Amenorrhea Dr Zainab A A Jaafar Objective At

Amenorrhea Dr. Zainab A. A. Jaafar

Objective: At the end of this lecture, the 5 th year student should be able to 1. Define the primary amenorrhea 2. Understands the clinical types of primary amenorrhea 3. Understands the causes of primary amenorrhea 4. State line of management of primary amenorrhea 5. Describe the clinical feature and management of TURNER’S SYNDROME (45 X AND MOSAICS)

Definition: Amenorrhea: defined as the absence of menses

Clinical types: Physiological: q Primary: Before puberty q Secondary: During pregnancy, lactation, menopause Pathological q primary q secondary

Definition: • Primary amenorrhea: when girls fail to menstruate by 16 years of age. Irrespective of the presence or absence of secondary sexual characteristics (the girl has never menstruated before)

Definition: q. Secondary amenorrhoea: is absence of menstruation for more than 6 months in a normal female of reproductive age who had menses previously and that is not due to pregnancy, lactation or the menopause.

Definition: There at least five basic factors involved in the onset and continuation of normal menstruation. 1. 2. 3. 4. 5. Normal female chromosomal pattern (46 XX). Coordinated hypothalamopituitary ovarian axis. Anatomical presence and patency of the outflow tract. Responsive endometrium. Active support of thyroid and adrenal glands.
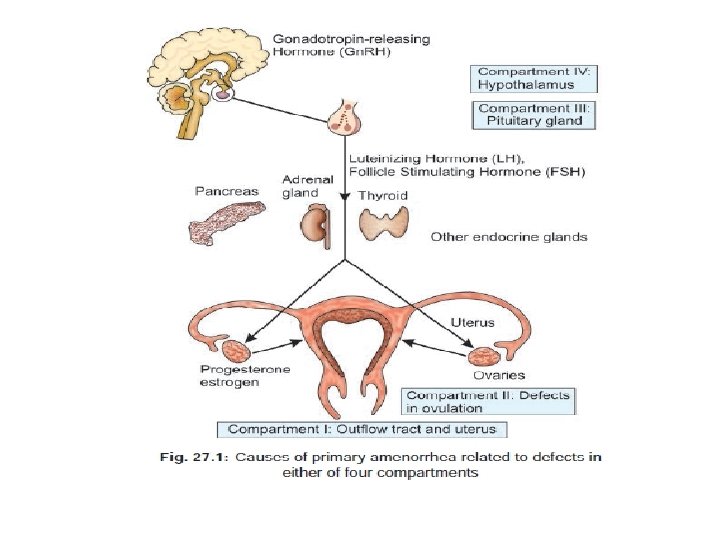

Etiology: is classified according to the presence or absence of secondary sexual characteristics

I. Absent breast development; uterus present • • • Gonadal failure: 45, X (Turner syndrome) 46, X, abnormal X (e. g. , short or long arm deletion) Mosaicism (e. g. , X/XX, XXX) 46, XX or 46, XY pure gonadal dysgene 17α hydroxylase deficiency with 46, XX, CAH

I. Absent breast development; uterus present Hypothalamic failure secondary to inadequate Gn. RH release 1. Insufficient Gn. RH secretion because of neurotransmitter defect 2. Congenital ( Isolated gonadotrophin relesasing hormone deficiency Kallmann’s syndrome) 3. Congenital anatomic defect in central nervous system 4. CNS neoplasm (craniopharyngioma)

I. Absent breast development; uterus present Pituitary failure 1. Isolated gonadotrophin insufficiency (thalassemia major, retinitis pigmentosa) 2. Pituitary neoplasia (adenoma) 3. Mumps, encephalitis 4. Newborn kernicterus 5. Prepubertal hypothyroidism
, 46 XY")
II. Breast development; uterus absent 1. Androgen insensitivity syndrome (Testicular feminization syndrome), 46 XY 2. Congenital Absence of the Uterus (Uterine Agenesis, Uterovaginal Agenesis, Mayer Rokitansky Küster Hauser Syndrome)

III. Absent breast development; uterus absent 1. 17, 20 desmolase deficiency 2. 17 hydroxylase deficiency with 46, XY karyotype 3. Agonadism

IV. Breast development; uterus present • Constitutional delay • Hormonal o Hypothalamic and pituitary dysfunction —eg. Stress, weight loss, excessive exercise, anorexia nervosa, chronic systemic disease (eg. tuberculosis). o approximately 25% of these individuals had hyperprolactinemia and prolactinomas

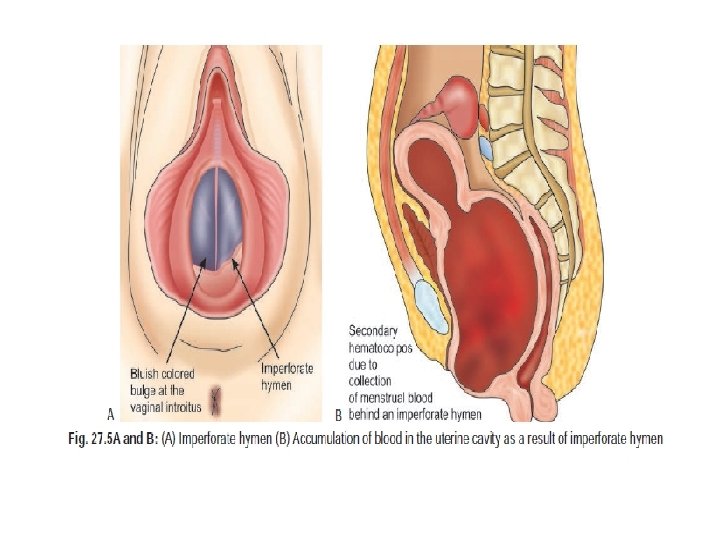
IV. Breast development; uterus present • Developmental defect of genital tract 1. Imperforate hymen. 2. Transverse vaginal septum. • endocrine 1. Metabolic disorders 2. Juvenile diabetes.

IV. Breast development; uterus present • Systemic illness 1. Malnutrition, anemia 2. Weight loss 3. Tuberculosis. • Unresponsive endometrium 1. Congenital 2. Uterine synechiae (tubercular).

Investigations: investigation is started if 1. No periods by 16 years but secondary sexual characters are present. 2. No periods by 14 years in the absence of secondary sexual characters.

History q. Aske other stages of puberty: Growth spurt, axillary and pubic hair, breast development(Lack of pubertal development suggests an ovarian/pituitary failure or a chromosomal abnormality)

History qcyclical abdominal pain and sometimes urinary retention suggestive of outflow obstruction q Clinical features of virilization eg. hirsutism q. Recent changes in weight( loss or gain) within short of time , exercise habits, or recent life events causing stress

History q. History of visual field defects q. Past medical diseases : eg. cushing syndrome, tuberculosis or diabetes , Any neonatal and childhood diseases( eg. Neonatal crisis, suggestive of adrenal cause)

History qsexual history qdrug history, e. g. use of metoclopramide, antipsychotics, previous radiotherapy and chemotherapy qfamily history of the same problem (of delayed menarche) in the family or absent puberty

Examination: q height, weight, BMI qexamine for secondary sexual characteristic*( eg. breast growth, pubic and underarm hair qfeature of endocrine diseases( Hirsutism, acne, striae, increased pigmentation q Vitiligo—may be seen associated with autoimmune conditions of ovarian failure

Examination: q Breast examine: • development • galactorrhea q. Stigmata of chromosomal abnormalities eg. Features of Turner’s syndrome—low hairline, webbed neck, widely spaced nipples. q. Abdominal examination for masses.
 q inspect the vulva")
Examination: Genital examination: q pubertal hair development q Clitoral size(clitoromegaly) q inspect the vulva for any abnormality such as • 1 - Tense bulging bluish membrane (imperforated hymen) • 2 -vaginal septum q pelvic examination not indicated in sexually in active female so we do rectal examination : for the Presence of cervix and uterus

Examination: Visual field exam Assess visual fields and CNS examination (Kallmann syndrome or pituitary tumor)

Investigation • The first step in the work-up of primary and secondary amenorrhea is a pregnancy test • Bone X ray’s for age estimation. • Pelvic ultrasound - Rarely may need MRI or CT of the abdomen scanning to assess pelvic anatomy. qfor presence or absence of the uterus and ovaries qto detect hematocolpos and hematometra
 v 45")
Investigation • karyotype : v 46 XY : Andogen Insensitivity (TSF syndrome) v 45 X 0 –turner syndrome • LH, FSH: ü Elevated LH, FSH: Hypergonadotropic Hypogonadism ( eg. gonadal dysgenesis) ü Low LH, FSH: Hypogonadotropic hypogonadism (intracranial leasion)

Investigation • Prolactin levels: Elevated indicates Prolactinoma • X ray or CT or MRI imaging of pituitary fossa : to rule pituitary tumors • Ovarian biopsy if suspect Resistant ovary syndrome. Histopathology illustrating absence of oocytes
 • Gn. RH stimulation test:")
Investigation • Thyroid function test(T 3, T 4, TSH) • Gn. RH stimulation test: If Gn. RH administered • increase pituitary gonadotropins( LH FSH) is the probable cause is hypothalamic dysfunction • no rise of gonadotropins( LH FSH): pituitary disorders

Investigation • serum progesteron: • high serum progesteron: sent for 17 -OHprogesterone , Urinary pregnanetriol and cortisol • Low serum progesteron: Resistant ovary syndrome , Gonadal agenesis

Management Is based on the etiology, and the presence or absence of secondary sexual characteristics.

Management • If constitutional delay and secondary sexual characteristics are complete no need to suggest any treatment apart from annual review until she has menstruation, some use COC pills to promote menstruation as this will reassure her that menstruation can occur. .

Management Outflow obstruction: Surgical management • Imperforate hymen; cruciate incision of the hymen or hymenectomy. • Transverse Vaginal Septum; Excision of the septum depending on its level within the vagina.

Management Absent uterus: 1. Girl managed by special psychological counseling as she got problem regarding their future sexual activity & infertility. 2. Vagina is created at appropriate time (Vaginoplasty ) by surgical or non surgical way using vaginal dilators. 3. Girl with XY Karyotype: The gonads should be removed after puberty( Gonadectomy ). because of increased development of seminoma or dysgerminoma

Management • Turner’s syndrome: short-term use of estrogen and progesterone at least for the development of secondary sex characters

Hypothalamic pituitary ovarian axis defect 1. Severe defect may not respond 2. isolated gonadotropin deficiency (like Kallmann’s syndrome) responds to pulsatile Gn. RH (for ovulation) and estrogen, progesterone (for menstruation) 3. Hypothalamic pituitary tumors eg. (craniopharyngioma) may need surgical excision or radiotherapy 4. If pituitary microadenoma: then treatment is with Bromocriptine or Cabergoline, macroadenoma may necessitate surgery or radiotherapy
 do not respond to thyroxin. Mild")
Management • Thyroid and adrenal diseases: – (Cretinism) do not respond to thyroxin. Mild hypothyroids respond well – Adrenogenital syndrome with enlarged clitoris treated by excise clitoris (clitoroplasty) as early as possible to avoid psychological trauma – Corticosteroids are useful in 17 α hydroxylase deficiency

Management • Metabolic and nutritional diseases: – Hypoglycemic agents and insulin in case of diabetics – Anti-TB treatment for TB – Anemia treatment – Malabsorption to be treated – Adequate nutrition in case of weight loss

Management • Unresponsive endometrium: – For TB synechiae: Adhesiolysis followed by incretion of IUCD and high dose of estrogen and progesterone to control for withdrawal bleeding – Receptor abnormal—no treatment
 • This is probably the commonest abnormality in")
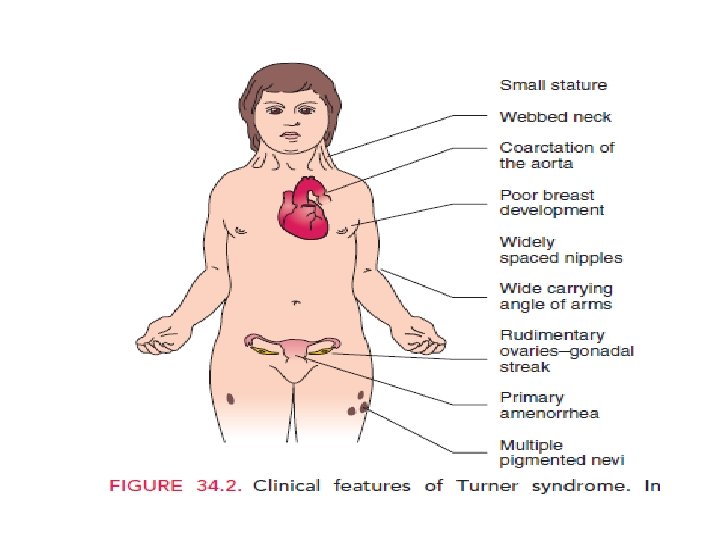
TURNER’S SYNDROME (45 X AND MOSAICS) • This is probably the commonest abnormality in females involving the sex chromosomes. Although 1 in 2500 live-born girls are affected, most pregnancies with this abnormality miscarry, probably secondary to major cardiac defects. • Turner syndrome (45, X) is characterized :
 q. The most common genotype is 45, X,")
TURNER’S SYNDROME (45 X AND MOSAICS) q. The most common genotype is 45, X, which is accompanied by nonfunctional streak ovaries and primary amenorrhea q Mosaicism (45, X/46, XX) may occur; these women may have some ovarian function through early adulthood, and may become pregnant, but then progress to secondary amenorrhea
 • • At birth by: low weight short")
TURNER’S SYNDROME (45 X AND MOSAICS) • • At birth by: low weight short stature edema of the hands and feet Loose skin folds on the neck.

Adolescent patients have : q. Growth failure: low birth weight and short stature; qovarian failure: no secondary sexual development in most cases qoccasionally secondary amenorrhea in mosaicism; qa low posterior hairline qwebbed neck qprominent ears

qinverted, widely spaced nipples, and shield chest qepicanthal folds qrenal dysgenesis; qleft sided cardiac malformations, coarctation of the aorta; qdistortion of the Eustachian tube leading to otitis media; qnail dysplasia; qeye deformities.

qincreased carrying angle at the elbow qcubitus valgus; qshort fourth metacarpal; qhigh, arched palate, micrognathia and defective dental development; q. Streak gonads: do not need to be removed as there is no Y chromosome present and no risk of malignancy. q Intelligence is usually normal, but there is risk of impairment of non verbal skills, e. g. maths

Treatment: The physician should start growth hormone at age of 10 year and a very low dose of estrogen usually started after the age of 12 to encourage steady growth of the breasts; as high dose of estrogen promotes epiphyseal fusion, which stops further growth. The dose of estrogen is gradu ally increased over 2 years.

Treatment: • The uterus will respond to estrogen therapy, once adult size uterus is found and ET more than 5 mm we start progesteron cyclically to produce regular endometrial shedding

Treatment: • HRT should be continued until at least the age of 50 years to decrease the risk of osteoporosis. For girls with mosaicism. • Cryopreservation of ovarian tissue may be an option for future fertility.

long term health complications • Cardiac: hypertension; coarctation of the aorta; bicuspid aortic valve; dissecting aortic aneurysm; diabetes; hypothyroidism; coeliac disease; • sensorineural hearing loss • renal disease: duplex system, horseshoes kidney

long term health complications • eye problems – red–green color blindness • skeletal: Increased risk of osteoporosis if insufficient estrogen therapy , juvinaile rheumatoid arthritis • Premature mortality in women with Turner’s syndrome is 3 times higher than in the general population.

long term health complications After treatment with donor oocytes. increased risk of com plications in the preg nancy including : 1. Diabetes 2. Hypertension 3. Delivery by caesarian section (CS) may be required because of the woman’s short stature (CPD). 4. IUGR: because of small uterus 5. rate of miscarriage 6. Rate of dissection aorta

Thank you
- Slides: 55