Amenorrhea Khalid Akkour MD FRCSC Definitions Classification Amenorrhea



")

















- Slides: 23
Amenorrhea Khalid Akkour, MD FRCSC
Definitions & Classification • Amenorrhea: Absence of menses. • Primary amenorrhea: Non occurrence of menarche by age of: • 14 with no secondary sex characters • 16 (18) with secondary sex characters. • Secondary amenorrhea: Absence of menses for 3 successive cycles.
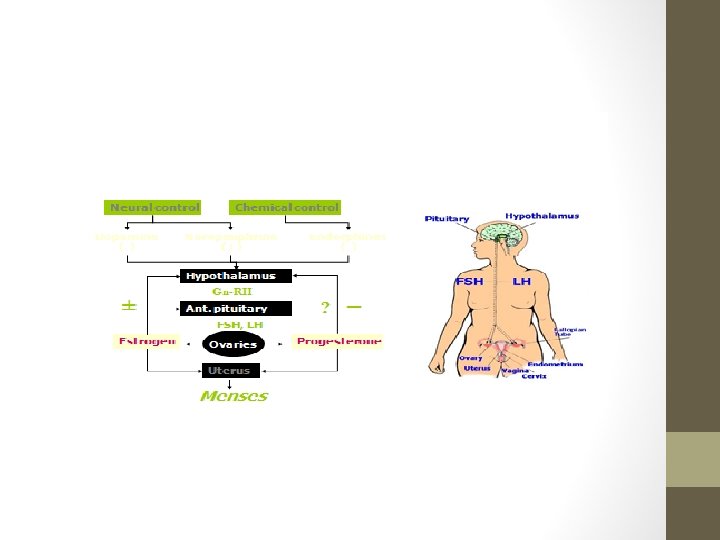
Amenorrhea Pathologic False Physiologic True Imperforate hymen Vaginal T. septa Cervix CNS Puberty Hypothalamic Menopause Pituitary Pregnancy Ovarian Lactation Uterine General
False amenorrhea (Cryptomenorrhea)
Cryptomenorrhea • Due to outflow obstruction. • The most common cause is imperforate hymen. • Blood accumulate behind the hymen hematocolpos Hematometra Pelvic hemorrhage. • Diagnosis: • • • P. amenorrhea with good 2 ry sex characters. PMS. Urinary symptoms. Abdominal mass ? ? . Local examination is diagnostic. • Treatment: Cruciate incision under anesthesia Slow evacuation + antibiotics.
True amenorrhea
CNS Causes • Psychological troubles: • Psychosis # neurosis. • Pseudocyesis. • Anorexia nervosa. • Chronic stresses. • Weight loss. • Exercise: • • Loss of body fat. Stress of competition. Hyperthermia and dehydration. Euphoria of winning causing increased opiates.
Hypothalamic causes • Destruction: • • Trauma Inflammation. Tumors. Infiltrations. • Drugs: • Estrogens. • CNS affecting drugs. • Dysfunction & congenital disorders: • • • Chiari Frommel syndrome. Del Castillo syndrome. Kallmann syndrome. Laurence Moon Biedl syndrome. Frohlich syndrome.
Pituitary causes • Destruction: • Infiltrations. • Tumors. • Sheehan syndrome. • Drugs: • Estrogens. • Prolactin inducing drugs. • Dysfunction and congenital disorders: • Levi Lorain syndrome. • Empty sella syndrome. • Prolactinomas.
• Congenital: Ovarian causes • Turner. • Androgen insensitivity syndrome. • Traumatic: • Surgical removal. • Irradiation. • Inflammatory: • Mumps. • PID. • TB. • Neoplasia: • Benign. • Malignant. • Dysfunctions: • PCO. • Resistant ovary syndrome.
• Congenital: Uterine causes • Mullerian agenesis. • Uterine atresia • Severe hypoplasia. • Traumatic: • Surgical removal. • Irradiation. • Inflammatory: • Asherman syndrome. • TB. • Neoplastic: • Obstructing the cervix. • Dysfunctions: • Insensitive endometrium.
General causes • DM: • Glucose metabolism. • Ketosis. • Immunological. • Thyroid: • Hyper. • Hypo. • Adrenal: • Addison. • Cushing. • Debilitating diseases.
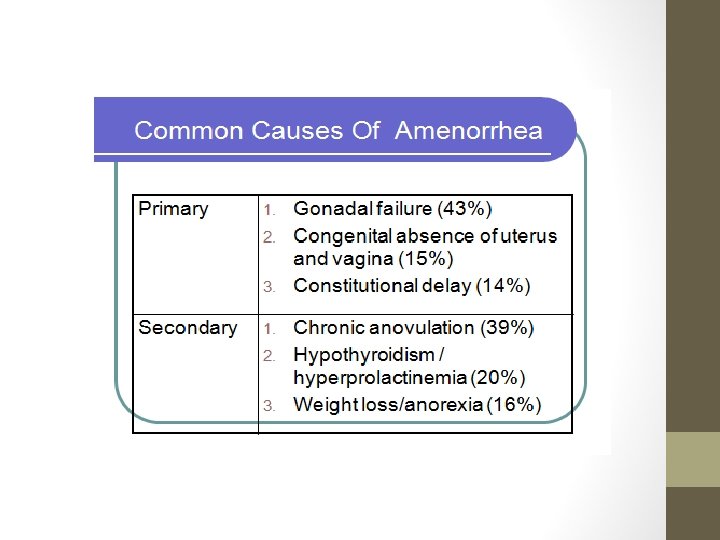
Causes of 1 ry amenorrhea 1 - Cryptomenorrhea: All congenital causes. 2 - True: • Psychological disturbances before menarche. • Congenital diseases in the hypothalamus or pituitary. • Ovarian dysgenesis and removal or destruction before menarche (T. B, irradiation). • Uterine aplasia or severe hypoplasia, T. B or removal before menarche. • General cause before menarche. • The most common causes of primary amenorrhea: • Gonadal dysgenesis. • Mullerian agenesis. • Complete AIS.
Causes of 2 ry amenorrhea • Physiological: • Pregnancy, lactation, after menopause. • Cryptomenorrhea: Any acquired cause. • True: • Psychogenic disorders after menarche, Chiari Frommel and Del Castillo syndromes, drugs, OCs, destruction by trauma, infections, tumors after puberty. • Sheehan syndrome, Simmond's disease, destruction and tumors after puberty. • Ovarian failure, PCO and ovarian tumors. • Intrauterine synechia, hysterectomy or T. B endometritis after puberty. • Any general cause after puberty.
Diagnosis of amenorrhea n. History: • • • Age, occupation, residence, habits and education. Primary or secondary amenorrhea. History of psychogenic disorders. History of neurological disturbances. History of endocrinological disorders. Past history of operations, pelvic infections, T. B, long drug course or irradiation. • Family history of similar condition, familial disease.
Diagnosis of amenorrhea • Examination: • Psyche, height, weight and span measure. Nutritional status should be also evaluated. • Secondary sexual characters. • Evidence of neurological disorders specially central lesions. • Evidence of endocrinological disorders with special reference to galactorrhea and hirsutism. • Evidence of general disease as heart, chest, renal or hepatic disorder. • Abdominal masses (ovarian, adrenal, renal hepatosplenomegaly or ascites). • External genital anomaly or hypoplasia. • Pelvic examination (PV or PR) for uterine and ovarian abnormalities.
Diagnosis of amenorrhea CNS Hypothalamus Pituitary Ovary Uterus Outflow tract
Diagnosis of amenorrhea • Special investigations – Step I: • • • Search for specific disease if suspected. Pregnancy test. TSH assay. Prolactin assay. Progesterone challenge test: • If (+)ve withdrawal Normal outflow tract and well estrogenized cases The cause is anovulation. • If (-)ve withdrawal Hypoestrogenic state or uterine cause step II.
Diagnosis of amenorrhea • Special investigations – Step II: • Give estrogen + Progesterone: • If (-)ve withdrawal Uterine cause. • If (+)ve withdrawal Normal outflow tract and uterus, and there is ovarian failure Step III • Special investigations – Step III: • Measure FSH: • If high Ovarian cause. • If low central cause.
Treatment of amenorrhea Treatment of the cause
THANK YOU