and return-to-work § Absence of anxiety, insomnia, and depression § High self esteem & self efficacy § Active social functioning Sullivan, & Stanish, 2003; Berglind & Gerner, 2002; Schultz et al. , 2005; Buchbinder, Jolley, Wyatt, 2001 DATZ 2015
 Looked at 253 workers with back injuries. Expectations of recovery")
SCHULTZ ET AL. (2004) Looked at 253 workers with back injuries. Expectations of recovery were one of the most significant predictors of disability, RTW, and cost. - Correctly classifies who returns to work 85% of the time. Negative/adversarial response by employer or WC system to the claim has been clinically observed to prolong disability DATZ 2015

EVIDENCE FOR BIOPSYCHOSOCIAL MODEL Lost work productivity 1 § Job dissatisfaction & depression better predictors than physical injury Surgery Outcomes 2 § Psychological assessments predictive for spinal surgery response § Predicts 80% of response in both invasive & noninvasive procedures 1. 2. Bigos et al. (1992); Carragee (2005); Carragee et al. (2005); Jarvik et al. (2005); Krause et al. (1998) Block et al. (2001); Gatchel et al. (1995); Giordano & Lofland (2005)

Scientific findings have led to a new understanding of work injury that differs from a longstanding view that sees work injury as only physical, and as an isolated problem. Traditionally, the mind and the body have been believed to be separate.

BIOLOGICAL Medical Findings, Pre-existing Location, Intensity, Quality, Duration PSYCHOLOGICAL Beliefs, Experiences, Memories, Behaviors, Activity level, Mood, Emotions, Interpretation SOCIAL Spiritual Cultural Litigation Finances Family/Relationships BIOPSYCHOSOCIAL Model of Chronic Pain

MANY INSURERS ARE NOW REQUIRING PSYCHOLOGICAL EVALUATIONS Based on data which show that psychological evaluations and testing are predictive of opioid risk and recovery, based on specific psychological risk factors and the presence of certain conditions, insurers are increasingly requesting psychological screening for patients with chronic pain.

BIOPSYCHOSOCIAL LAWS Regulations and guidelines are increasingly recognizing science-based approaches “Biopsychosocial laws” now populate many evidence-based treatment guidelines § Official Disability Guidelines (ODG) § Work Loss Data Institute (WLDI) § American College of Occupational and Environmental Medicine (ACOEM) § The Reed Group (MDA) § Colorado Division of Workers Compensation § Washington State Dept of Labor & Industries § Texas Division of Workers Compensation

CO: DEFLATION OF COSTS FOR WORKERS' COMPENSATION VIA BIOPSYCHOSOCIAL LAWS 1980 s: CO work comp costs 2 – 4 x than most states. Reform in 1992 Prior to reform, the mean medical cost per claim (MMCC) in CO 38% higher than the mean of 44 other states combined. By 2007, MMCC for CO was 24% LOWER than 44 states, a 62% DECREASE Mean indemnity cost per claim was essentially the same as other states – a 62% reduction.

WHY THE COST REDUCTION? ONE MAIN CHANGE “Mandated Psychological Evaluation and Psychological testing 6 to 12 weeks after failure of conservative care” (PT, short acting medication, “rest”/off work) Why did this help so much?

MORE THAN MEETS THE EYE? MRI studies are often used to assess objective pathophysiology and quantify impairment Several studies shown that + MRI findings are common in people who are symptom free. Physical pathology accounted for ONLY 10% of disability in the year following injury Psych assessment was more predictive of future disability than MRI Psych factors accounted for 59% of disability Jensen et 1994, Carragee et al 2004, 2005; Burton et al, 1995
 Looked at 253 workers with back injuries. Expectations of recovery")
SCHULTZ ET AL. (2004) Looked at 253 workers with back injuries. Expectations of recovery were one of the most significant predictors of disability, RTW, and cost. Correctly classifies who returns to work 85% of the time. Negative/adversarial response by employer or WC system to the claim has been clinically observed to prolong disability

WHAT ARE WE DOING WRONG? A traditional approach is to keep the employee off work until she/he is “healed”. In many cases, this does not help.

RTW LIKELIHOOD AFTER # DAYS OFF

WORKER SATISFACTION WITH EMPLOYER RESPONSE PREDICTS RTW

COGNITIVE BEHAVIORAL THERAPY A specialized form of mental health counseling Evidence based, structured, focused & limited in duration Conducted by qualified healthcare professional Modifies negative patterns of thinking and behavior

COGNITIVE BEHAVIORAL THERAPY Helps the patient develop coping skills Coaches the patient in understanding chronic pain & what is happening to their body Empowers the patient to self manage symptoms Creates rewiring in the brain

NEUROPLASTICITY The brain can generate new cells at any age. § Neuroplasticity is the ability of the brain to lay down new pathways in light of new information. Chronic pain becomes “memorized” by the brain. § By 3 months the pain pathway is laid, due to frequency of neural impulses being fired, and the perceived importance of this information.

TALK TREATMENTS CHANGE THE BRAIN 19 studies on BRAIN CHANGES after psychotherapy for depression & various anxiety disorders have been published Typically talk treatments are compared with RX Both have effects Cognitive-behavioral therapy (CBT) alters brain function in patients suffering from major depressive disorder (MDD), panic disorder, social anxiety disorder, specific phobias, posttraumatic stress disorder

HOW THE BRAIN IN PAIN CAN BE REWIRED Trained Movements and Exercise help remap the area of the brain that represents the painful area Use of visualization, meditation Self soothing and self massage Relaxation, Biofeedback, Breathing Retraining Empower patients to export skills into daily life Educate about opioids and other medication classes

What if the pain never stops? What’s happening to my body? When it will heal? Will I will ever be the same? What if I get fired? I can’t take all this stress! DATZ 2015 Do I take my medication? Should I really exercise?

Negative emotions § Blame, anger, frustration, depression, helplessness § Lack of knowledge, Passivity of patient, and the belief by the person that they can be fixed by some external force, (when none exists) all serve to reinforce the pain pathway. § Add the negative cycle of challenges that often accompany the person being out of work, others not understanding, or having a worker’s compensation claim

HOW THE BRAIN IN PAIN CAN BE REWIRED Replace fear with curiosity and hope Trained Movements and Exercise help remap the area of the brain that represents the painful area Use of visualization, meditation Self soothing and self massage Relaxation, Biofeedback, Breathing Retraining Empower patients to export skills into daily life Educate about opioids and other medication classes

HOW DOES CBT WORK? How you think about a situation affects how you feel about it, which can effect what you do in response Ways of reacting to situations may be helpful or unhelpful

THE A-B-C MODEL A B C Activating Event Beliefs Consequences Pain flare up “My pain is only getting worse” Depression; anxiety about pain; worsened pain level

THE VICIOUS CIRCLE, Activating Event: you’ve had a work injury. Taken off work by your doctor. Depression, irritability, anger, anxiety set in. Distress & Deconditioning creates self fulfilling prophecy. Behavioral conseq: isolating, overmedicating, sedentary, avoidance and fear in activity. Beliefs: “I am worthless. I am no good to anyone. I cannot provide for my family. ” Psychological consequences: feeling low, rejected, sad, ashamed

CBT FOR CHRONIC PAIN It changes the way people view their pain. CBT can change thoughts, emotions, and behaviors related to pain, improve coping strategies, and put the discomfort in a better context CBT can also change the physical response in the brain that makes pain worse. Pain causes stress, and stress affects pain control chemicals in the brain, such as norepinephrine and serotonin. CBT reduces the arousal that impacts these chemicals. This, in effect, may make the body’s natural pain relief response more powerful.

PARADIGM SHIFT § Psych as “bad”, a liability, or to be used only when credibility is called into question § Psych as a Pandora’s Box § Psych as only dealing with pre-existing vulnerabilities § Use of Psych to deal with only pure “mental-mental” claims § The idea that psychological treatment is indefinite
 § > 50% Psychotherapy (CPT 90837) § Cognitive")
PSYCHOLOGICAL TREATMENTS Psychotherapy treatments (Evidence Based) § > 50% Psychotherapy (CPT 90837) § Cognitive Behavioral Therapy for Chronic Pain § Mindfulness Based Stress Reduction / Chronic Pain § Acceptance & Commitment Therapy Health and Behavioral treatments § < 50% psychotherapy (CPT 96150 – 96153) § Pain education and health coping skills only § Limited in scope, no testing, no “psych” Functional Restoration Approaches (CPT 97799) § At least 50% or > psych

COGNITIVE BEHAVIORAL THERAPY Effects are durable. Maintained at 6, 9 and 12 months. Determined to meet a high level of effectiveness for chronic pain Clients are taught skills to use for a lifetime. Low cost: psychotherapy is covered under most insurance, and if not, self pay is not unreasonable Low Risk - no side effects
 § Equal to back fusion surgery")
EFFECTIVENESS OF PSYCHOLOGICAL TREATMENTS Cognitive Behavioral Therapy (CBT) § Equal to back fusion surgery § Equal to physical therapy Using health care providers like nursing to address psychosocial and other complications can improve RTW for chronic pain and injury Mirza S. K. , & Deyo, R. A. (2007). Systematic review of randomized trials comparing lumbar fusion surgery to nonoperative care for ttreatment of chronic back pain. Spine, 32(7), 816– 823. Smeets, R. J. , Vlaeyen, J. W. , Hidding, A. , Kester, A. D. , van der Heijden, G. J. , van Geel, A. C. , et al. (2006). Active rehabilitation for chronic low back pain: cognitive-behavioral, physical, or both? First direct posttreatment results from a randomized controlled trial [ISRCTN 22714229]. BMC Musculoskeletal Disorders, 7, 5.

MEDITATION & PAIN Can lead to 40% to 60% reductions in pain compared to non – meditation and opioids More effective than narcotics in some patients No side effects, portable, self induced strategy Targets the same areas of the brain that are hyper activated in chronic pain

FMRI STUDIES OF BRAIN ACTIVATIONS DURING MEDITATION

NON OPIOID / NON MEDICATION/ COMPLEMENTARY TREATMENTS

PARADIGM SHIFT A shift towards investment in Recovery Mindset § Early Intervention § Emphasize return to work and job accommodation Openness to non opioid treatment: all parties! Understanding of the literature of chronic pain recovery & rehabilitation

GETTING “UNHOOKED” FROM OPIOIDS Alternative treatment modalities: 1. Cognitive-behavioral therapy 2. Functional Restoration 3. Yoga It’s time for transition away from a “medicalization-only mindset” Mark Pew, Claims Management
 Study Quite positive Effectiveness rates range from 65")
RTW OUTCOMES & FUNCTIONAL RESTORATION (2007) Study Quite positive Effectiveness rates range from 65 to 90% at years 1 or 2 A (2010) Study 55% RTW compared to 9% at baseline Even 5 years post injury, 70% of successful completers were RTW “Maintaining job status with the pre-injury employer is often best accomplished by the provision of suitable modified duties. ” • Worker attachment to job and staff was strongly predictive • Younger age, practice of sports, shorter sick leave strongly predictive • Failures predicted by surgery to same area post discharge, increased health utilization (>30 visits), higher pre-treatment levels of depression and perceived disability • Call to implement early in injury process

FRP INITIATED EARLY = BIG $AVINGS N = 1, 119 patients Group 1 : 4 to 8 months after injury Group 2: 9 to 18 months Group 3: 18 months Results: RTW: 88% RTW Work Retention: 80% Health care utilization: much reduced Groups did not significantly differ on these domains.
 had medical cost savings of 64% and")
COST SAVINGS Early intervention group (Group 1) had medical cost savings of 64% and productivity loss savings/disability savings of 80% Total economic cost savings of 170, 000 per claim If FRP was initiated early on, it cost 56% less than if initiated later on

CAN FUNCTION RESTORATION RESOLVE UNCERTAIN SURGICAL CANDIDATES? Recovery can be slowed by indecisiveness over optional surgery. (Approx 80% of spine surgeries are elective) Claimants may be slowed from enrollment in functional restoration pending resolution of the surgical decision A surgical option process was created: Allow person to enter Functional Restoration. Halfway through, make a determination about whether or not to move forward with surgery. If surgery elected, finish FRP when surgery is done.

RESULTS Patients attended 10 days FT. Then made a decision whether to pursue surgery vs not. Completion of FRP resolved surgical uncertainty in a large proportion of cases: 73% Declined surgery. § Types of surgeries declined: § Cervical spine fusion (13%) § Lumbar spine fusion (41%) § Lumbar spine (other) 22% § Upper extremity (13%) § Knee (13%)

§ Despite an opportunity to re enter the rehab program, those who were denied surgery by their insurer, only 50% of those took it. § People who persistently sought surgery, contrary to the recommendations of a surgeon, frequently fail rehab programs.

CASE EXAMPLE #1 54 -year-old Caucasian female Nurse, at Gulfport area Injured on the job in 2004 lifting a patient- left work permanently in 2006 Chronic low back pain Had been on a Fentanyl patch for years & was not ready to stop, also taking muscle relaxer and PRN percoset Symptoms of depression with suicidal ideation & anxiety Attended outpatient counseling briefly & saw a psychiatrist- minimal benefit Attended PT with aquatic therapy- minimal benefit Attended PRP January & February 2016 Discharged with no restrictions and put at MMI

CASE EXAMPLE #2 33 -year-old African American male Injured on the job in 2014 in a motor vehicle accident- off work since accident Neck & upper back pain, diagnosed with severe whiplash Tingling in hand & arm Took pain medication- minimal benefit Attended PT- minimal benefit Obtained injections- mild benefit Symptoms of depression & anxiety Attended PRP program November & December 2014 Returned to work March 2015. No restrictions.
- Slides: 68