AMELOBLASTOMA Odontogenic tumors a complex group of lesions

AMELOBLASTOMA

Odontogenic tumors a complex group of lesions of diverse histopathologic types and clinical behavior. true neoplasms Rarely exhibit malignant behavior Tumorlike malformations (hamartomas)

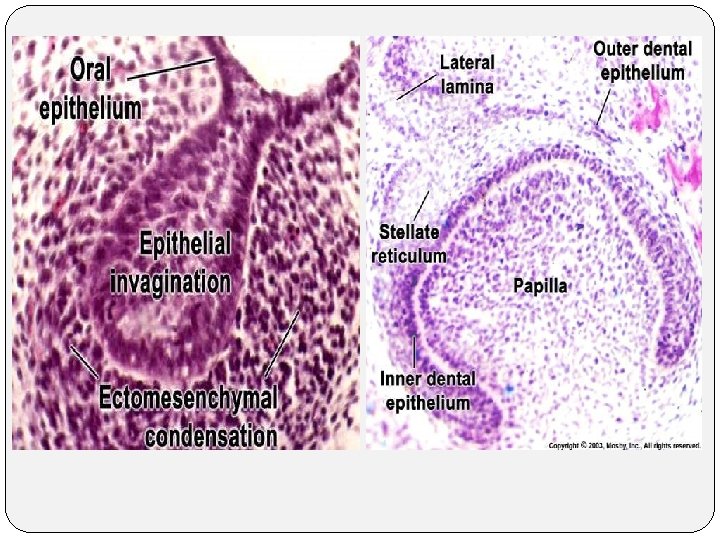
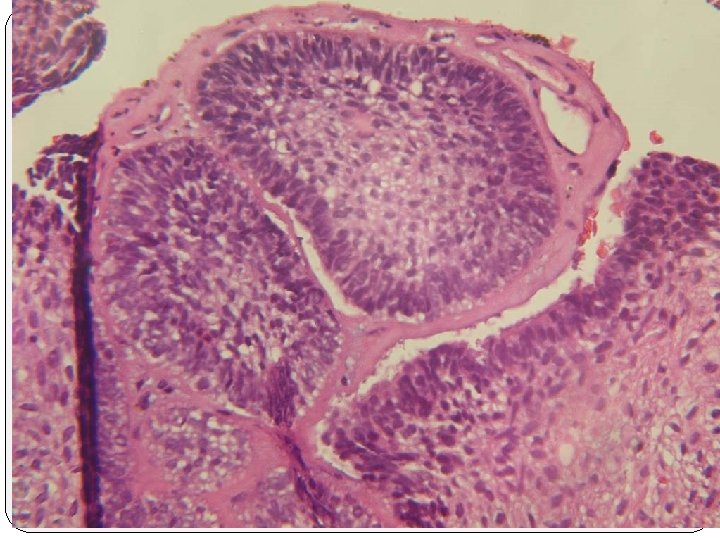
Odontogenic tumors, like normal odontogenesis, demonstrate varying inductive interactions between odontogenic epithelium and odontogenic ectomesenchyme. Oral epithelium Epithelial invagination A C Dental lamina ectomesenchyme B D

Classification of Odontogenic Tumors A. Tumors of odontogenic epithelium 1. Ameloblastoma a. Malignant ameloblastoma b. Ameloblastic carcinoma 2. Clear cell odontogenic carcinoma 3. Adenomatoid odontogenic tumor* 4. Calcifying epithelial odontogenic tumor 5. Squamous odontogenic tumor B. Mixed odontogenic tumors 1. Ameloblastic fibroma 2. Ameloblastic fibro-odontoma 3. Ameloblastic fibrosarcoma 4. Odontoameloblastoma 5. Compound odontoma 6. Complex odontoma C. Tumors of odontogenic ectomesenchyme 1. Odontogenic fibroma 2. Granular cell odontogenic tumor 3. Odontogenic myxoma 4. Cementoblastoma

Tumors of Odontogenic Epithelium are composed of odontogenic epithelium without participation of odontogenic ectomesenchyme. AMELOBLASTOMA the most common clinically significant odontogenic tumor. Its relative frequency equals the combined frequency of all other odontogenic tumors, excluding odontomas Tends to infiltrate between intact cancellous bone trabeculae at the periphery of the lesion before bone resorption becomes radiographically evident. Recurrence often takes many years to become clinically manifest.

rests of dental lamina a developing enamel organ they ma yarise from the epithelial lining of an odontogenic cyst the basal cells of the oral mucosa the epithelial cell rests of Malessez

Ameloblastomas are slow-growing, locally invasive tumors that run a benign course in most cases. Three different clinicoradiographic situations 1)Conventional solid or multicystic (86%) 2)Unicystic (13%) 3)Peripheral (Extraosseous) (1%) differing therapeutic considerations and prognosis.

Conventional solid a wide age range or multicystic Relatively uncommon in the 10 - to 19 -year-old groupequal prevalence in the third to seventh decades of life rare in children younger than age 10 no significant gender predilection Pain and paresthesia are uncommon, even with large tumors. Most often in the molar-ascending ramus area

A painless swelling expansion of the jaw is the usual clinical presentation If untreated, the lesion may grow slowly to massive or grotesque proportions

Radiographic feature Multilocular radiolucent lesion, soap Buccal & lingual cortical expansion resorption of the roots of teeth In many cases an unerupted teeth defect "soap bubble" appearance. bubble / honey combed specially 3 rd molar is associated with "honeycombed" appearance.

Solid ameloblastomas may radiographically appear as unilocular defects, which may resemble almost any type of cystic lesion radiolucent resorption of the roots of teeth irregular scalloping margins. This small unilocular radiolucency lesion be mistaken for a lateral periodontal cyst

Although the radiographic features, particularly of the typical multilocular defect, may be highly suggestive of ameloblastoma a variety of odontogenic and nonodontogenic lesions may show similar radiographic features Odontogenic keratocyst Central giant cell granuloma Ameloblastic fibroma Odontogenic myxoma

Histopathologic Features Follicular II. plexiform I. III. Acanthomatuos IV. granular cell desmoplastic V. VI. The No correlation between clinical behavior and these microscopic patterns basal cell follicular and plexiform patterns are the most common

Follicular pattern Islands of epithelium resemble enamel organ epithelium in a mature fibrous connective tissue stroma a core of loosely arranged angular cells resembling the stellate reticulum of an enamel organ. A single layer of tall columnar ameloblast-like cells or cuboidal that resemble basal cells surrounds this central core. The nuclei of these cells are located at the opposite pole to the basement membrane (reversed polarity) .

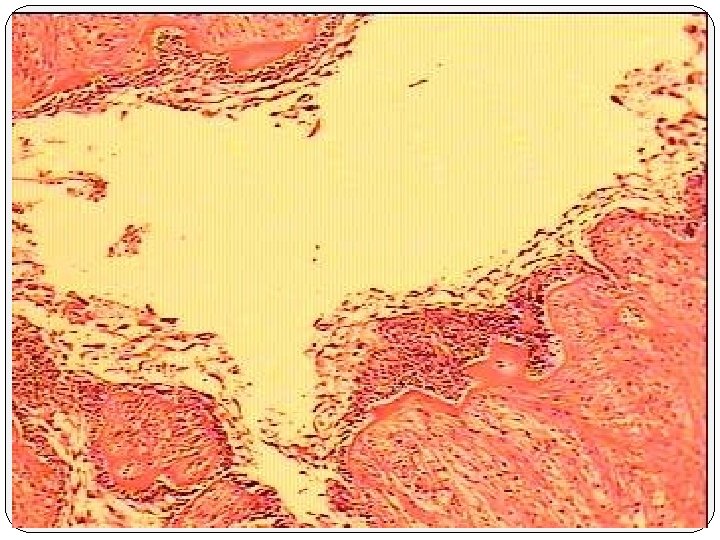
Cyst formation is common and may vary from microcysts, which form within the epithelial islands, to large macroscopic cysts, which may be several centimeters in diameter

Plexiform pattern consists of long, anastomosing cords or larger sheets of odontogenic epithelium columnar or cuboidal ameloblast-like cells surrounding more loosely arranged epithelial cells. The supporting stroma tends to be loosely arranged and vascular. Cyst formation is relatively uncommon. When Cyst formation occurs, it is more often associated with stromal degeneration rather than cystic change within the epithelium

Acanthomatous pattern When extensive squamous metaplasia, often associated with keratin formation, occurs in the central portions of the epithelial islands of a follicular ameloblastoma This change does not indicate a more aggressive course for the lesion.

Islands of ameloblastoma demonstrating central squamous differentiation.

unicystic ameloblastoma

separate consideration clinical features Radiographic features pathologic features its response to treatment 10% to 15% of all intraosseous ameloblastomas Whether the unicystic ameloblastoma originates de nova as a neoplasm or whether it is the result of neoplastic transformation of nonneoplastic cyst epithelium has been long debate.

Clinical and Radiographic Features 50% of all such tumors, diagnosed during the second decade of life More than 90%. . . . in the mandible, ( usually in the posterior regions) Often asymptomatic A circumscribed radiolucency that surrounds the crown of an unerupted mandibular third molar Other tumors simply appear as sharply defined radiolucent areas and are usually considered to be a primordial , radicular, or residual cyst. The surgical findings may also suggest that the lesion in question is a cyst.

Histopathologic Features luminal a fibrous cyst wall l a basal layer of columnar or cuboidal cells with hyperchromatic nuclei reverse polarity and basilar cytoplasmic vacuolization The overlying epithelial cells are loosely cohesive and resemble stellate reticulum

plexiform unicystic ameloblastomas. one or more nodules of ameloblastoma project from the cystic lining into the lumen of the cyst Because the secondary inflammation, The intraluminal cellular proliferation does not always meet the strict histopathologic criteria for ameloblastoma intralumina Typical ameloblastoma, however, may be found in other, less inflamed parts of the specimen.

the fibrous wall of the cyst is infiltrated by typical follicular or plexiform ameloblastoma. multiple sections through many levels of the specimen are necessary to rule out the possibility of mural invasion of tumor cells Mural UAB

Radiographic diff. diagnosis 1. residual cyst 2. okc 3. ameloblastoma

gross features

Subepithelial hyalinization

Squamous differentiation Mural invasion of tumor cells Ameloblastomatous invasion into the underlying mature collagenous connective tissue wall

The End
- Slides: 33