Amenorrhea Professor Ahmed Abdel Aziz Ismail Amenorrhea Primary

Amenorrhea Professor Ahmed Abdel Aziz Ismail

Amenorrhea • Primary – Absence of menses by age 16 with normal secondary sexual characteristics – Absence of menses by age 14 without secondary sexual development • Secondary – Absence of menses for 6 months in a previously menstruating female
 Chemical control Norepiniphrine (+) Endorphines (-) Hypothalamus")
CNS-Hypothalamus-Pituitary Ovary-uterus Interaction Neural control Dopamine (-) Chemical control Norepiniphrine (+) Endorphines (-) Hypothalamus Gn-RH ± – Ant. pituitary ACT H Estrogen FSH, LH Ovaries Uterus Menses TSH Progesterone
 – Requires estrogen • Pubarche/adrenarche (pubic hair")
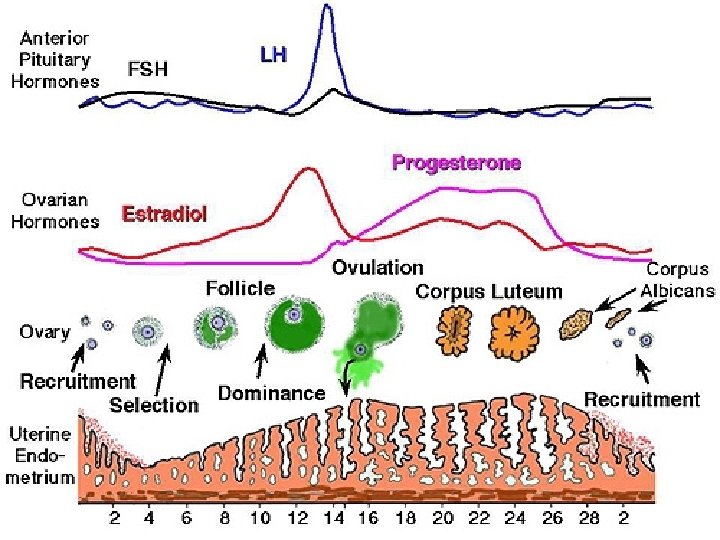
Events of Puberty • Thelarche (breast development) – Requires estrogen • Pubarche/adrenarche (pubic hair development) – Requires androgens • Menarche – – – Requires: Gn. RH from the hypothalamus FSH and LH from the pituitary Estrogen and progesterone from the ovaries Normal outflow tract

Are there secondary sexual characteristics?

Primary Amenorrhea • Is there normal development of secondary sexual characteristcs? NO Think hypogonadism or hypogonadotropism

Amenorrhea with Immature Secondary Characteristics FSH Serum level Low / normal Hypogonadotropic hypogonadism High Gonadal dysgenesis
 – Gonadal dysgenesis –")
Primary Amenorrhea with Immature Sexual Characteristics • Hypogonadism (gonadal failure) – Gonadal dysgenesis – Irradiation – Chemotherapy – Galactosemia • Note: gonadotropins (FSH/LH) will be high, similar to menopause
 – Gonadal dysgenesis –")
Primary Amenorrhea with Immature Sexual Characteristics • Hypogonadism (gonadal failure) – Gonadal dysgenesis – Irradiation – Chemotherapy – Galactosemia • Note: gonadotropins (FSH/LH) will be high, similar to menopause
 - Turner variants")
Gonadal Dysgenesis • Chromosomally abnormal - Classic turner’s syndrome (45 XO) - Turner variants (45 XO/46 XX), (46 X-abnormal X) - Mixed gonadal dygenesis (45 XO/46 XY) • Chromosomally normal - 46 XX (Pure gonadal dysgeneis) - 46 XY (Swyer’s syndrome)

Primary Amenorrhea with Immature Sexual Characteristics • Hypogonadotropism – Hypothalamic dysfunction • • Kallmann syndrome Anorexia nervosa Space-occupying lesion of CNS Marijuana use – Pituitary damage (surgery/radiation) – Constitutional delay

Are there secondary sexual characteristics? yes

Primary Amenorrhea • Is there normal development of secondary sexual characteristics? YES • Think – Pregnancy – Mullerian anomaly – Androgen insensitivity

Primary Amenorrhea with Normal Secondary Characteristics • Mullerian Anomalies – Mullerian agenesis (Mayer-Rokitansky-Kuster. Hauser syndrome) – Imperforate hymen – Transverse vaginal septum
 • 15% of primary amenorrhea • Normal secondary development &")
Mayer-Rokitansky-Kuster-Hauser Syndrome (utero-vaginal agenesis) • 15% of primary amenorrhea • Normal secondary development & external female genitalia • Normal female range testosterone level • Absent uterus and upper vagina & normal ovaries • Karyotype 46 -XX • 15 -30% renal, skeletal and middle ear

Imperforate Hymen

Androgen Insensitivity • Normal breasts but no sexual hair • Normal looking female external genitalia • Absent uterus and upper vagina • Karyotype 46, XY • Male range testosterone level • Treatment : gonadectomy after puberty + HRT

Primary Amenorrhea • Evaluation – Pregnancy test – Physical exam to determine presence of uterus – FSH – Karyotype

Primary Amenorrhea • Treatment – Cyclic estrogen/progestin – Remove gonadal streaks if XY or mosaic • Increased (52%) risk of gonadoblastomas, dysgerminomas, and yolk sac tumors – Pulsatile Gn. RH for ovulation induction in selected patients – Surgical resection of intrauterine, cervical, and vaginal adhesions/septa

Secondary Amenorrhea • • Pregnancy! CNS disorders Pituitary gland Thyroid Ovary Uterus Systemic disorders – Renal failure, liver disorders, DM • Medications: anti-psychotics, reserpine

Secondary Amenorrhea • CNS disorders – Chronic hypothalamic anovulation • Stress • Increased exercise levels • Anorexia nervosa – Head trauma – Space-occupying lesions

Secondary Amenorrhea • Pituitary disorders – Hyperprolactinemia • • Prolactinoma Medications PCOS Renal failure – Hypoprolactinemia • Pituitary resection • Sheehan’s syndrome • Thyroid disorders – Hyper- or hypothyroidism

Secondary Amenorrhea • Ovulation disorders – Polycystic ovarian syndrome – Premature ovarian failure • Uterine abnormalities – Asherman’s syndrome – Cervical stenosis • Drug-induced amenorrhea – Hormonal contraceptives – Gn. RH analogues

Asherman’s Syndrome

Secondary Amenorrhea History – Nutrition/exercise habits, weight change – Sexual/contraceptive practice – History of uterine/cervical surgery • Physical exam – – Height/weight Hirsutism Galactorrhea Estrogen status of tissues • Laboratory – Bh. CG PRL & TSH progesterone challenge FSH if high karyotype

Negative Pregnancy. test TSH , PROLACTIN, Progesterone challenge test without withdrawal bleeding hypoestrogenic anovulation +ve. est/progest challenge test Normal FSH. Low E 2 hypothalamicpituitary failure FSH>30 -40 compromised outflow tract -ve. est/progest challenge test Normal FSH + Normal E 2 repeat Premature Ov Failure HSG OR hysteroscopy Asherman’s

Secondary Amenorrhea • Treatment goals – Discovery and treatment of underlying cause – Hormone replacement – Menses every 1 -3 months – Pregnancy • Ovulation induction • Gn. RH pump • HMG/HCG

• Thank you
- Slides: 29