Amenorrhea Diana Haddad Amenorrhea the absence of menses

Amenorrhea Diana Haddad
. Physiological : before puberty, pregnancy, lactation , menopause")
Amenorrhea ( the absence of menses). Physiological : before puberty, pregnancy, lactation , menopause Primary : Absence of menses at age 14 without secondary sexual characteristics OR. Absence of menses at age 16 with secondary sexual characteristics Secondary : (in a female who is menstruating) -Absence of menses for 3 consecutive cycles (if regular) or 6 months (if irregular).

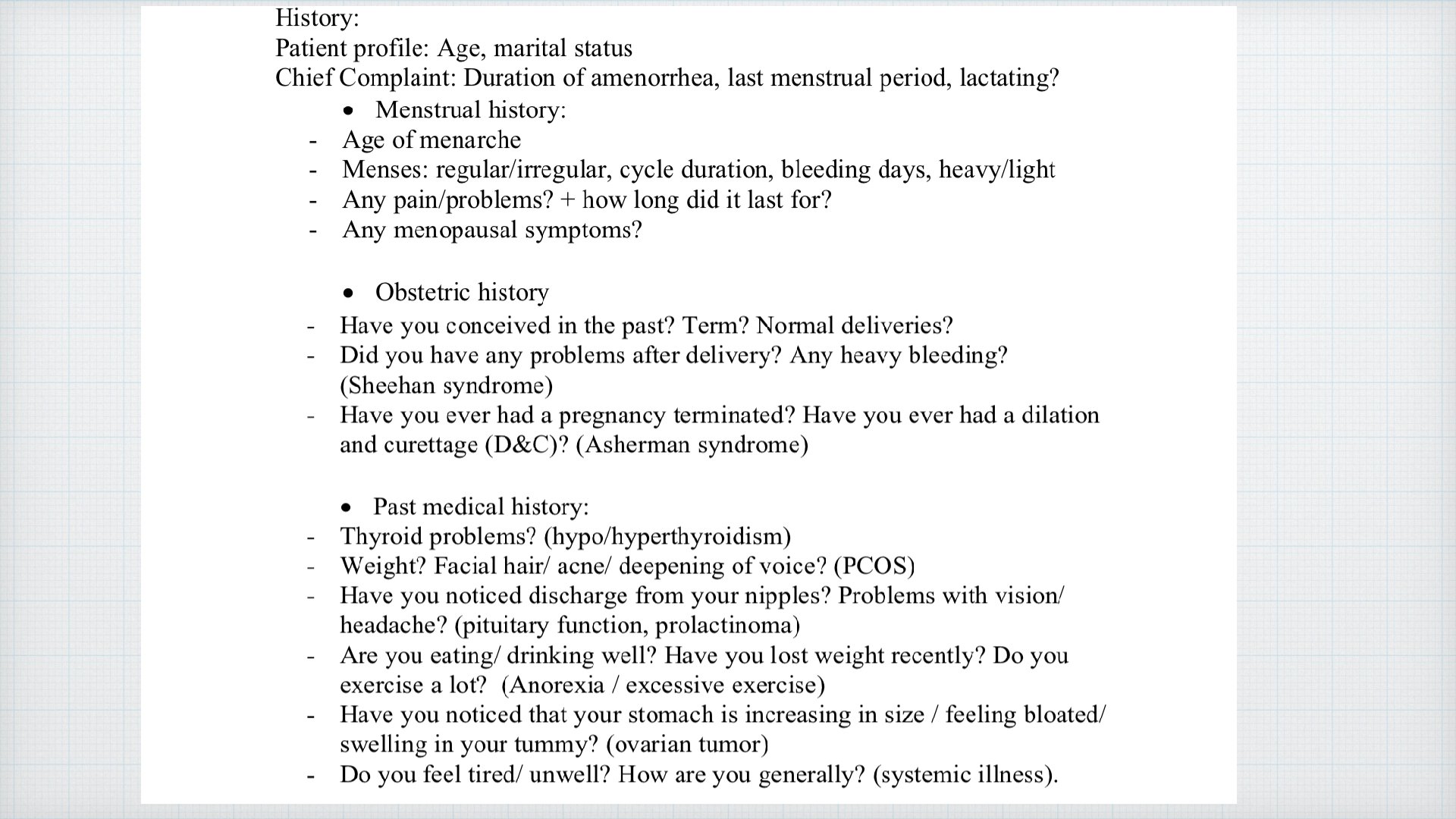
HPO axis Case: 16 yo female cam to clinic complaining from absent period and she had never come before , what is the first thing you looking for? !
 If")
If secondary sexual characteristics are present so HPO axis is working (functional ) If not present so the problem in the axis

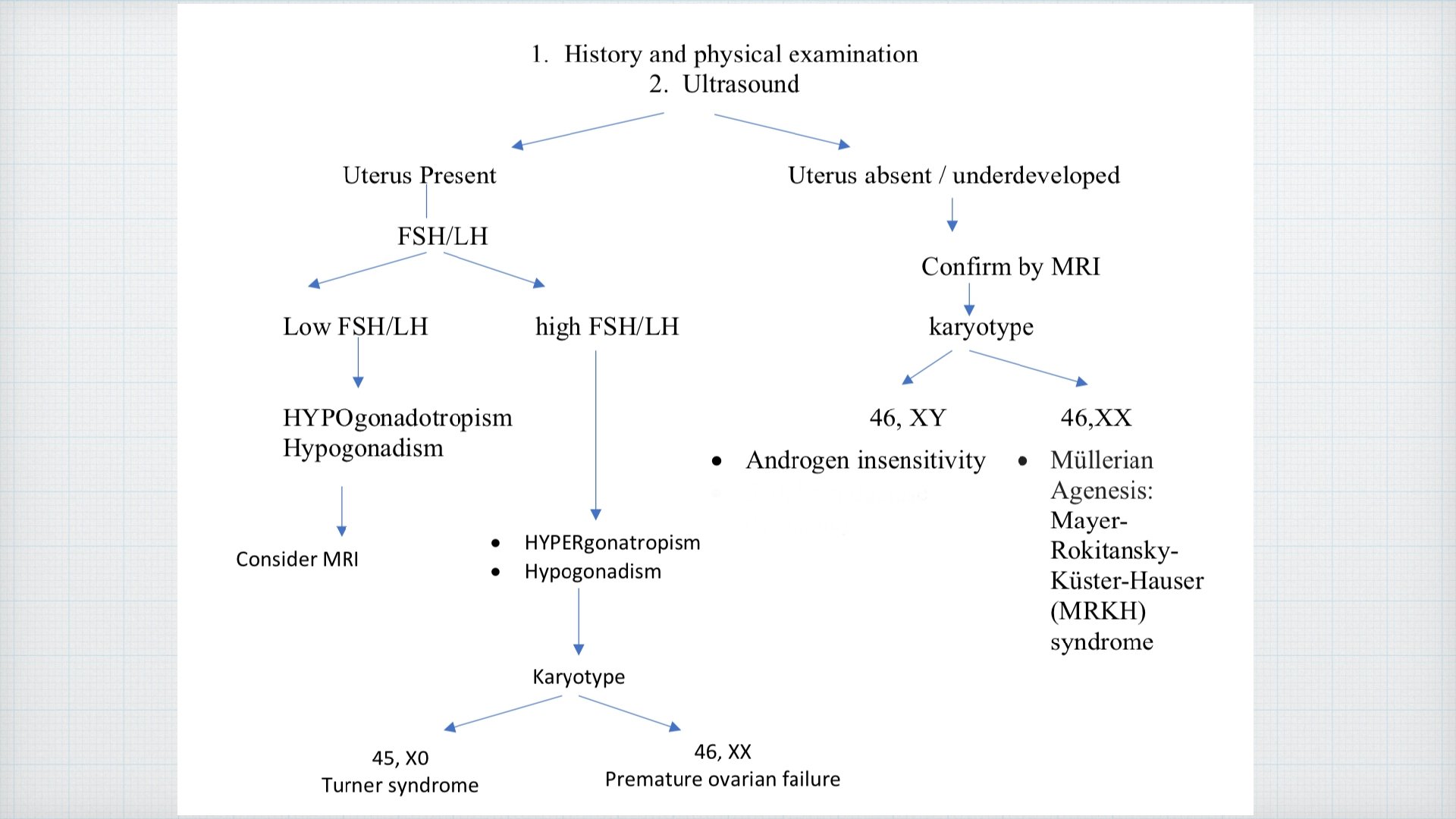
To know where is the problem in HPO axis by: Fs. H: If high : ovarian cause ( no estrogen ) , so we do karyotype ( could be 45 XO or 46 XX ) If low : hypothalamus or pituitary cause If normal : it’s usually in secondary amenorrhea and 2 ary sexual characteristics will be present

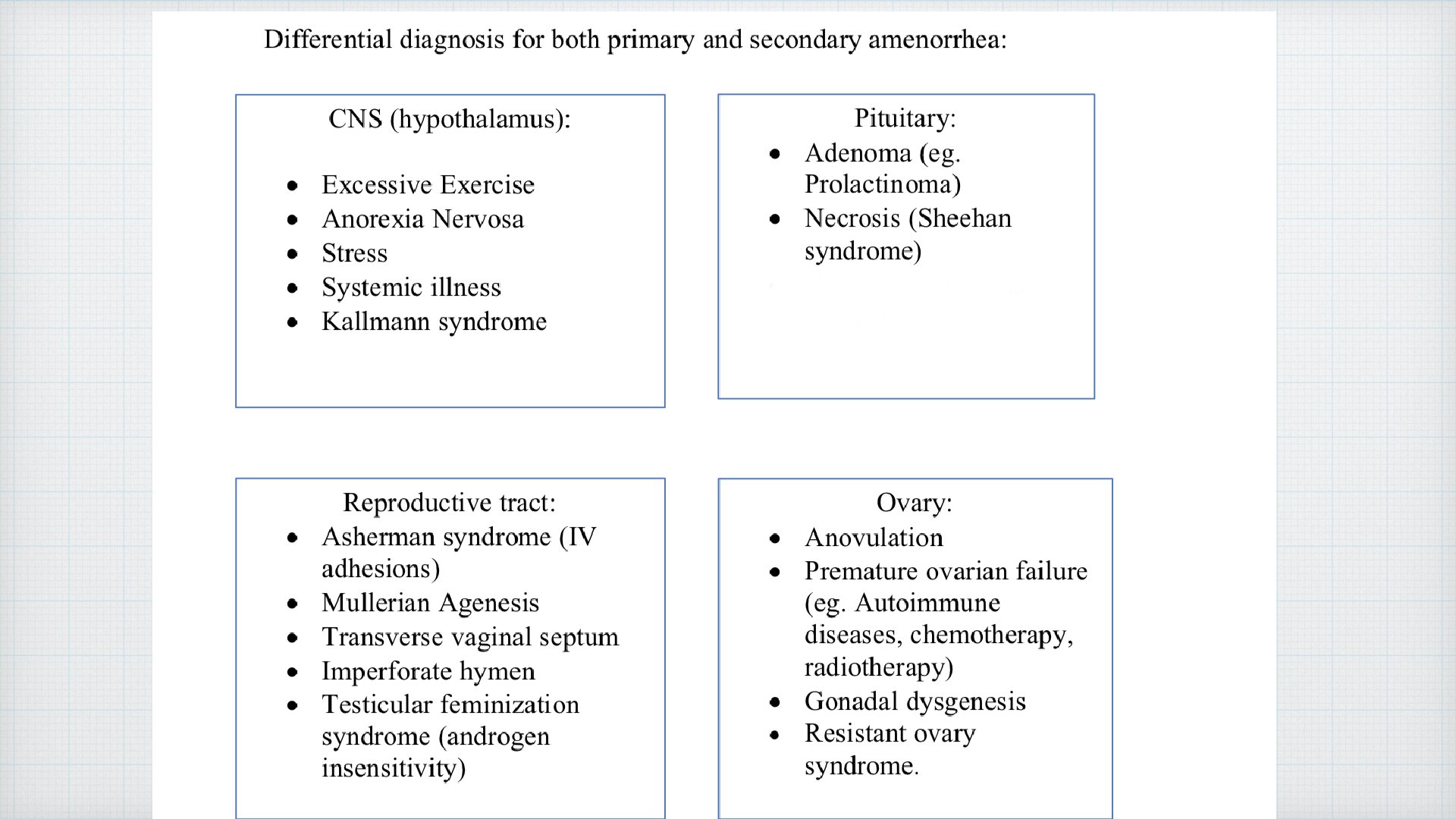
Causes : 1 - outflow tract obstruction 2 -uterine causes 3 - ovarian causes 4 - pituitary causes 5 - hypothalamus causes
 Tx")
Outflow tract obstruction 1 -Cervical obstruction ( tumor , atresia , stenosis ) Tx : hystrectomy 2 - transverse vaginal septum 3 - imperforated hymen (Last 2 caused by müllerian defects that cause obstruction of the vaginal canal) Cervical stenosis

In imperforate hymen: females usually presents to the clinic with monthly dysmenorrhea BUT NO vaginal bleeding, on rectal examination, a vaginal bulge and midline cystic mass can be felt. On Ultrasonography �hematocolpos : medical condition in which the vagina fills with menstrual blood. There is a uterus and ovaries. Treatment: hymenectomy. If a patient presents with similar symptoms but NO vaginal bulge, US confirms normal uterus and ovaries, the diagnostic tool of choice is MRI �if it confirms a transverse vaginal septum �surgery is indicated.

Blood color is chocolate why ? ? ?
 congenital")
Uterine causes 5% : 1 - Müllerian agencies : Mayer– Rokitansky–Küster–Hauser syndrome (MRKH) congenital malformation characterized by a failure of the Müllerian duct to develop, resulting in a missing uterus and variable degrees of vaginal hypoplasia of its upper portion. there anomalies within the uterus or vagina, please make sure to investigate the urinary tract for anomalies ( due to embryological origins ) by intravenous pyelogram or diagnostic radiography.
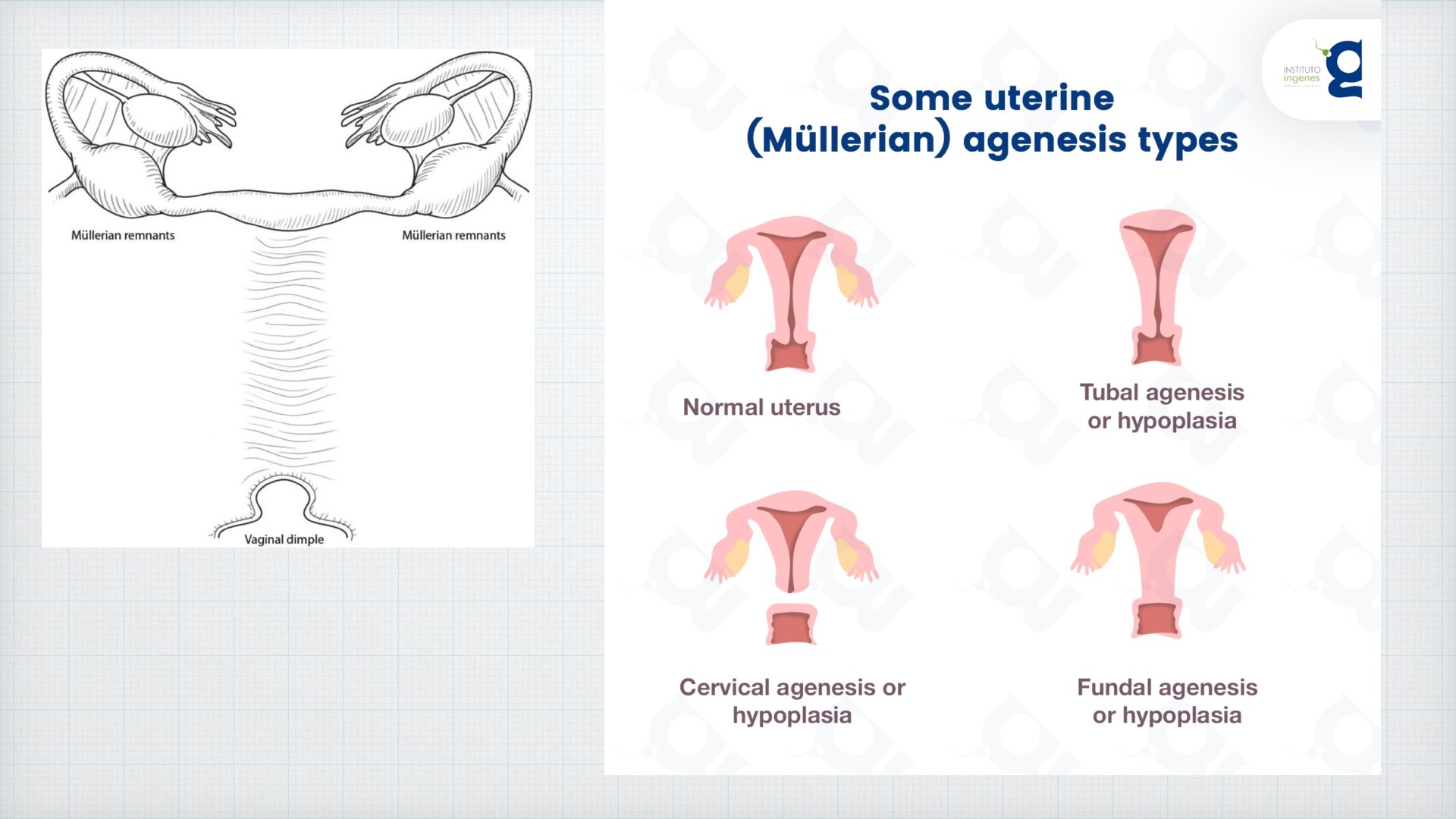
or called Testicular feminization syndrome Mildly")
2 -androgen insensitivity syndrome AIS: ( 46 XY )or called Testicular feminization syndrome Mildly elevated LH and FSH? ? Breast development (with nipples and areolae smaller than. a normal genotypical female‟s) ? ? In these patients the testes secrete normal male amounts of anti -müllerian hormone (AMH); therefore, patients have only a vaginal dimple and no uterus.

Treatment: A- gonadal resection to avoid neoplasia B- creation of a neovagina By: 1 -The Frank method of vaginal dilation 2 -Mc. Indoe vaginoplasty C- Psychological counseling
, after uterine instrumentation like D&C after pregnancy")
3 -Asherman syndrome: intrauterine Normal scarring (synechiae), after uterine instrumentation like D&C after pregnancy termination. should be evaluated by hysterosalpingography or sonohysterography. Tx : Hysteroscopic treatment with excision of the synechiae and normalization of the uterine cavity
 She can’t get")
Ovarian causes 40% : 1 - Agenesis: like Turner syndrome (XO) She can’t get pregnant bcz there’s no ovary But she has hypoplastic uterus FSH and LH ? ! Do karyotype

2 -premature ovarian failure: ovarian failure before the age of 40 years, if it happens before 30 then it may be caused by a chromosomal defect. --> do karyotyping cause of POF: - Ovarian injury as a result of surgery, radiation, or chemotherapy; - Galactosemia - Carrier status of the fragile X syndrome - Treatment : HRT to prevent osteoporosis.

3 -Polycystic ovarian syndrome Will discuss later on
 : Hypersecretion of prolactin leads to gonadal")
Pituitary causes: 1 - Adenoma ( prolactinoma) : Hypersecretion of prolactin leads to gonadal dysfunction by interrupting the secretion of Gn. RH, which inhibits the release of LH and FSH and thereby impairs gonadal steroidogenesis. 50% have radiographic changes in sella tursica 10% of all intracranial tumors. -fasting prolactin, TSH , CT scan - Divided into micro-adenoma( less than 10 mm) or macro-adenoma (more or equal to 10 mm) �we worry about macro size because if it increases in size it may cause additional harm.

2 - empty sella tursica syndrome : the pituitary gland shrinks or becomes flattened, filling the sella turcica with cerebrospinal fluid instead of the normal pituitary. low FSH , LH , other hormones are low except prolactin in beginning but it will decrease Tx: ?

3 - Sheehan syndrome: Postpartum hemorrhage, extensive bleeding may reduce the blood flow to the pituitary gland causing the pituitary cells to be damaged or die (necrosis). Complaining: failure to lactate the baby Tx: hormonal replacement therapy ( thyroxine , cortisol, estrogen , . . . )

Hypothalamus causes 35% 1 -Psychological problem : stress, anxiety , irritability, antidepressant drugs , anorexia nervosa Reversible If no modifiable cause is identified from above —> treat with combined OCPS. Or E 2 skin patches; to reduce osteoporosis and maintain vaginal and breast development.

2 - congenital syndrome: kallmann Syndrome hypogonadotropic hypogonadism Delayed or absent puberty along with an absent / impaired sense of smell Tx: HRT to normalize the sex hormone levels, so as to induce and maintain sexual development.

Thank you ��
- Slides: 27